You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- GMT 95 LUR 1995 GM Light Duty Truck Unit Repair Manual PDFDocument790 pagesGMT 95 LUR 1995 GM Light Duty Truck Unit Repair Manual PDFhidraulic50% (2)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Handout IV: DSM-5 ASD Checklist: Making An Autism Spectrum Disorder DiagnosisDocument2 pagesHandout IV: DSM-5 ASD Checklist: Making An Autism Spectrum Disorder DiagnosisValentina IerotheouNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- DOPE Personality TestDocument8 pagesDOPE Personality TestMohammed Hisham100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- GSM Network SDCCH Congestion & Solutions-16Document15 pagesGSM Network SDCCH Congestion & Solutions-16abdullaaNo ratings yet
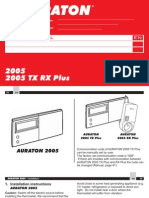
- Auraton 2005Document24 pagesAuraton 2005Muhidin KozicaNo ratings yet
- Icp-Aes S1Document57 pagesIcp-Aes S1fitriana dewi kurniawatiNo ratings yet
- Using SSPC Coating Material Standards 1Document18 pagesUsing SSPC Coating Material Standards 1achusanachu100% (1)
- Milgram's Obedience To Authority: Its Origins, Controversies, and ReplicationsDocument32 pagesMilgram's Obedience To Authority: Its Origins, Controversies, and ReplicationsnabilahbilqisNo ratings yet
- Tingkat Pengetahuan HerawatiDocument7 pagesTingkat Pengetahuan HerawatinabilahbilqisNo ratings yet
- Adhrence 1Document9 pagesAdhrence 1nabilahbilqisNo ratings yet
- Pathania 2019Document20 pagesPathania 2019nabilahbilqisNo ratings yet
- Katigbak 2018Document9 pagesKatigbak 2018nabilahbilqisNo ratings yet
- Oup Accepted Manuscript 2021Document19 pagesOup Accepted Manuscript 2021nabilahbilqisNo ratings yet
- Avor Tri 2019Document6 pagesAvor Tri 2019nabilahbilqisNo ratings yet
- Psychology of Sport and Exercise: Changiz Mohiyeddini, Regina Pauli, Stephanie BauerDocument9 pagesPsychology of Sport and Exercise: Changiz Mohiyeddini, Regina Pauli, Stephanie BauernabilahbilqisNo ratings yet
- Intention and AttitudeDocument9 pagesIntention and AttitudenabilahbilqisNo ratings yet
- A Security Risk Perception Model For The Adoption of MobileDocument25 pagesA Security Risk Perception Model For The Adoption of MobilenabilahbilqisNo ratings yet
- Papies 2017Document19 pagesPapies 2017nabilahbilqisNo ratings yet
- Journal Pre-Proofs: Food Quality and PreferenceDocument33 pagesJournal Pre-Proofs: Food Quality and PreferencenabilahbilqisNo ratings yet
- ComplianceDocument11 pagesCompliancenabilahbilqisNo ratings yet
- Jurnal PromkesDocument14 pagesJurnal PromkesnabilahbilqisNo ratings yet
- Behaviour & Information Technology: Click For UpdatesDocument16 pagesBehaviour & Information Technology: Click For UpdatesnabilahbilqisNo ratings yet
- Jurnal PentingDocument11 pagesJurnal PentingnabilahbilqisNo ratings yet
- Attitude, KnowledgeDocument7 pagesAttitude, KnowledgenabilahbilqisNo ratings yet
- HIV Retesting of HIV-Negative Pregnant Women in The Context of Prevention of Mother-to-Child Transmission of HIV in Primary Health Centers in Rural Zambia: What Did We Learn?Document6 pagesHIV Retesting of HIV-Negative Pregnant Women in The Context of Prevention of Mother-to-Child Transmission of HIV in Primary Health Centers in Rural Zambia: What Did We Learn?nabilahbilqisNo ratings yet
- AwarnesDocument6 pagesAwarnesnabilahbilqisNo ratings yet
- 2018 Article 708Document7 pages2018 Article 708nabilahbilqisNo ratings yet
- Exploring The Association Between Multimorbidity and Cognitive Impairment in Older Adults Living in The Community: A Review of The LiteratureDocument11 pagesExploring The Association Between Multimorbidity and Cognitive Impairment in Older Adults Living in The Community: A Review of The LiteraturenabilahbilqisNo ratings yet
- Antenatal Care and Uptake of HIV Testing Among Pregnant Women in Sub-Saharan Africa: A Cross-Sectional StudyDocument10 pagesAntenatal Care and Uptake of HIV Testing Among Pregnant Women in Sub-Saharan Africa: A Cross-Sectional StudynabilahbilqisNo ratings yet
- Economic Systematic ReviewDocument12 pagesEconomic Systematic ReviewnabilahbilqisNo ratings yet
- 10 Tips To Fight Headache PainDocument2 pages10 Tips To Fight Headache PainPurushotham KumarNo ratings yet
- Anti-Violence Against Women and Their Children Act of 2004 (Republic Act No. 9262)Document5 pagesAnti-Violence Against Women and Their Children Act of 2004 (Republic Act No. 9262)Tobythe BullyNo ratings yet
- Kunft KDW4752N DishwasherDocument59 pagesKunft KDW4752N Dishwashermike_sanNo ratings yet
- Case Session - 5Document3 pagesCase Session - 5Ruthwick GowdaNo ratings yet
- Nitrox Tablice!Document6 pagesNitrox Tablice!Frane AsanovićNo ratings yet
- Diabettes Mellitus and Cognitive ImpairmentsDocument12 pagesDiabettes Mellitus and Cognitive ImpairmentsPutri YunandaNo ratings yet
- COMEDK UGET-2011 Medical Rank ListDocument147 pagesCOMEDK UGET-2011 Medical Rank ListiamvarkeyNo ratings yet
- Lesson 14 Reference Notes Class 10Document3 pagesLesson 14 Reference Notes Class 10Seetha Lekshmi KishoreNo ratings yet
- Bkf1243-Analytical Chemistry 21314 PDFDocument9 pagesBkf1243-Analytical Chemistry 21314 PDFrushdiNo ratings yet
- MDR - Conformity AssessmentDocument8 pagesMDR - Conformity AssessmentNathan LabordeNo ratings yet
- MBA 504 Ch3 SolutionsDocument22 pagesMBA 504 Ch3 SolutionsMohit Kumar GuptaNo ratings yet
- Anesthesia: Essays and Researches General Anesthesia in Tetanus Patient Undergoing Emergency Surgery: A Challenge For AnesthesiologistDocument4 pagesAnesthesia: Essays and Researches General Anesthesia in Tetanus Patient Undergoing Emergency Surgery: A Challenge For AnesthesiologistEnrico StefanelliNo ratings yet
- Transition Metal ChemistryDocument15 pagesTransition Metal Chemistryswc306No ratings yet
- Daftar Pustaka PDFDocument7 pagesDaftar Pustaka PDFaulia rahmiNo ratings yet
- Pharmaceutical QualityDocument4 pagesPharmaceutical Qualityziauddin bukhariNo ratings yet
- Golf Pei Course Comparison ChartDocument1 pageGolf Pei Course Comparison ChartSteve DimondNo ratings yet
- MSP Duct Installation ManualDocument48 pagesMSP Duct Installation ManualPablo DenisNo ratings yet
- Chemistry Mar 2009 EngDocument8 pagesChemistry Mar 2009 EngPrasad C M100% (1)
- Hildegard PeplauDocument7 pagesHildegard PeplauCarmenchuParraNo ratings yet
- 300 SS TigDocument10 pages300 SS TigSameer KhanNo ratings yet
- Water ProofingDocument5 pagesWater ProofingMalith De SilvaNo ratings yet
- 7 Advertising - AirDocument1 page7 Advertising - Airaletzring@innovectra.comNo ratings yet
- Arterial CatheterizationDocument5 pagesArterial CatheterizationSREEDEVI T SURESHNo ratings yet