You might also like
- History and Biodata of Anxiety PatientDocument16 pagesHistory and Biodata of Anxiety PatientannuNo ratings yet
- Case Study 2 (PTSD)Document12 pagesCase Study 2 (PTSD)Atul MishraNo ratings yet
- PNEUMONIA Case 2 PDFDocument49 pagesPNEUMONIA Case 2 PDFRed OrangeNo ratings yet
- Preterm birth case study at Lira Regional Referral HospitalDocument11 pagesPreterm birth case study at Lira Regional Referral HospitalIrahuka CliftonNo ratings yet
- DENGUEDocument21 pagesDENGUEHikari 光 ShidouNo ratings yet
- Everything You Need to Know About DiarrheaDocument15 pagesEverything You Need to Know About DiarrheaAlmaRisaFitrianaNo ratings yet
- Case Study-TrichotilomaniaDocument34 pagesCase Study-TrichotilomaniaMonikaNo ratings yet
- Case Study On IBDDocument41 pagesCase Study On IBDchampaNo ratings yet
- Case Study 2Document29 pagesCase Study 2falguni mondalNo ratings yet
- Refractive ErrorDocument6 pagesRefractive Errortri erdiansyahNo ratings yet
- 1st Yr ANM Oral Practical Regular Exam Scheudule 21-22-08.02.2023Document237 pages1st Yr ANM Oral Practical Regular Exam Scheudule 21-22-08.02.2023Mrs NobodyNo ratings yet
- Journal Homepage: - : Manuscript HistoryDocument10 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- Nutritional AsthaDocument30 pagesNutritional AsthaSwati SharmaNo ratings yet
- Care Plan-Otitis NewDocument33 pagesCare Plan-Otitis NewSUNIL KUMARNo ratings yet
- Physical Assessment Skin & Integument FindingsDocument9 pagesPhysical Assessment Skin & Integument FindingsmeowzartNo ratings yet
- Anti PsychoticsDocument20 pagesAnti Psychoticschetan1uips100% (1)
- Nurs702 Critique Final2Document9 pagesNurs702 Critique Final2natalie nodayNo ratings yet
- BSc Nursing Curriculum at AIIMS BhopalDocument141 pagesBSc Nursing Curriculum at AIIMS Bhopalvikash kumarNo ratings yet
- Health TalkDocument19 pagesHealth TalkRubban HashmiNo ratings yet
- Psychoactive Substances and Home Care Management, Amit TamboliDocument7 pagesPsychoactive Substances and Home Care Management, Amit TamboliAmit TamboliNo ratings yet
- A Descriptive Study To Assess The Knowledge and Attitude Regarding Use of Emergency Contraceptive Pills As A Method of Contraception Among Female Staff Nurses of Rajindera Hospital PatialaDocument29 pagesA Descriptive Study To Assess The Knowledge and Attitude Regarding Use of Emergency Contraceptive Pills As A Method of Contraception Among Female Staff Nurses of Rajindera Hospital PatialaEditor IJTSRDNo ratings yet
- ANATOMY and PHYSIOLOGY of CHRONIC OTITIS MEDIA-GCS Sa MED - ANNEX-maam ValezaDocument36 pagesANATOMY and PHYSIOLOGY of CHRONIC OTITIS MEDIA-GCS Sa MED - ANNEX-maam ValezaBonieve Pitogo NoblezadaNo ratings yet
- New Born Case StudyDocument4 pagesNew Born Case StudyErick SanangaNo ratings yet
- Care Plans-Cholelithiasis NewDocument14 pagesCare Plans-Cholelithiasis NewSUNIL KUMARNo ratings yet
- QP CODE: 2101: Section - A, AnatomyDocument122 pagesQP CODE: 2101: Section - A, AnatomyMeghanaNo ratings yet
- BPAD Lesson PlanDocument47 pagesBPAD Lesson PlanNoonu ChettriNo ratings yet
- Case No 1 ClinicalDocument7 pagesCase No 1 ClinicalSarah Saqib AhmadNo ratings yet
- Seminar On PhilosophyDocument37 pagesSeminar On Philosophymalleshwari athramNo ratings yet
- Curriculum Planning PBBSC Second Year Mental Health NursingDocument8 pagesCurriculum Planning PBBSC Second Year Mental Health NursingSAGAR ADHAONo ratings yet
- Syllab Abus and Regulations NS: P Post Basic B.Sc. NursingDocument4 pagesSyllab Abus and Regulations NS: P Post Basic B.Sc. NursingmuthukumarNo ratings yet
- For PDFDocument128 pagesFor PDFHermin TorresNo ratings yet
- Respiratory Disorders Case StudyDocument4 pagesRespiratory Disorders Case StudyPremiums of the RoseNo ratings yet
- Patient Profile and History of Acute Coronary SyndromeDocument32 pagesPatient Profile and History of Acute Coronary SyndromenidhiNo ratings yet
- Master Rotation 4 M.Sc.Document1 pageMaster Rotation 4 M.Sc.MadhuNo ratings yet
- M.S.E. AlcoholDocument10 pagesM.S.E. AlcoholWillsun BhagatNo ratings yet
- Insulin and Oral Hypoglycemic DrugsDocument45 pagesInsulin and Oral Hypoglycemic DrugsRamadi PrameelaNo ratings yet
- Article Requirement Pedia ListDocument9 pagesArticle Requirement Pedia ListAnita Singh100% (1)
- Definition:: EpilepsyDocument7 pagesDefinition:: EpilepsyNinia MNo ratings yet
- Case Study 3 (Eating Disorder)Document11 pagesCase Study 3 (Eating Disorder)Atul MishraNo ratings yet
- N Research 06.05.2020 Graphical Representation of DataDocument50 pagesN Research 06.05.2020 Graphical Representation of DataBalasakthiNo ratings yet
- Psychiatry Case StudyDocument21 pagesPsychiatry Case StudyJimmy MainaNo ratings yet
- Nursing Process SchizophreniaDocument9 pagesNursing Process SchizophreniaannuNo ratings yet
- EpidiascopeDocument6 pagesEpidiascoperumasadraunaNo ratings yet
- Case Study On MiDocument26 pagesCase Study On MiShikha Thakur100% (1)
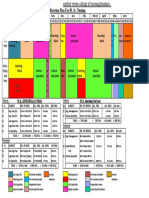
- Clinical rotation plan for B.Sc Nursing 4th year studentsDocument1 pageClinical rotation plan for B.Sc Nursing 4th year studentsMadhuNo ratings yet
- Case Presentation On Multiple SclerosisDocument19 pagesCase Presentation On Multiple SclerosisAayushi SrivastavaNo ratings yet
- Hypothyroidism Guide: Causes, Symptoms and TreatmentDocument11 pagesHypothyroidism Guide: Causes, Symptoms and TreatmentFarhat KhanNo ratings yet
- Identification Data: A. Past Medical HistoryDocument12 pagesIdentification Data: A. Past Medical HistoryPrernaSharmaNo ratings yet
- Cerebral PalsyDocument13 pagesCerebral PalsyAnsu MaliyakalNo ratings yet
- Final Hernioplasty Compilation RevisedDocument58 pagesFinal Hernioplasty Compilation RevisedRaidis PangilinanNo ratings yet
- Dengue FeverDocument8 pagesDengue FeverJay MagsaysayNo ratings yet
- Case Study ExampleDocument46 pagesCase Study ExampleDerick PaguiriganNo ratings yet
- Clinical Rotation Plan For M.SC Nsg. 1st Year 2018 19 1Document10 pagesClinical Rotation Plan For M.SC Nsg. 1st Year 2018 19 1MadhuNo ratings yet
- Case PresentationDocument33 pagesCase PresentationPratima ThakurNo ratings yet
- Health Assessment 2Document9 pagesHealth Assessment 2Mandira NagNo ratings yet
- Long Case - Susilowati (En Lokal)Document17 pagesLong Case - Susilowati (En Lokal)Hendra WardhanaNo ratings yet
- Preventive Measures of ARIDocument4 pagesPreventive Measures of ARIrittika dasNo ratings yet
- Ocd MseDocument8 pagesOcd MseGogs Ediza AlejoNo ratings yet
- MS Eent (Nle)Document3 pagesMS Eent (Nle)Maginalyn CangasNo ratings yet
- Case in Herniorraphy BESTCASEDocument23 pagesCase in Herniorraphy BESTCASEAdrian MallarNo ratings yet
- Clinical Decision Making in Mental Health Practice Chapter 1 SampleDocument19 pagesClinical Decision Making in Mental Health Practice Chapter 1 SampleRanusha AnushaNo ratings yet
- Types and Symptoms of Common Psychiatric DisordersDocument6 pagesTypes and Symptoms of Common Psychiatric DisordersRanusha AnushaNo ratings yet
- Teaching Clinical Decision MakingDocument34 pagesTeaching Clinical Decision MakingRanusha AnushaNo ratings yet
- Siadh Diabetes Insipidus Acute Renal Failure Chronic Renal FailureDocument6 pagesSiadh Diabetes Insipidus Acute Renal Failure Chronic Renal FailureRanusha AnushaNo ratings yet
- The Silent PandemicDocument11 pagesThe Silent PandemicRanusha AnushaNo ratings yet
- Mental Health Problems Faced by Healthcare WorkersDocument14 pagesMental Health Problems Faced by Healthcare WorkersRanusha AnushaNo ratings yet
- Clinical Decision Making in Mental Health Practice Chapter 1 SampleDocument19 pagesClinical Decision Making in Mental Health Practice Chapter 1 SampleRanusha AnushaNo ratings yet
- State The Psychological Impact of Pandemic Covid - 19 Generalized Anxiety Disorder (GAD)Document3 pagesState The Psychological Impact of Pandemic Covid - 19 Generalized Anxiety Disorder (GAD)Ranusha AnushaNo ratings yet
- NBNC2603 CP Psychiatric Mental Health Nursing - COURSE KITDocument31 pagesNBNC2603 CP Psychiatric Mental Health Nursing - COURSE KITRanusha AnushaNo ratings yet
- Case Study Renal 1Document43 pagesCase Study Renal 1Ranusha AnushaNo ratings yet
- Acute Renal Failure Nursing Care PlanDocument15 pagesAcute Renal Failure Nursing Care PlanRanusha AnushaNo ratings yet
- Schizophrenia Case StudyDocument14 pagesSchizophrenia Case Studyapi-593859653No ratings yet
- Schizophrenia Clinical Case StudyDocument13 pagesSchizophrenia Clinical Case Studyapi-497473260100% (1)
- Assignemet RenalDocument16 pagesAssignemet RenalRanusha AnushaNo ratings yet
- Schizophrenia Case StudyDocument8 pagesSchizophrenia Case StudyJohn Carlo Toledo0% (1)
- Schizophrenia Care Plan RNDocument8 pagesSchizophrenia Care Plan RNRanusha AnushaNo ratings yet
- Schizophrenia NCMH Case StudyDocument41 pagesSchizophrenia NCMH Case StudyJohn Crisostomo89% (36)
- Schizophrenia CaseDocument14 pagesSchizophrenia CaseRanusha AnushaNo ratings yet
- A Case Study On SchizophreniaDocument11 pagesA Case Study On SchizophreniaRosa Isabel57% (7)
- Bipolar Case StudyDocument45 pagesBipolar Case StudyRanusha AnushaNo ratings yet
- Case Study On SchizophreniaDocument21 pagesCase Study On SchizophreniaRanusha Anusha100% (1)
- Case Study Renal 1Document43 pagesCase Study Renal 1Ranusha AnushaNo ratings yet
- Nursing Care Plan For Patient With Renal FailureDocument18 pagesNursing Care Plan For Patient With Renal FailureRanusha AnushaNo ratings yet
- Nursing Care Plan - SchizophreniaDocument3 pagesNursing Care Plan - SchizophreniaJasmin Jacob76% (46)
- Schizophrenia Case StudyDocument8 pagesSchizophrenia Case StudyJohn Carlo Toledo0% (1)
- Sultanate of Oman Ministry of Health Directorate General of Education & Training Al-Dhahira Nursing InistituteDocument31 pagesSultanate of Oman Ministry of Health Directorate General of Education & Training Al-Dhahira Nursing InistituteRanusha AnushaNo ratings yet
- Reflective JournalDocument3 pagesReflective Journalapi-302591810100% (6)
- Teaching Clinical Decision MakingDocument34 pagesTeaching Clinical Decision MakingRanusha AnushaNo ratings yet
- Acute Renal Failure Nursing Care PlanDocument15 pagesAcute Renal Failure Nursing Care PlanRanusha AnushaNo ratings yet
- The Silent PandemicDocument11 pagesThe Silent PandemicRanusha AnushaNo ratings yet
- Cucs 016 13 PDFDocument16 pagesCucs 016 13 PDFAnonymous SlyvspdBNo ratings yet
- Coding deCoding class insightsDocument18 pagesCoding deCoding class insightsShalabh Vikram SahuNo ratings yet
- Compare and Contrast History EssayDocument9 pagesCompare and Contrast History EssayGiselle PosadaNo ratings yet
- Dead Reckoning and Estimated PositionsDocument20 pagesDead Reckoning and Estimated Positionscarteani100% (1)
- I. VHF CommunicationsDocument12 pagesI. VHF CommunicationsSamuel OyelowoNo ratings yet
- Iag Narrative ReportDocument16 pagesIag Narrative ReportHoely SaintNo ratings yet
- Envi. Data AcquisitionDocument10 pagesEnvi. Data AcquisitionDexter John Gomez JomocNo ratings yet
- Kendriya Vidyalaya Sangathan: Observation & ReportingDocument6 pagesKendriya Vidyalaya Sangathan: Observation & ReportingSravan KumarNo ratings yet
- Philippine School Action Plan for Scouting ProgramDocument1 pagePhilippine School Action Plan for Scouting ProgramLaira Joy Salvador - ViernesNo ratings yet
- Festivals WorksheetDocument8 pagesFestivals WorksheetlurdesNo ratings yet
- 65-1-3-D MathematicsDocument8 pages65-1-3-D MathematicsRohan YadavNo ratings yet
- Lecture Notes in Computer Science-7Document5 pagesLecture Notes in Computer Science-7Arun SasidharanNo ratings yet
- Galloway 1989 Genetic Stratigraphic Sequence Basin Analysis IDocument18 pagesGalloway 1989 Genetic Stratigraphic Sequence Basin Analysis IMitreNo ratings yet
- Haven, Quantum Social ScienceDocument306 pagesHaven, Quantum Social ScienceMichael H. HejaziNo ratings yet
- Lucky TextileDocument5 pagesLucky TextileSaim Bin RashidNo ratings yet
- DBMS Notes For BCADocument9 pagesDBMS Notes For BCAarndm8967% (6)
- Prepare Egg Dishes GuideDocument5 pagesPrepare Egg Dishes GuideRuth CesistaNo ratings yet
- TR 101 - Issue 2Document101 pagesTR 101 - Issue 2ergismiloNo ratings yet
- Ground Penetrating Radar For Locating Buried Utilities: Operation ManualDocument75 pagesGround Penetrating Radar For Locating Buried Utilities: Operation ManualArmando BiringkanaeNo ratings yet
- Class of 2016 Graduate ListsDocument16 pagesClass of 2016 Graduate ListscallertimesNo ratings yet
- Section 5: Finite Volume Methods For The Navier Stokes EquationsDocument27 pagesSection 5: Finite Volume Methods For The Navier Stokes EquationsUmutcanNo ratings yet
- Case Study - Steel Works, Inc.Document5 pagesCase Study - Steel Works, Inc.Tayyab UllahNo ratings yet
- Literature Review On OscilloscopeDocument5 pagesLiterature Review On Oscilloscopedhjiiorif100% (1)
- Paratech Brochures RSSDocument12 pagesParatech Brochures RSSTatiana Andrea Carvajal GutierrezNo ratings yet
- NES 362 Type and Production Testing of Mechanical Equipment Category 3Document36 pagesNES 362 Type and Production Testing of Mechanical Equipment Category 3JEORJENo ratings yet
- Google Book Search project makes public domain texts discoverable onlineDocument456 pagesGoogle Book Search project makes public domain texts discoverable onlineVladoMihojevićNo ratings yet
- TCS L6 ActsDocument7 pagesTCS L6 ActsBhebz Erin MaeNo ratings yet
- Y10 ICT End of TermDocument7 pagesY10 ICT End of TermIvy Atuhairwe BisoborwaNo ratings yet
- Louis Moreau Gottschalk's Pan-American Symphonic Ideal-SHADLEDocument30 pagesLouis Moreau Gottschalk's Pan-American Symphonic Ideal-SHADLERafaelNo ratings yet
- ATPL theory summary formulas and guidelines (40 charactersDocument60 pagesATPL theory summary formulas and guidelines (40 charactersJonas Norvidas50% (2)