You might also like
- Spicer Kendall - FinalDocument25 pagesSpicer Kendall - Finalapi-611386981No ratings yet
- Local Public Health in Uncertain Times: Julie Morita, MD Commissioner Chicago Department of Public HealthDocument39 pagesLocal Public Health in Uncertain Times: Julie Morita, MD Commissioner Chicago Department of Public HealthNational Press FoundationNo ratings yet
- Chapter Four Result and Findings 4.1: Age of The RespodentDocument13 pagesChapter Four Result and Findings 4.1: Age of The RespodentsareedoNo ratings yet
- JEMM 2022 - Province, District, Health Facility Profile Template Inggris Edit 1Document30 pagesJEMM 2022 - Province, District, Health Facility Profile Template Inggris Edit 1TianKaunangNo ratings yet
- Psoriatic ArthritisDocument8 pagesPsoriatic ArthritisGilia OpreaNo ratings yet
- Multiple Choice Questions: ST RDDocument6 pagesMultiple Choice Questions: ST RDAbdulrab SaeedNo ratings yet
- Page - NBB ResearchDocument41 pagesPage - NBB ResearchToche DoceNo ratings yet
- WHO - HQ - Reports G2 PROD EXT TBFinancingCountryProfileDocument1 pageWHO - HQ - Reports G2 PROD EXT TBFinancingCountryProfileAugie KadunNo ratings yet
- Challenges of Viral Hepatitis Treatment in EthiopiaDocument16 pagesChallenges of Viral Hepatitis Treatment in EthiopiaEleni HagosNo ratings yet
- Pediatric Hiv - Zambia.Document59 pagesPediatric Hiv - Zambia.Linus PuleNo ratings yet
- Diagnostic System For COVID-19 in South Korea: Hyukmin Lee, Prof., M.D., PH.DDocument18 pagesDiagnostic System For COVID-19 in South Korea: Hyukmin Lee, Prof., M.D., PH.DPaolaContrerasMoranNo ratings yet
- MEDCAC Cronenwett PDFDocument37 pagesMEDCAC Cronenwett PDFVladimirTonellodeVasconcelosNo ratings yet
- Epiaid Recs 08022021 EmbargoedDocument58 pagesEpiaid Recs 08022021 EmbargoedJeff MorrisNo ratings yet
- Ending Aids Papua Aids ConferenceDocument48 pagesEnding Aids Papua Aids ConferenceStevanus Bob Arvianto AlwieNo ratings yet
- Clinical Profile of Isolation Ward Patients Amidst Pandemic of Covid-19 in Workshop Hospital Kanchrapara, Eastern Railway & Their ManagementDocument24 pagesClinical Profile of Isolation Ward Patients Amidst Pandemic of Covid-19 in Workshop Hospital Kanchrapara, Eastern Railway & Their ManagementSubhashish DasNo ratings yet
- Hepatitis B in Pregnancy PDFDocument38 pagesHepatitis B in Pregnancy PDFAlsyNo ratings yet
- W2. 01. Introduction - To - Surveillance SerouriDocument53 pagesW2. 01. Introduction - To - Surveillance Serouriع كيف كيفك Dhaif-saeedNo ratings yet
- Prof. Lesmana - The 4th Liv GI Fair PGC On Hepatitis C Evolution of DAA (Direct Acting Antiviral AgentDocument26 pagesProf. Lesmana - The 4th Liv GI Fair PGC On Hepatitis C Evolution of DAA (Direct Acting Antiviral AgentWenny NgawingNo ratings yet
- PUBH151 Lab Exercises W3 Student'sDocument8 pagesPUBH151 Lab Exercises W3 Student'sAbdulqader DawoudNo ratings yet
- NVHD COVID UPDATE July 29 2020Document12 pagesNVHD COVID UPDATE July 29 2020The Valley IndyNo ratings yet
- Mother To Child Transmission HBVDocument48 pagesMother To Child Transmission HBVMuhammad FaisalNo ratings yet
- Vaccinology 2017 Suchada JiamsiriDocument19 pagesVaccinology 2017 Suchada Jiamsirimauricio ramosNo ratings yet
- Dr. Dr. Teguh Triyono, M.Kes., SP - PK (K) - Convalescent Plasma Collection Synchronized With COVID-19 VaccinationDocument23 pagesDr. Dr. Teguh Triyono, M.Kes., SP - PK (K) - Convalescent Plasma Collection Synchronized With COVID-19 VaccinationHairul AnwarNo ratings yet
- Maine ILIweek 2014Document5 pagesMaine ILIweek 2014NEWS CENTER MaineNo ratings yet
- A Boosting Approach For Prostate Cancer Detection Using Multi-Parametric MRIDocument8 pagesA Boosting Approach For Prostate Cancer Detection Using Multi-Parametric MRIareeNo ratings yet
- Meena - Sis - North DakotaDocument71 pagesMeena - Sis - North DakotaRain NakagoNo ratings yet
- Description of Knowledge and Attitude in Control of Blood Pressure On Hypertension Patients in Nanggalo Community Health Clinic Padang in 2016Document21 pagesDescription of Knowledge and Attitude in Control of Blood Pressure On Hypertension Patients in Nanggalo Community Health Clinic Padang in 2016zenezaNo ratings yet
- 11 January 2021: RT PCR Lab: 114 Genexpert Lab: 27 Rapid Antigen: 40Document8 pages11 January 2021: RT PCR Lab: 114 Genexpert Lab: 27 Rapid Antigen: 40Abir HabibNo ratings yet
- HCV Elimination in Pwids and The IncarceratedDocument60 pagesHCV Elimination in Pwids and The IncarceratedntnquynhproNo ratings yet
- Hepatitis A: Key ChangesDocument16 pagesHepatitis A: Key ChangesDanesa MadoNo ratings yet
- Clinical Development Programs For Chronic Idiopathic Urticaria Indication For H1-AntihistaminesDocument23 pagesClinical Development Programs For Chronic Idiopathic Urticaria Indication For H1-AntihistaminesfadlNo ratings yet
- Ppra Snars I Dr. DewiDocument93 pagesPpra Snars I Dr. DewiNilam atika sariNo ratings yet
- HTN Slide Deck NewDocument27 pagesHTN Slide Deck NewChristy BerryNo ratings yet
- Review Article: Endocrine-Disrupting Chemicals: Associated Disorders and Mechanisms of ActionDocument53 pagesReview Article: Endocrine-Disrupting Chemicals: Associated Disorders and Mechanisms of ActionFabiana PassamaniNo ratings yet
- BPH QuestionDocument20 pagesBPH QuestionChaithra BvinodNo ratings yet
- Oet Materials 2Document201 pagesOet Materials 2jojan100% (3)
- Novel Coronavirus (COVID-19) : Updates For Clinicians: September 4, 2020Document44 pagesNovel Coronavirus (COVID-19) : Updates For Clinicians: September 4, 2020Mahita SainiNo ratings yet
- Hand Hygine Guideline WHODocument6 pagesHand Hygine Guideline WHORiriz AfiantoNo ratings yet
- ABSTRACTDocument7 pagesABSTRACTSudha SathishNo ratings yet
- Global Dan Nasional Problem AMR 2019Document36 pagesGlobal Dan Nasional Problem AMR 2019DewiNo ratings yet
- Article eDocument17 pagesArticle eSaad ShafiqNo ratings yet
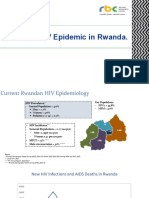
- State of HIV Epidemic in RwandaDocument17 pagesState of HIV Epidemic in RwandaNshimiyimana Jean ClaudeNo ratings yet
- Ab OperasiDocument28 pagesAb OperasiFarmasi RSUD Kramat JatiNo ratings yet
- High Alert Medications 2018Document30 pagesHigh Alert Medications 2018Eman MohamedNo ratings yet
- CCO COVID19 Resources Center Diagnosis Transmission SlidesDocument64 pagesCCO COVID19 Resources Center Diagnosis Transmission SlidesYoshimuneNo ratings yet
- Report COVID Clinical ManagmentDocument70 pagesReport COVID Clinical ManagmentJeevan Emmanual JoyNo ratings yet
- Mm7019e1 HDocument5 pagesMm7019e1 HworksheetbookNo ratings yet
- Medication Error Analysis 2020Document30 pagesMedication Error Analysis 2020sanisani1020No ratings yet
- 2066721labtest Id1675Document4 pages2066721labtest Id1675idark0720No ratings yet
- Challenges in VH Treatment: Fmoh 2021Document17 pagesChallenges in VH Treatment: Fmoh 2021Eleni HagosNo ratings yet
- Jurnal 1Document10 pagesJurnal 1Muhammad SalehNo ratings yet
- Mother To Child Transmission HBVDocument48 pagesMother To Child Transmission HBVAyu Andini Putri100% (1)
- The Israeli Healthcare SystemDocument23 pagesThe Israeli Healthcare SystemNikhil TyagiNo ratings yet
- Acute Viral HepatitisDocument76 pagesAcute Viral HepatitisSaurabh SagunNo ratings yet
- Daily Update Report - August 18 2020Document14 pagesDaily Update Report - August 18 2020The Valley IndyNo ratings yet
- EJMCM - Volume 7 - Issue 11 - Pages 5263-5268Document6 pagesEJMCM - Volume 7 - Issue 11 - Pages 5263-5268Nabila RizkikaNo ratings yet
- Project EnglishDocument3 pagesProject EnglishEries GunaNo ratings yet
- Regulated Bioanalytical Laboratories: Technical and Regulatory Aspects from Global PerspectivesFrom EverandRegulated Bioanalytical Laboratories: Technical and Regulatory Aspects from Global PerspectivesNo ratings yet
- Laboratory Total Quality Management for Practitioners and Students of Medical Laboratory ScienceFrom EverandLaboratory Total Quality Management for Practitioners and Students of Medical Laboratory ScienceRating: 5 out of 5 stars5/5 (3)
- Icu Fluids JCDocument3 pagesIcu Fluids JCapi-611386981No ratings yet
- Patient Case - Vpa ToxicityDocument13 pagesPatient Case - Vpa Toxicityapi-611386981No ratings yet
- Journal Club - Bezlotoxumab 12-Month Modify IIDocument15 pagesJournal Club - Bezlotoxumab 12-Month Modify IIapi-611386981No ratings yet
- Patient Case - HyponatremiaDocument14 pagesPatient Case - Hyponatremiaapi-611386981No ratings yet
- Kendall Spicer CVDocument4 pagesKendall Spicer CVapi-611386981No ratings yet
- EFFECTS OF VOLCANIC ERUPTION - PPSXDocument19 pagesEFFECTS OF VOLCANIC ERUPTION - PPSXMyla Balingit AdiNo ratings yet
- Stephane Moses The Angel of History Rosenzweig Benjamin Scholem PDFDocument196 pagesStephane Moses The Angel of History Rosenzweig Benjamin Scholem PDFlivehuman100% (3)
- القطع بالبلازماDocument27 pagesالقطع بالبلازماsamehNo ratings yet
- Coronary Stents: Current StatusDocument42 pagesCoronary Stents: Current StatusMANSI SALUNKENo ratings yet
- Rangtong Shentong ViewDocument19 pagesRangtong Shentong Viewlongjim31100% (1)
- 5980 10143 1 SM PDFDocument11 pages5980 10143 1 SM PDFfaustinaNo ratings yet
- Designing Hopping Animal PDFDocument3 pagesDesigning Hopping Animal PDFAntonio Francisco Muñoz100% (1)
- Lord Kuthumi - Dolphins SpeakDocument8 pagesLord Kuthumi - Dolphins SpeakEmeraldRay0% (1)
- Practice Tests - Tiếng Anh 7 I-learn Smart World TestDocument9 pagesPractice Tests - Tiếng Anh 7 I-learn Smart World TestnghiepNo ratings yet
- The Symbols Found in TarotDocument17 pagesThe Symbols Found in TarotPEdro100% (1)
- Baño - Griferia - KOHLER - K-74013M+0.50GPMDocument3 pagesBaño - Griferia - KOHLER - K-74013M+0.50GPMGiordano Tuanama YapoNo ratings yet
- Method Statement For Boom Barrier Installation (Rev00) ELV2Document38 pagesMethod Statement For Boom Barrier Installation (Rev00) ELV2balajiNo ratings yet
- Auxiliary Fire Service: William (Far Right) c1942Document3 pagesAuxiliary Fire Service: William (Far Right) c1942api-25925381No ratings yet
- Blender To Google EarthDocument41 pagesBlender To Google Earthrichx7No ratings yet
- 5100 NSL (User's Guide) PDFDocument40 pages5100 NSL (User's Guide) PDFJEREMEE MICHAEL TYLERNo ratings yet
- Quiz13 130630200754 Phpapp02Document10 pagesQuiz13 130630200754 Phpapp02anukrititiwaNo ratings yet
- Review Questions UAPGADocument28 pagesReview Questions UAPGAkarenNo ratings yet
- Five Hour Baby Boy Sweater PDFDocument2 pagesFive Hour Baby Boy Sweater PDFOana DabijaNo ratings yet
- Interzinc 2280 Product BrochureDocument4 pagesInterzinc 2280 Product BrochureAshish Raul CIENo ratings yet
- Documentation ExamplesDocument5 pagesDocumentation ExamplesErika HarveryNo ratings yet
- Hebrew and TamilDocument98 pagesHebrew and TamilSreshta JustinNo ratings yet
- Elements of HardscapingDocument57 pagesElements of HardscapingNathar ShaNo ratings yet
- Inhalation AnestheticsDocument27 pagesInhalation AnestheticsMarcelitaTaliaDuwiriNo ratings yet
- Introduction On Photogrammetry Paul R WolfDocument33 pagesIntroduction On Photogrammetry Paul R Wolfadnan yusufNo ratings yet
- Geotechnical Laboratory: Open-Ended LabDocument7 pagesGeotechnical Laboratory: Open-Ended LabNoorshahira Md IsaNo ratings yet
- Wahabism - Bala SurajoDocument17 pagesWahabism - Bala SurajoAbu Muhammad50% (2)
- GENII - Nissan Patrol GQ & GU - RE4 4 Speed Diesel & Petrol - Lock Up Instructions-1Document14 pagesGENII - Nissan Patrol GQ & GU - RE4 4 Speed Diesel & Petrol - Lock Up Instructions-1Trav GilesNo ratings yet
- SBB Product NoteDocument3 pagesSBB Product NoteFilipe MartinsNo ratings yet
- Tech Brief 3: Digitally Control Phase Shift: Application Note 559Document6 pagesTech Brief 3: Digitally Control Phase Shift: Application Note 559Sreerag Kunnathu SugathanNo ratings yet
- 4864.21 - Optics System 2Document39 pages4864.21 - Optics System 2Edgar Jose Aponte MartinezNo ratings yet