You might also like
- Themes in Romeo and JulietDocument7 pagesThemes in Romeo and JulietChiosa AdinaNo ratings yet
- Nursing Documentation: Practice SupportDocument24 pagesNursing Documentation: Practice SupportDr Magda Bayoumi60% (5)
- Essene Moses Ten CommandmentsDocument4 pagesEssene Moses Ten Commandmentsjeryon91No ratings yet
- Guide Clinical Audit LeadsDocument40 pagesGuide Clinical Audit LeadsppeterarmstrongNo ratings yet
- 2nd QUARTER EXAMINATION IN P. E 2019-2020Document3 pages2nd QUARTER EXAMINATION IN P. E 2019-2020Lyzl Mahinay Ejercito MontealtoNo ratings yet
- Surgical Audit and Peer Review Guide 2014Document54 pagesSurgical Audit and Peer Review Guide 2014juweriyNo ratings yet
- S 5 Schedule of Column Beam Wall Footing Detail Wall Footing Details UpdatedDocument1 pageS 5 Schedule of Column Beam Wall Footing Detail Wall Footing Details UpdatedJBFP100% (1)
- A Clinical Audit Practical HandbookDocument50 pagesA Clinical Audit Practical HandbookndimascioNo ratings yet
- Philippine LiteratureDocument82 pagesPhilippine LiteratureLovelene Chrizze100% (5)
- A GUIDE TO START CLINICAL AUDITSDocument13 pagesA GUIDE TO START CLINICAL AUDITSwassie gebiNo ratings yet
- What Is A Clinical EvaluationDocument2 pagesWhat Is A Clinical EvaluationSaraNo ratings yet
- Clinical Audit ProtocolDocument14 pagesClinical Audit Protocolsami ketemaNo ratings yet
- Practical Guide to Improving Clinical AuditDocument50 pagesPractical Guide to Improving Clinical Auditchunmun__sNo ratings yet
- Introduction to Clinical Effectiveness and Audit in HealthcareFrom EverandIntroduction to Clinical Effectiveness and Audit in HealthcareNo ratings yet
- Guidebook For Hospitals - 4th EditionDocument239 pagesGuidebook For Hospitals - 4th EditionJobin JamesNo ratings yet
- 5th Edition Hospital STD April 2020Document153 pages5th Edition Hospital STD April 2020Archana GaonkarNo ratings yet
- Practicalguideclaudit2013 PDFDocument86 pagesPracticalguideclaudit2013 PDFkylieverNo ratings yet
- Why Islam Is The True Religion in Light of The Quran and SunnahDocument7 pagesWhy Islam Is The True Religion in Light of The Quran and SunnahAsmau DaboNo ratings yet
- iHFG Part B Complete PDFDocument717 pagesiHFG Part B Complete PDFcobbymarkNo ratings yet
- 3rd Edition NABH Guidebook 2012.newDocument258 pages3rd Edition NABH Guidebook 2012.newDavid Turner93% (14)
- Nursing StaffingDocument5 pagesNursing StaffingPeace Andong PerochoNo ratings yet
- SHCO Standards - 3rd EditionDocument188 pagesSHCO Standards - 3rd Editionrenu100% (2)
- KPI OphthalmologyDocument46 pagesKPI OphthalmologyABM100% (6)
- Appraisal Handbook FinalDocument42 pagesAppraisal Handbook FinalmadmaxmaxmusNo ratings yet
- Daily Assessment RecordDocument4 pagesDaily Assessment Recordapi-342236522100% (2)
- OPPE ToolkitDocument70 pagesOPPE ToolkitBungKee IscmuNo ratings yet
- How to Enhance Your Medical Academic Portfolio: A Guide for Doctors in TrainingFrom EverandHow to Enhance Your Medical Academic Portfolio: A Guide for Doctors in TrainingNo ratings yet
- Class Opening Preparations Status ReportDocument3 pagesClass Opening Preparations Status ReportMaria Theresa Buscato86% (7)
- OPPE-FPPE ToolkitDocument71 pagesOPPE-FPPE ToolkitHosi Pba100% (1)
- NABH 5 STD April 2020Document120 pagesNABH 5 STD April 2020kapil100% (7)
- Nursing and Midwifery Workload Management StandardDocument11 pagesNursing and Midwifery Workload Management StandardabanewstdigitalNo ratings yet
- Nursing Audit ProtocolDocument15 pagesNursing Audit ProtocolMegersa AleneNo ratings yet
- 3rd Edition NABH Guidebook 2012 New PDFDocument258 pages3rd Edition NABH Guidebook 2012 New PDFraamki_99No ratings yet
- Framework of Standard Phase - 1Document98 pagesFramework of Standard Phase - 1Rajib Ul HaqueNo ratings yet
- Human Resource Management (HRM)Document8 pagesHuman Resource Management (HRM)Sarfraz LocusNo ratings yet
- Usaid Doh Records PDFDocument109 pagesUsaid Doh Records PDFJudy Ramos De GuzmanNo ratings yet
- 10.2 - Annual Clinical Audit Report 2013 - 2014Document32 pages10.2 - Annual Clinical Audit Report 2013 - 2014Accounts Grover MedicalsNo ratings yet
- Victorian AOD Clinician GuideDocument67 pagesVictorian AOD Clinician GuideHarjotBrar100% (1)
- Applying Lean Principles To A Continuing CareDocument5 pagesApplying Lean Principles To A Continuing CareEva VillalbaNo ratings yet
- EBC EHAQ 4 Audit Tool Final January 2024Document46 pagesEBC EHAQ 4 Audit Tool Final January 2024AberaNo ratings yet
- Surgical Site Infection Ssi Prevention Quality Improvement ToolDocument94 pagesSurgical Site Infection Ssi Prevention Quality Improvement ToolMelo Pérez Pamela J.No ratings yet
- Guidelines For Designation, Establishment and Upgrading of HfsDocument16 pagesGuidelines For Designation, Establishment and Upgrading of HfsNsubugaNo ratings yet
- EHAQ 4th Cycle Audit Tool Final Feb.10-2022Document51 pagesEHAQ 4th Cycle Audit Tool Final Feb.10-2022Michael Gebreamlak100% (1)
- Microsoft Word Safe Staffing The Basics NHPPD Version 1 0Document15 pagesMicrosoft Word Safe Staffing The Basics NHPPD Version 1 0odin9360343No ratings yet
- Australian Hospital Patient Costing Standards - Version 4.0 - Part 2 - Business RulesDocument76 pagesAustralian Hospital Patient Costing Standards - Version 4.0 - Part 2 - Business RulesHonors GroupNo ratings yet
- End User Training - Docx 4Document80 pagesEnd User Training - Docx 4yechale tafereNo ratings yet
- OPPE Dokter Di RS - EnglishDocument70 pagesOPPE Dokter Di RS - EnglishKetut Widiyasa BonaNo ratings yet
- E2C Addendum To ICH E2C Clinical Safety Data Management Periodic Safety Update Reports For Marketed DrugsDocument12 pagesE2C Addendum To ICH E2C Clinical Safety Data Management Periodic Safety Update Reports For Marketed Drugs涂皇堯No ratings yet
- User'S Manual: Workloadindicators OfstaffingneedDocument56 pagesUser'S Manual: Workloadindicators OfstaffingneedAchef RukmanaNo ratings yet
- WISN User ManualDocument52 pagesWISN User ManualBosman AriestaNo ratings yet
- Wada Guidelines Sample Collection Personnel 2014 v1.0 enDocument29 pagesWada Guidelines Sample Collection Personnel 2014 v1.0 ensome buddyyNo ratings yet
- 03 QAP Orientation For QMT Members (Davao Sur - Davao City) July 9, 2014Document68 pages03 QAP Orientation For QMT Members (Davao Sur - Davao City) July 9, 2014John Russell MoralesNo ratings yet
- Accreditation Manual 2nd EditionDocument49 pagesAccreditation Manual 2nd EditionjGithinji100% (2)
- Staffing Model DescriptionDocument14 pagesStaffing Model DescriptionImwaniki21No ratings yet
- Chapter 214: Clinical Services AdministrationDocument14 pagesChapter 214: Clinical Services AdministrationAhmad Gamal Elden MAhanyNo ratings yet
- MSS Primary HospitalsDocument128 pagesMSS Primary HospitalsRuzen BazzracharyaNo ratings yet
- NABET Accreditation Criteria for Hospital Consultants (NABH StandardsDocument16 pagesNABET Accreditation Criteria for Hospital Consultants (NABH StandardsDrnuzhat FatemaNo ratings yet
- QBP KidneyDocument36 pagesQBP KidneyRaka ArifirmandaNo ratings yet
- Salem Hospital Nurse Staffing PlanDocument3 pagesSalem Hospital Nurse Staffing PlanKathlyn Joy EclarinalNo ratings yet
- Medical Devices Training For Medical StaffDocument3 pagesMedical Devices Training For Medical StafffatematareefNo ratings yet
- PCA L1 - FinalDocument17 pagesPCA L1 - FinalNitin AgrawalNo ratings yet
- OP 65 PUBLIC Policy Printable VersionDocument30 pagesOP 65 PUBLIC Policy Printable VersionHadi AraouiNo ratings yet
- Ctas Pre HospitalDocument97 pagesCtas Pre HospitalHani Tri HandokoNo ratings yet
- Nguyen HA and Murai S (Eds.) - (2018) - Practices in Hospital Quality Management and PatientDocument98 pagesNguyen HA and Murai S (Eds.) - (2018) - Practices in Hospital Quality Management and PatientAnh Phạm VănNo ratings yet
- Homoeopathy Hospitals Guidebook - 2nd EditionDocument237 pagesHomoeopathy Hospitals Guidebook - 2nd EditionDr Ankit PardhiNo ratings yet
- Attestation Engagements on Sustainability Information (Including Greenhouse Gas Emissions Information)From EverandAttestation Engagements on Sustainability Information (Including Greenhouse Gas Emissions Information)No ratings yet
- Assessing Universal Health Coverage for Breast Cancer Management: Is the Service and Financial Coverage Adequate for Preventive and Curative Care?From EverandAssessing Universal Health Coverage for Breast Cancer Management: Is the Service and Financial Coverage Adequate for Preventive and Curative Care?No ratings yet
- MinitabDocument9 pagesMinitabJBFPNo ratings yet
- DATAENG PROJECT (Old Copy)Document2 pagesDATAENG PROJECT (Old Copy)JBFPNo ratings yet
- Roof Girders FinalDocument194 pagesRoof Girders FinalJBFPNo ratings yet
- DATAENG PROJECT (Old Copy)Document2 pagesDATAENG PROJECT (Old Copy)JBFPNo ratings yet
- Ulian River (Streamflow Data)Document88 pagesUlian River (Streamflow Data)JBFPNo ratings yet
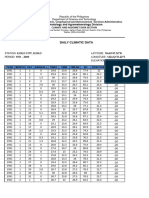
- Iloilo Daily Climatic Data (1951-2009)Document991 pagesIloilo Daily Climatic Data (1951-2009)JBFPNo ratings yet
- 190th Recognition RitesDocument272 pages190th Recognition RitesJBFPNo ratings yet
- Daniel Kenneth Villanueva: ProblemDocument7 pagesDaniel Kenneth Villanueva: ProblemJBFPNo ratings yet
- Thsvil2 FormaDocument1 pageThsvil2 FormaJBFPNo ratings yet
- Summer Term EnrollmentDocument7 pagesSummer Term EnrollmentJBFPNo ratings yet
- Application For Pure Online LearningDocument1 pageApplication For Pure Online LearningJBFPNo ratings yet
- 190th GCOE Recognition Rites Host ScriptDocument7 pages190th GCOE Recognition Rites Host ScriptJBFPNo ratings yet
- 190th GCOE Recognition Rites Host ScriptDocument7 pages190th GCOE Recognition Rites Host ScriptJBFPNo ratings yet
- A. Campus Entry and Exit Points: Vaccination Record Monitoring FormDocument5 pagesA. Campus Entry and Exit Points: Vaccination Record Monitoring FormJBFPNo ratings yet
- Kernel From Disclosure-No.-550-2020-Audited-Financial-Statements-as-of-December-31-2019-1Document4 pagesKernel From Disclosure-No.-550-2020-Audited-Financial-Statements-as-of-December-31-2019-1JBFPNo ratings yet
- Member Data Record: Villanueva, Daniel ChuaDocument1 pageMember Data Record: Villanueva, Daniel ChuaJBFPNo ratings yet
- A Small Bus Stop ProjectDocument2 pagesA Small Bus Stop ProjectJBFPNo ratings yet
- Academic Calendar CurrentDocument5 pagesAcademic Calendar CurrentJBFPNo ratings yet
- Canopy 3 Roof Beam Layout 1 2Nd Floor Roof Framing Plan 2: RB-1 RB-1 RB-1 SB-1 TRUSS-20Document1 pageCanopy 3 Roof Beam Layout 1 2Nd Floor Roof Framing Plan 2: RB-1 RB-1 RB-1 SB-1 TRUSS-20JBFPNo ratings yet
- S 4 Roof Framing Plan Schedule of FootingDocument1 pageS 4 Roof Framing Plan Schedule of FootingJBFPNo ratings yet
- S 2 Foundation Plan Second Floor Framming PlanDocument1 pageS 2 Foundation Plan Second Floor Framming PlanJBFPNo ratings yet
- Polygenic InheritanceDocument13 pagesPolygenic InheritanceSandeep Kumar RaghuvanshiNo ratings yet
- IPO Fact Sheet - Accordia Golf Trust 140723Document4 pagesIPO Fact Sheet - Accordia Golf Trust 140723Invest StockNo ratings yet
- Simulia Abaqus Standard DatasheetDocument3 pagesSimulia Abaqus Standard Datasheetuser923019231831No ratings yet
- Managing Post COVID SyndromeDocument4 pagesManaging Post COVID SyndromeReddy VaniNo ratings yet
- 2 5 Marking ScheduleDocument6 pages2 5 Marking Scheduleapi-218511741No ratings yet
- OPHTHALDocument8 pagesOPHTHALVarun ChandiramaniNo ratings yet
- Service Positioning and DesignDocument3 pagesService Positioning and DesignSaurabh SinhaNo ratings yet
- Fashion Cycle StepsDocument2 pagesFashion Cycle Stepssaranya narenNo ratings yet
- English Extra Conversation Club International Women's DayDocument2 pagesEnglish Extra Conversation Club International Women's Dayevagloria11No ratings yet
- Fermat points and the Euler circleDocument2 pagesFermat points and the Euler circleKen GamingNo ratings yet
- Oracle Apps Quality ModuleDocument17 pagesOracle Apps Quality ModuleSantOsh100% (2)
- Eole Press KitDocument15 pagesEole Press KitBob AndrepontNo ratings yet
- Project Report Software and Web Development Company: WWW - Dparksolutions.inDocument12 pagesProject Report Software and Web Development Company: WWW - Dparksolutions.inRavi Kiran Rajbhure100% (1)
- A Summer Internship Project ON " To Study The Supply Chain Management On Amul Fresh Products" AT GCMMF, AmulDocument19 pagesA Summer Internship Project ON " To Study The Supply Chain Management On Amul Fresh Products" AT GCMMF, AmulweetrydhNo ratings yet
- Mechanical Engineer with Experience in Heavy Mining Machinery MaintenanceDocument1 pageMechanical Engineer with Experience in Heavy Mining Machinery MaintenanceCertified Rabbits LoverNo ratings yet
- SeparatorDocument2 pagesSeparatormmk111No ratings yet
- Liquid Analysis v3 Powell-Cumming 2010 StanfordgwDocument28 pagesLiquid Analysis v3 Powell-Cumming 2010 StanfordgwErfanNo ratings yet
- Design & Construction of Substation 16P Painting System ComplianceDocument103 pagesDesign & Construction of Substation 16P Painting System ComplianceRamil LazNo ratings yet
- Staining TechniquesDocument31 pagesStaining TechniquesKhadija JaraNo ratings yet
- Operating Manual: Please Read These Operating Instructions Before Using Your FreedomchairDocument24 pagesOperating Manual: Please Read These Operating Instructions Before Using Your FreedomchairNETHYA SHARMANo ratings yet
- Interesting Facts (Compiled by Andrés Cordero 2023)Document127 pagesInteresting Facts (Compiled by Andrés Cordero 2023)AndresCorderoNo ratings yet
- History and Development of the Foodservice IndustryDocument23 pagesHistory and Development of the Foodservice IndustryMaria Athenna MallariNo ratings yet
- BOQ - Hearts & Arrows Office 04sep2023Document15 pagesBOQ - Hearts & Arrows Office 04sep2023ChristianNo ratings yet