You might also like
- GNI. PSD - Pengajuan Shop Drawing (R.00)Document1 pageGNI. PSD - Pengajuan Shop Drawing (R.00)Randha MuliaNo ratings yet
- Non-Compliance Report (NCR) : Liconin Limitted CompanyDocument2 pagesNon-Compliance Report (NCR) : Liconin Limitted CompanyMINH THÁINo ratings yet
- Form PenetrantDocument2 pagesForm PenetrantEko Adi PutraNo ratings yet
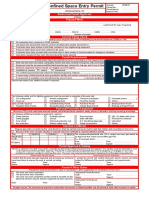
- D.08 - Confined Space Entry Permit FormDocument1 pageD.08 - Confined Space Entry Permit FormBenedito Cossa FelicianoNo ratings yet
- Work Permit - Plaza Lowyat Rev1Document1 pageWork Permit - Plaza Lowyat Rev1peikengNo ratings yet
- Form Renovation WorkDocument2 pagesForm Renovation WorkKhairulzamil NazimNo ratings yet
- 003 Implementation of WorkDocument1 page003 Implementation of WorkakbarNo ratings yet
- ABS EHS 36 Excavation Work PermitDocument2 pagesABS EHS 36 Excavation Work Permitsyed khaja misbhuddinNo ratings yet
- F TMD09 13Document1 pageF TMD09 13phatsorakornNo ratings yet
- Moa Perunding Design & BuiltDocument102 pagesMoa Perunding Design & BuiltIr Meor Shamshir100% (1)
- Work OrderDocument2 pagesWork OrderEriaNsyah AgMal100% (1)
- Box Culvert Construction Form PDFDocument12 pagesBox Culvert Construction Form PDFPaphanh FXNo ratings yet
- D.06 - Hot Work Permit FormDocument1 pageD.06 - Hot Work Permit FormBenedito Cossa FelicianoNo ratings yet
- Noc-Mw - Danzas Aei Emirates (L.L.C) (Mo0422 & Mo0422a)Document5 pagesNoc-Mw - Danzas Aei Emirates (L.L.C) (Mo0422 & Mo0422a)MUQEET ahmedNo ratings yet
- D.07 - Cold Work Permit FormDocument1 pageD.07 - Cold Work Permit FormBenedito Cossa FelicianoNo ratings yet
- FM-MR-13 NCR (Eng) (2020-11-16)Document3 pagesFM-MR-13 NCR (Eng) (2020-11-16)eAK TiNo ratings yet
- Rfwi FormDocument1 pageRfwi FormShida YunusNo ratings yet
- PERHATIAN: Lembaran Ini Harap Dibawa Saat Service: Cap Nama (Name)Document1 pagePERHATIAN: Lembaran Ini Harap Dibawa Saat Service: Cap Nama (Name)Ananda QomarasNo ratings yet
- First Aid Record Form: Personal DetailsDocument1 pageFirst Aid Record Form: Personal Detailspuput utomoNo ratings yet
- Permit To Work - Mechanical ContractorDocument2 pagesPermit To Work - Mechanical ContractorSamsudin AhmadNo ratings yet
- Acceptletter Based JKRDocument5 pagesAcceptletter Based JKRNUR HAMIZAH BINTI ISHAK STUDENTNo ratings yet
- Acceptance Letter JKRDocument5 pagesAcceptance Letter JKRNUR HAMIZAH BINTI ISHAK STUDENTNo ratings yet
- Sixth ScheduleDocument3 pagesSixth Scheduleangelene koidNo ratings yet
- Works Diary by Contractor (Mes)Document5 pagesWorks Diary by Contractor (Mes)BIJAY KRISHNA DASNo ratings yet
- Piccaso City Garden Condominum Project: Shop Drawing Submission For Approval (购物图纸提交批准)Document1 pagePiccaso City Garden Condominum Project: Shop Drawing Submission For Approval (购物图纸提交批准)Thai chheanghourtNo ratings yet
- Concrete Slab On Ground ITP TemeplateDocument3 pagesConcrete Slab On Ground ITP TemeplatecarolynneaNo ratings yet
- Piccaso City Garden Condominum Project: Shop Drawing Submission For Approval (购物图纸提交批准)Document1 pagePiccaso City Garden Condominum Project: Shop Drawing Submission For Approval (购物图纸提交批准)Thai chheanghourtNo ratings yet
- Contractor FormDocument2 pagesContractor FormMuhammadSyafie100% (1)
- Supervision Sheet DAILYDocument3 pagesSupervision Sheet DAILYamigoNo ratings yet
- D.09 - Vehicle Entry Permit FormDocument1 pageD.09 - Vehicle Entry Permit FormBenedito Cossa FelicianoNo ratings yet
- Payment RequestDocument1 pagePayment RequestRatha MenNo ratings yet
- Agarwal Cycles Job SheetDocument2 pagesAgarwal Cycles Job SheetsalmanNo ratings yet
- FORM XIX-Wage SlipDocument1 pageFORM XIX-Wage SlipRITE/ HRNo ratings yet
- Piccaso City Garden Condominum Project: Shop Drawing Submission For Approval (购物图纸提交批准)Document1 pagePiccaso City Garden Condominum Project: Shop Drawing Submission For Approval (购物图纸提交批准)Thai chheanghourtNo ratings yet
- LightsDocument5 pagesLightsTajiriMollelNo ratings yet
- Application For Staff QuarterDocument1 pageApplication For Staff Quarteragarwaalaaaa100% (1)
- Proforma 1 Certificate of Net Worth From Chartered AccountantDocument1 pageProforma 1 Certificate of Net Worth From Chartered Accountantaee lweNo ratings yet
- Proforma 1 Certificate of Net Worth From Chartered AccountantDocument1 pageProforma 1 Certificate of Net Worth From Chartered Accountantaee lweNo ratings yet
- Form Cek ListDocument2 pagesForm Cek ListRyan KapytanNo ratings yet
- 5A - Building Permit Renewal FormDocument1 page5A - Building Permit Renewal Formneharishi22No ratings yet
- SRT Tugas BLK (SPPD) - Aria-IkhwanDocument1 pageSRT Tugas BLK (SPPD) - Aria-IkhwanipungyanuasmaraNo ratings yet
- Trade License Application FormDocument2 pagesTrade License Application FormAbdul MomenNo ratings yet
- 31 - hs-78001 - Basic Safety Rules FormsDocument5 pages31 - hs-78001 - Basic Safety Rules Formsrony_lesbtNo ratings yet
- COPY-Emergent Works AuthorityDocument1 pageCOPY-Emergent Works AuthorityiGp2013No ratings yet
- Sans10400 A - Form 2 Rev 1Document3 pagesSans10400 A - Form 2 Rev 1richardkrigeNo ratings yet
- Manpower IndentDocument2 pagesManpower Indentaashik.nbcacNo ratings yet
- Reimbursements (1) 1Document1 pageReimbursements (1) 1Srinivasarao ObillaNo ratings yet
- Supplier Survey Form: (General Supplier / Sole Agent / Distributor / Representative / Manufacture / Sub KontractorDocument2 pagesSupplier Survey Form: (General Supplier / Sole Agent / Distributor / Representative / Manufacture / Sub KontractorPATRA SAMAPTANo ratings yet
- 3rd Schedule Regulation 53 Written Declaration On Design and Construction of Industrial Effluent Treatment SystemDocument2 pages3rd Schedule Regulation 53 Written Declaration On Design and Construction of Industrial Effluent Treatment SystemLye lyeNo ratings yet
- Cidb Standard Form of Contract 2000Document127 pagesCidb Standard Form of Contract 2000Zad LiaNo ratings yet
- Model I - Pma (Penanaman Modal Asing)Document7 pagesModel I - Pma (Penanaman Modal Asing)mightylubuNo ratings yet
- India Patent Form 4Document2 pagesIndia Patent Form 4adityakochharNo ratings yet
- BQ Retaining WallDocument26 pagesBQ Retaining WallnurfirdausfadzilNo ratings yet
- FM-HR-BPK-06 Permohonan Bantuan Pelunasan Excess of ClaimsDocument1 pageFM-HR-BPK-06 Permohonan Bantuan Pelunasan Excess of Claimsbudi firgiantosaNo ratings yet
- Sans10400 A - Form 3Document4 pagesSans10400 A - Form 3gbharcombeNo ratings yet
- LNR Constructions (PVT) LTD.: Estimate Bill of QuantityDocument4 pagesLNR Constructions (PVT) LTD.: Estimate Bill of QuantitylnrneltechNo ratings yet
- Non-Compliance Report (NCR) : Liconin Limitted CompanyDocument2 pagesNon-Compliance Report (NCR) : Liconin Limitted CompanyMINH THÁINo ratings yet
- PSMB GIG 3 20-Trainee-Attendance-FormDocument1 pagePSMB GIG 3 20-Trainee-Attendance-FormMogana RawanNo ratings yet
- Do MOOODocument9 pagesDo MOOOTajiriMollelNo ratings yet
- Daily Safety Report (11!07!2018) LOT-2Document1 pageDaily Safety Report (11!07!2018) LOT-2Abdul RafeequeNo ratings yet
- PTW Shamasiya 20211009002Document6 pagesPTW Shamasiya 20211009002Abdul RafeequeNo ratings yet
- Accident/Incident Report Section 1: Details of Person Making This ReportDocument2 pagesAccident/Incident Report Section 1: Details of Person Making This ReportAbdul RafeequeNo ratings yet
- Corporate Projects Project Management Manual Hse Inspection/Audit Checklist Contract: Date Inspected: NWC Representatives: Areas InspectedDocument11 pagesCorporate Projects Project Management Manual Hse Inspection/Audit Checklist Contract: Date Inspected: NWC Representatives: Areas InspectedAbdul RafeequeNo ratings yet
- Manual Handling Risk Assessment Form: Department / Service: Location: Date: Assessed By: Signature: Review DateDocument2 pagesManual Handling Risk Assessment Form: Department / Service: Location: Date: Assessed By: Signature: Review DateAbdul RafeequeNo ratings yet
- Project Management Manual Hse Assessment Checklist: Acceptance of The Hse Assessment For The Method StatementDocument19 pagesProject Management Manual Hse Assessment Checklist: Acceptance of The Hse Assessment For The Method StatementAbdul RafeequeNo ratings yet
- Corporate Projects Project Management Manual Local Hse Legislation RegisterDocument4 pagesCorporate Projects Project Management Manual Local Hse Legislation RegisterAbdul RafeequeNo ratings yet
- PMF-012-COM-013 v1 Non Conformance ReportDocument5 pagesPMF-012-COM-013 v1 Non Conformance ReportAbdul RafeequeNo ratings yet
- Weekly HSE Reports: Indicators/ Metrics This Week Month (8) Year To Date Project To DateDocument2 pagesWeekly HSE Reports: Indicators/ Metrics This Week Month (8) Year To Date Project To DateAbdul RafeequeNo ratings yet
- National Water Company Permit To Work (PTW) : 1. Plastering Work at Pump StationDocument2 pagesNational Water Company Permit To Work (PTW) : 1. Plastering Work at Pump StationAbdul RafeequeNo ratings yet
- Pump Station: Corporate Projects Project Management Manual Hse Observation RecordDocument2 pagesPump Station: Corporate Projects Project Management Manual Hse Observation RecordAbdul RafeequeNo ratings yet
- Continuous Testing in DevOpsDocument6 pagesContinuous Testing in DevOpssimonaNo ratings yet
- Sem Unp Lab ProgramsDocument39 pagesSem Unp Lab ProgramsEnduku MeekuNo ratings yet
- 01 134201 066 10175976863 15112022 012600pm 1Document5 pages01 134201 066 10175976863 15112022 012600pm 1Hášṅáť ḾálịǩNo ratings yet
- SDWAN - A Technical Tutorial by FAE Telecom Oct2019Document40 pagesSDWAN - A Technical Tutorial by FAE Telecom Oct2019Jonny TekNo ratings yet
- Chapter - 001: Computer Fundamental & HistoryDocument33 pagesChapter - 001: Computer Fundamental & HistoryPRAVINITNo ratings yet
- Machine Condition Monitoring Project Final ReportDocument11 pagesMachine Condition Monitoring Project Final ReportSivasidharth EzhilNo ratings yet
- Presentacion Serie X DahuaDocument40 pagesPresentacion Serie X DahuaDaniel Flores SánchezNo ratings yet
- Step1:: The Steps For Installing Windows7 OSDocument16 pagesStep1:: The Steps For Installing Windows7 OSابو حميد ابو حميدNo ratings yet
- ISO 27001 MappingDocument17 pagesISO 27001 MappingNikolas Kyriakidis100% (1)
- 762 ExperionHS PIN March09Document10 pages762 ExperionHS PIN March09FITAS MOUNIRNo ratings yet
- Is Lab Manual IT 801Document32 pagesIs Lab Manual IT 801sai thesisNo ratings yet
- Rached Boubaker: Odoo DeveloperDocument4 pagesRached Boubaker: Odoo DeveloperAymenNo ratings yet
- Application Building With IotDocument64 pagesApplication Building With IotNahom DiresNo ratings yet
- Man in The Middle Attacks ARP Poisoning: Redirect Packets To and From Any Client To Our DeviceDocument19 pagesMan in The Middle Attacks ARP Poisoning: Redirect Packets To and From Any Client To Our DevicemarkopvNo ratings yet
- Hospital Manage-WPS OfficeDocument20 pagesHospital Manage-WPS OfficePranita PawarNo ratings yet
- Communiques - DP - DP 302 Submission of Annual System Audit ReportDocument13 pagesCommuniques - DP - DP 302 Submission of Annual System Audit ReportscnehraNo ratings yet
- Module 3 CDSS PDFDocument44 pagesModule 3 CDSS PDFGanga Nayan T LNo ratings yet
- BSIT Tracer Study Sir RundelleDocument25 pagesBSIT Tracer Study Sir RundelleJosenia Constantino100% (2)
- Diebold Nixdorf BEETLE XSDocument33 pagesDiebold Nixdorf BEETLE XSOferty Firm / SklepówNo ratings yet
- Amcrest+Http+API+9 202Document651 pagesAmcrest+Http+API+9 202nmccomputerNo ratings yet
- Excel J17-31 ModifiedDocument4 pagesExcel J17-31 Modifiedmahmoud shaheenNo ratings yet
- User Guide Nokia 1 Plus User GuideDocument55 pagesUser Guide Nokia 1 Plus User GuideNimal RanasingheNo ratings yet
- AZ-104 ExamDocument195 pagesAZ-104 Examankushsingh007100% (1)
- Ivo NgalaDocument3 pagesIvo NgalaashokNo ratings yet
- Heterogeneous Integration and Chiplet Assembly - All Between 2D and 3DDocument5 pagesHeterogeneous Integration and Chiplet Assembly - All Between 2D and 3DAnkit KaulNo ratings yet
- Automatic Billing System Using ZigbeeDocument6 pagesAutomatic Billing System Using ZigbeeBrightworld ProjectsNo ratings yet
- REPS and Co Application Runbook Template: Matt WilhelmDocument6 pagesREPS and Co Application Runbook Template: Matt WilhelmMilet HidrosoloNo ratings yet
- JAVA Full Stack Development New VersionDocument3 pagesJAVA Full Stack Development New VersionmisbahNo ratings yet
- Mc-Unit IDocument16 pagesMc-Unit IShankara NarayananNo ratings yet
- Master TheoremDocument21 pagesMaster TheoremBhuvnesh Kumar100% (1)