You might also like
- Albumin Drug StudyDocument1 pageAlbumin Drug StudyMaine Concepcion100% (1)
- Cerebrovascular Accident (Stroke) Drug Study: Submitted By: Daryl S. AbrahamDocument4 pagesCerebrovascular Accident (Stroke) Drug Study: Submitted By: Daryl S. AbrahamBiway RegalaNo ratings yet
- FINAL Student Preparation Surgical Client Case and Safe Medication AdministrationDocument3 pagesFINAL Student Preparation Surgical Client Case and Safe Medication AdministrationsaemhatdsbNo ratings yet
- Rheumatologic Renal Disease: SLE vs. SclerodermaDocument2 pagesRheumatologic Renal Disease: SLE vs. SclerodermaKenNo ratings yet
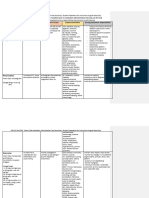
- Drug and Dosage Drug Classification Therapeutic Action Indications Contraindications Adverse Effects Nursing ConsiderationsDocument3 pagesDrug and Dosage Drug Classification Therapeutic Action Indications Contraindications Adverse Effects Nursing ConsiderationszhandygurlNo ratings yet
- Drug StudyDocument8 pagesDrug StudyJuan de Vera100% (4)
- Arterial Hypertension Eng PDFDocument29 pagesArterial Hypertension Eng PDFagustinaw1981No ratings yet
- Drug StudyDocument14 pagesDrug StudyNikki RodrigoNo ratings yet
- Glomerulopathies: Hasyim Kasim Divisi Nephrology and Hypertensi FKUH 2016Document39 pagesGlomerulopathies: Hasyim Kasim Divisi Nephrology and Hypertensi FKUH 2016andiNo ratings yet
- Hematuria 2019 PEDIATRIA PDFDocument7 pagesHematuria 2019 PEDIATRIA PDFfernanda garnicaNo ratings yet
- CeftriaxoneDocument3 pagesCeftriaxonejiloNo ratings yet
- Drug Gordons PeDocument6 pagesDrug Gordons PeNicko Pazon AranasNo ratings yet
- Drug Study Amphotericin B, Meropenem, Furosemide, Ciprofloxacin, Pentoxifylline, Pip-Tazo, Midazolam, VecuroniumDocument12 pagesDrug Study Amphotericin B, Meropenem, Furosemide, Ciprofloxacin, Pentoxifylline, Pip-Tazo, Midazolam, Vecuroniumpaupaulala100% (4)
- Roca-Drug Study Week2Document3 pagesRoca-Drug Study Week2Leah Mariz RocaNo ratings yet
- Aspirin (FSW)Document4 pagesAspirin (FSW)khelxoNo ratings yet
- Chronic Complications of Diabetes MellitusDocument48 pagesChronic Complications of Diabetes MellitusReina TarihoranNo ratings yet
- Introduction To Glomerular DiseaseDocument16 pagesIntroduction To Glomerular DiseaseAdrian ZapataNo ratings yet
- Pheochromocytoma Conn'S Disease: Primary Hyperaldosteronism Refers To HypersecretionDocument13 pagesPheochromocytoma Conn'S Disease: Primary Hyperaldosteronism Refers To HypersecretionAirish LimNo ratings yet
- DR AfableDocument25 pagesDR AfableJohnny DeeNo ratings yet
- Capsule: 500 MG Injection: 100Document2 pagesCapsule: 500 MG Injection: 100Melissa Marie CustodioNo ratings yet
- Drug Study Aspirin, Clopidogrel, HydrochlorothiazideDocument4 pagesDrug Study Aspirin, Clopidogrel, Hydrochlorothiazidepaupaulala77% (13)
- Glomerular DiseasesDocument5 pagesGlomerular DiseasesAdrian ZapataNo ratings yet
- Clinical Presentation & Management of Glomerular Diseases: Hematuria, Nephritic & Nephrotic SyndromeDocument4 pagesClinical Presentation & Management of Glomerular Diseases: Hematuria, Nephritic & Nephrotic SyndromeMutiara FauzaNo ratings yet
- 1 s2.0 S1578219008703275 MainDocument10 pages1 s2.0 S1578219008703275 Mainavnish sharmaNo ratings yet
- Drug Study Week2Document3 pagesDrug Study Week2Leah Mariz RocaNo ratings yet
- DRUG Mefenamic AcidDocument2 pagesDRUG Mefenamic Acidbeautifuljade_16No ratings yet
- Approach To PurpuraDocument33 pagesApproach To PurpuraAyushi MishalNo ratings yet
- Drug Study: NCM 106 PharmacologyDocument4 pagesDrug Study: NCM 106 PharmacologyLore Anne Mhae SantosNo ratings yet
- Glomerulonephritis 2019Document31 pagesGlomerulonephritis 2019EsoklailNo ratings yet
- Patho MicroDocument17 pagesPatho Microjyothsna yarraNo ratings yet
- Bolile Aparatului Urogenital: Glomerulonefrita Acuta Difuza PoststreptococicaDocument17 pagesBolile Aparatului Urogenital: Glomerulonefrita Acuta Difuza PoststreptococicanadaNo ratings yet
- Drug StudyDocument13 pagesDrug StudyJimuel Brian ManelaNo ratings yet
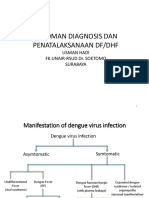
- DHF - DinkesDocument31 pagesDHF - DinkesAlfindraHaidaNabilaNo ratings yet
- Chronic Kidney Disease DR Moses KazevuDocument29 pagesChronic Kidney Disease DR Moses KazevuMoses Jr KazevuNo ratings yet
- Drug Study: Far Eastern UniversityDocument3 pagesDrug Study: Far Eastern UniversityChoy DacanayNo ratings yet
- Generic Name & Brand Name Mechanism of Action Indications and Drug Rationale Contraindications Common Side Effects Nursing ConsiderationsDocument2 pagesGeneric Name & Brand Name Mechanism of Action Indications and Drug Rationale Contraindications Common Side Effects Nursing ConsiderationsMary Shine GonidaNo ratings yet
- Drug Study MixDocument29 pagesDrug Study MixMatty JolbitadoNo ratings yet
- Drug Study HydrocodoneDocument1 pageDrug Study HydrocodoneYlrenne DyNo ratings yet
- Drug Study AspirinDocument1 pageDrug Study AspirinMaria Charis Anne Indanan100% (1)
- Steroid Responsif Nephrotic Syndrome (SRNS)Document16 pagesSteroid Responsif Nephrotic Syndrome (SRNS)Ikrar AbdillahNo ratings yet
- Schematic Diagram of The Pathophysiology of Nephrotic SyndromeDocument1 pageSchematic Diagram of The Pathophysiology of Nephrotic SyndromenurNo ratings yet
- CNS: Dizziness, Assessment History: Allergy ToDocument7 pagesCNS: Dizziness, Assessment History: Allergy To6teen_gurlNo ratings yet
- GLOMERULOPATHYDocument51 pagesGLOMERULOPATHYAumnissa SamsiNo ratings yet
- Acute Kidney Injury Kidney Infection: ClasificationDocument1 pageAcute Kidney Injury Kidney Infection: ClasificationSiti RuchjayaniNo ratings yet
- Sindrom NefrotikDocument32 pagesSindrom NefrotikCindy AmeLiyana Part IINo ratings yet
- Glomerulonefritis Akut Dan Kronis: DR - Hasan Basri, Sppd-Kgh-FinasimDocument53 pagesGlomerulonefritis Akut Dan Kronis: DR - Hasan Basri, Sppd-Kgh-FinasimnadddNo ratings yet
- Final CC EdemaDocument31 pagesFinal CC EdematabatchNo ratings yet
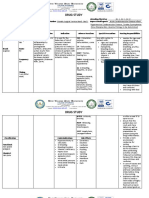
- Name of Drug Mechanism of Action Indication Contraindication Adverse Effect Nursing Responsibility Generic Name: Brand Name: Classification: CnsDocument4 pagesName of Drug Mechanism of Action Indication Contraindication Adverse Effect Nursing Responsibility Generic Name: Brand Name: Classification: CnsRoxy TofyNo ratings yet
- conceptmap-DIABETES MELLITUSDocument8 pagesconceptmap-DIABETES MELLITUSDonnabell DayudayNo ratings yet
- Case Study On AGNDocument28 pagesCase Study On AGNArchana SahuNo ratings yet
- Syncope CasesFrom EverandSyncope CasesRoberto García-CiveraNo ratings yet
- Diabetes in Hospital: A Practical Approach for Healthcare ProfessionalsFrom EverandDiabetes in Hospital: A Practical Approach for Healthcare ProfessionalsNo ratings yet
- Human Tumours Secreting Catecholamines: Clinical and Physiopathological Study of the PheochromocytomasFrom EverandHuman Tumours Secreting Catecholamines: Clinical and Physiopathological Study of the PheochromocytomasRating: 5 out of 5 stars5/5 (1)
- The Perfect Neutropenic Diet Cookbook; The Complete Nutrition Guide To Reinstating Overall Health For General Wellness With Delectable And Nourishing RecipesFrom EverandThe Perfect Neutropenic Diet Cookbook; The Complete Nutrition Guide To Reinstating Overall Health For General Wellness With Delectable And Nourishing RecipesNo ratings yet
- Hepatorenal Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHepatorenal Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Generalized Anxiety Disorder Case Study 2017Document4 pagesGeneralized Anxiety Disorder Case Study 2017Pratik SinghNo ratings yet
- All Mycoses SGDDocument140 pagesAll Mycoses SGDkashan100% (1)
- Patient Room No 320 Name: Patient G.F. Problem/Case: Gestational Diabetes MellitusDocument2 pagesPatient Room No 320 Name: Patient G.F. Problem/Case: Gestational Diabetes MellitusBel CortezNo ratings yet
- 30926722: 2019 Update of The EULAR Recommendations For The Management of Systemic Lupus ErythematosusDocument10 pages30926722: 2019 Update of The EULAR Recommendations For The Management of Systemic Lupus ErythematosusLuis Enrique Caceres AlavrezNo ratings yet
- Anti-Inflammatory Effect of Panyawan Stem For Toothache (1)Document10 pagesAnti-Inflammatory Effect of Panyawan Stem For Toothache (1)Nolemae NavalesNo ratings yet
- Gallbladder Specialist SurgeonDocument5 pagesGallbladder Specialist SurgeonGeorgia Top SurgeonsNo ratings yet
- 2018 01 Early Pregnancy Loss LightDocument41 pages2018 01 Early Pregnancy Loss LightMishal FatimaNo ratings yet
- Philosophy of Internal Medicine - Osler and HinohaDocument3 pagesPhilosophy of Internal Medicine - Osler and HinohaSri ViisnnuNo ratings yet
- Laporan KunjunganDocument6 pagesLaporan KunjungananggiNo ratings yet
- Personal Health NotesDocument6 pagesPersonal Health NotesMichael ReiferNo ratings yet
- NICU QI Project To Decrease Neonatal Death2015Document24 pagesNICU QI Project To Decrease Neonatal Death2015Elias TewabeNo ratings yet
- An Auricular Marker For Covid-19: Nadia Volf, MD, PHD, Valery Salques, MD, and Anne Lassaux, MDDocument2 pagesAn Auricular Marker For Covid-19: Nadia Volf, MD, PHD, Valery Salques, MD, and Anne Lassaux, MDyan92120No ratings yet
- Francesca Genco, Antonella Sarasini, Maurizio Parea, Martina Prestia, Valeria Meroni Background ResultsDocument1 pageFrancesca Genco, Antonella Sarasini, Maurizio Parea, Martina Prestia, Valeria Meroni Background ResultsFouad RahiouyNo ratings yet
- Screening For Diabetic Retinopathy in Europe - Progress Since 2005Document17 pagesScreening For Diabetic Retinopathy in Europe - Progress Since 2005NaveenJainNo ratings yet
- MastitisDocument2 pagesMastitisJuviely PremacioNo ratings yet
- Ethics and The Care of Critically Ill Infants and ChildrenDocument6 pagesEthics and The Care of Critically Ill Infants and ChildrenmirandastoreNo ratings yet
- Alterations in VentilationDocument10 pagesAlterations in VentilationCharisma Pastor100% (1)
- CR Jason Michael Hauk Botchford 2019-0297-0066Document2 pagesCR Jason Michael Hauk Botchford 2019-0297-0066Bob MackinNo ratings yet
- Mikro PDFDocument6 pagesMikro PDFYudha Pradhana PutraNo ratings yet
- Therese ADocument2 pagesTherese ATherese MananghayaNo ratings yet
- VITILIGO (SAFED DAAG OR SHIVTRA) :leucodermaDocument3 pagesVITILIGO (SAFED DAAG OR SHIVTRA) :leucodermaDr shailendra Kumar NaithaniNo ratings yet
- Diabetes Foot CareDocument2 pagesDiabetes Foot CareseramulambaNo ratings yet
- FHP BlankDocument12 pagesFHP BlankDarlyn AmplayoNo ratings yet
- Welly@unissula - Ac.id: Welly Anggarani, Sandy Christiono, Prima AgusmawantiDocument6 pagesWelly@unissula - Ac.id: Welly Anggarani, Sandy Christiono, Prima Agusmawantinabilah syahirahNo ratings yet
- Sanitary Awakening in IndiaDocument34 pagesSanitary Awakening in IndiasiegherrNo ratings yet
- Drug Study For BronchiectasisDocument6 pagesDrug Study For BronchiectasisEdith AlegreNo ratings yet
- Penetrating Cardiac InjuryDocument7 pagesPenetrating Cardiac InjuryRidelNo ratings yet
- Neurocognitive DisorderDocument50 pagesNeurocognitive DisorderMechaela SiasatNo ratings yet
- DetailedapproaDocument65 pagesDetailedapproaMuhammed BarznjiNo ratings yet