You might also like
- Advanced farriery knowledge: A study guide and AWCF theory course companionFrom EverandAdvanced farriery knowledge: A study guide and AWCF theory course companionNo ratings yet
- Anatomy Biomechanics of The Hip PDFDocument8 pagesAnatomy Biomechanics of The Hip PDFangelluis1980No ratings yet
- Healthy Hips Handbook: Exercises for Treating and Preventing Common Hip Joint InjuriesFrom EverandHealthy Hips Handbook: Exercises for Treating and Preventing Common Hip Joint InjuriesNo ratings yet
- Pilates For Scapular DyskinesisDocument16 pagesPilates For Scapular Dyskinesiskapturzak100% (1)
- Human Anatomy Synopsis Spine PDFDocument109 pagesHuman Anatomy Synopsis Spine PDFInês Fernandes100% (1)
- Anatomy, Abdomen and Pelvis, Quadratus Lumborum: December 2018Document7 pagesAnatomy, Abdomen and Pelvis, Quadratus Lumborum: December 2018Fer NandoNo ratings yet
- Anatomy, Bony Pelvis and Lower Limb, Leg Bones: February 2019Document8 pagesAnatomy, Bony Pelvis and Lower Limb, Leg Bones: February 2019Chess NutsNo ratings yet
- The Evolution of The Vertebral ColumnDocument12 pagesThe Evolution of The Vertebral ColumnBoyana GrigorovaNo ratings yet
- The Pelvic Floor - Structure - Function - Muscles - TeachMeAnatomyDocument3 pagesThe Pelvic Floor - Structure - Function - Muscles - TeachMeAnatomyrizwanakm96No ratings yet
- Neuroanatomy, Spinal Cord Myotatic Reflex - StatPearls - NCBI Bookshelf 2Document1 pageNeuroanatomy, Spinal Cord Myotatic Reflex - StatPearls - NCBI Bookshelf 2Vienna TulauanNo ratings yet
- Scapular Dyskinesia, The Forgotten Culprit of Shoulder Pain and How To RehabilitateDocument6 pagesScapular Dyskinesia, The Forgotten Culprit of Shoulder Pain and How To RehabilitateQuiroprácticaParaTodosNo ratings yet
- Biomechanics of Human SpineDocument41 pagesBiomechanics of Human Spinebisnismail88No ratings yet
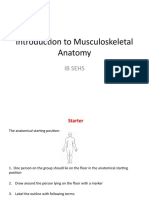
- Introduction To Musculoskeletal Anatomy: Ib SehsDocument34 pagesIntroduction To Musculoskeletal Anatomy: Ib SehsMaggie-Louise BellamyNo ratings yet
- Hamstring 12-23 2Document10 pagesHamstring 12-23 2Pótha JohannaNo ratings yet
- Anatomy Lab 6Document16 pagesAnatomy Lab 6Mariam2180No ratings yet
- ProQuestDocuments 2022 03 01Document11 pagesProQuestDocuments 2022 03 01Éoghan McCulloughNo ratings yet
- Core 2 TextbookDocument41 pagesCore 2 TextbooksfgeNo ratings yet
- Pilates For The Treatment Fo Postural Hyper Kyphosis PDFDocument17 pagesPilates For The Treatment Fo Postural Hyper Kyphosis PDFbrunoduartefrNo ratings yet
- Diskinesia EscapularDocument9 pagesDiskinesia EscapularArmandoRiosNo ratings yet
- Kibler Et Al 2012 Scapula Dyskinesis and Its Relation To Shoulder Injury PDFDocument9 pagesKibler Et Al 2012 Scapula Dyskinesis and Its Relation To Shoulder Injury PDFPamela DíazNo ratings yet
- Kafo Ortotik ProstetikDocument41 pagesKafo Ortotik ProstetikAinunJariyahNo ratings yet
- Banton BiomechanicsDocument9 pagesBanton BiomechanicsIoan AndraNo ratings yet
- 4th Grade Science Workbook Term 3: Name: - ClassDocument21 pages4th Grade Science Workbook Term 3: Name: - ClassJezabel MolinaNo ratings yet
- Ecz Grade 10 - 12 Biology Summarised Notes (Locomotion and The Skeleton) With Exam Questions and AnswersDocument15 pagesEcz Grade 10 - 12 Biology Summarised Notes (Locomotion and The Skeleton) With Exam Questions and AnswersItx Jones100% (1)
- Terminology 1A&PDocument30 pagesTerminology 1A&PNadan KhanNo ratings yet
- Human Anatomy & Physiology of Hip JointDocument4 pagesHuman Anatomy & Physiology of Hip JointZed P. EstalillaNo ratings yet
- Structures of The Hip Joint: Articulating SurfacesDocument7 pagesStructures of The Hip Joint: Articulating SurfacesChethan K NarayanNo ratings yet
- Hip Bone: Hip Bone (Os Coxae, Innominate Bone, Pelvic Bone Coxal Bone) Is A LargeDocument9 pagesHip Bone: Hip Bone (Os Coxae, Innominate Bone, Pelvic Bone Coxal Bone) Is A LargeranshNo ratings yet
- Vertebral TechniquesDocument24 pagesVertebral TechniquesOnofrei Oana ElenaNo ratings yet
- Cervical SpondylitisDocument21 pagesCervical SpondylitisRudolph Antony ThomasNo ratings yet
- Spinal Stenosis Q & ADocument28 pagesSpinal Stenosis Q & AProfessor Stephen D. Waner67% (3)
- Mod 1.4 Hip JointDocument23 pagesMod 1.4 Hip JointNandhkishoreNo ratings yet
- Feature: An Introduction To Cranial Movement and OrthodonticsDocument4 pagesFeature: An Introduction To Cranial Movement and OrthodonticsabeNo ratings yet
- Year 7 Notes Chapter B1. 2 Structure and Function of Body SystemDocument71 pagesYear 7 Notes Chapter B1. 2 Structure and Function of Body SystemNurhafiza Ab MajidNo ratings yet
- Neurological Physiotherapy Evaluation Form 2 0Document82 pagesNeurological Physiotherapy Evaluation Form 2 0Eman SabryNo ratings yet
- Presented By: Directed By:: Department of Tashreeh-UL-Badan (Anatomy)Document38 pagesPresented By: Directed By:: Department of Tashreeh-UL-Badan (Anatomy)QC quadcoreNo ratings yet
- Theories of Growth (Autosaved)Document53 pagesTheories of Growth (Autosaved)Harish Kumar.THOTANo ratings yet
- BTEC Sport Level 3 Revision Guide Skeletal SystemDocument23 pagesBTEC Sport Level 3 Revision Guide Skeletal SystemMP100% (3)
- A Rare Anatomical Variation of Palmaris Longus Muscle - A Case ReportDocument3 pagesA Rare Anatomical Variation of Palmaris Longus Muscle - A Case ReportEditor IJTSRDNo ratings yet
- Pelvic Fractures: BackgroundDocument21 pagesPelvic Fractures: BackgroundAdrianNo ratings yet
- Anatomy of The PelvisDocument6 pagesAnatomy of The Pelvisapi-195986134No ratings yet
- Back Pain PDFDocument40 pagesBack Pain PDFsana shiekhNo ratings yet
- The Lower Limb - Boundless Anatomy and PhysiologyDocument15 pagesThe Lower Limb - Boundless Anatomy and PhysiologyHurulaeniNo ratings yet
- 2.0 Tissues and Supporting SystemDocument39 pages2.0 Tissues and Supporting Systemwalterkalu385No ratings yet
- Biomechanics of Posterior Shoulder Instability - Current Knowledge and Literature ReviewDocument11 pagesBiomechanics of Posterior Shoulder Instability - Current Knowledge and Literature ReviewRaúl GonzálezNo ratings yet
- CH 41 LBP - Braddom's Physical Medicine & RehabilitationDocument46 pagesCH 41 LBP - Braddom's Physical Medicine & RehabilitationPyrectic WilliamsNo ratings yet
- Axial SkeletonDocument7 pagesAxial SkeletonArmileo C AuxteroNo ratings yet
- Human Anatomy PDFDocument22 pagesHuman Anatomy PDFWally WallyNo ratings yet
- L-Spine Spine Lumbar AnatomyDocument8 pagesL-Spine Spine Lumbar AnatomyWilliamNo ratings yet
- Neuroanatomy, Putamen: April 2020Document12 pagesNeuroanatomy, Putamen: April 2020liorahelgaNo ratings yet
- Muscles SharkDocument9 pagesMuscles SharkJames Sumagaysay100% (1)
- Biomechanics of Head and NeckDocument14 pagesBiomechanics of Head and NeckMann SabahNo ratings yet
- ISSA FastTrack Basic and Applied Sciences PDFDocument8 pagesISSA FastTrack Basic and Applied Sciences PDFOlufemi PalmerNo ratings yet
- ISSA FastTrack Basic and Applied Sciences PDFDocument8 pagesISSA FastTrack Basic and Applied Sciences PDFOlufemi Palmer0% (1)
- SMR 00275 ShoulderDocument15 pagesSMR 00275 ShoulderIulian FrunzăNo ratings yet
- Nasir BDocument7 pagesNasir BArthur CostaNo ratings yet
- Anatomy of Exercise PDFDocument98 pagesAnatomy of Exercise PDFnyanaung82% (11)
- (Jean Oliver and Alison Middleditch (Auth.) ) Funct (B-Ok - CC)Document332 pages(Jean Oliver and Alison Middleditch (Auth.) ) Funct (B-Ok - CC)Lorena BurdujocNo ratings yet
- Detailed Reconstruction of The Musculature in Limnognathia Maerski (Micrognathozoa) and Comparison With Other GnathiferaDocument17 pagesDetailed Reconstruction of The Musculature in Limnognathia Maerski (Micrognathozoa) and Comparison With Other GnathiferaDayana FlorezNo ratings yet
- Musculoskeletal SystemDocument47 pagesMusculoskeletal SystemZULFIKAR GHOZI MALIKUL AKBAR -No ratings yet
- Trauma Center 2019 720p WEBRip x264 AAC-HUD-hrv SRTDocument52 pagesTrauma Center 2019 720p WEBRip x264 AAC-HUD-hrv SRTMilorad SpasićNo ratings yet
- Ziropadja, LJ., O Surovosti Iz Poslusnosti PDFDocument14 pagesZiropadja, LJ., O Surovosti Iz Poslusnosti PDFneils23No ratings yet
- License AgreementDocument1 pageLicense Agreementrobert7000No ratings yet
- License AgreementDocument1 pageLicense Agreementrobert7000No ratings yet
- Metode Otkrivanja LaziDocument15 pagesMetode Otkrivanja LaziSteel90No ratings yet
- License AgreementDocument1 pageLicense Agreementrobert7000No ratings yet
- Esp-2000 BSDocument6 pagesEsp-2000 BSByron LopezNo ratings yet
- Cover Sheet: Online Learning and Teaching (OLT) Conference 2006, Pages Pp. 21-30Document12 pagesCover Sheet: Online Learning and Teaching (OLT) Conference 2006, Pages Pp. 21-30Shri Avinash NarendhranNo ratings yet
- Kharrat Et Al., 2007 (Energy - Fuels)Document4 pagesKharrat Et Al., 2007 (Energy - Fuels)Leticia SakaiNo ratings yet
- 20171025141013chapter-3 Chi-Square-Test PDFDocument28 pages20171025141013chapter-3 Chi-Square-Test PDFNajwa WawaNo ratings yet
- Applied Social Research A Tool For The Human Services 9th Edition Monette Test Bank 1Document36 pagesApplied Social Research A Tool For The Human Services 9th Edition Monette Test Bank 1wesleyvasquezmeoapcjtrb100% (25)
- The Latest Open Source Software Available and The Latest Development in IctDocument10 pagesThe Latest Open Source Software Available and The Latest Development in IctShafirahFameiJZNo ratings yet
- Statement 1680409132566Document11 pagesStatement 1680409132566úméshNo ratings yet
- English ExerciseDocument2 pagesEnglish ExercisePankhuri Agarwal100% (1)
- How To Measure Light Levels and Lux LevelsDocument4 pagesHow To Measure Light Levels and Lux LevelsAngelo PalamingNo ratings yet
- Macro Economics A2 Level Notes Book PDFDocument33 pagesMacro Economics A2 Level Notes Book PDFMustafa Bilal50% (2)
- IFE Level 4 Certificate in Fire InvestigationDocument16 pagesIFE Level 4 Certificate in Fire InvestigationMarlon FordeNo ratings yet
- Dhulikhel RBB PDFDocument45 pagesDhulikhel RBB PDFnepalayasahitya0% (1)
- Topic 3 - Analyzing The Marketing EnvironmentDocument28 pagesTopic 3 - Analyzing The Marketing Environmentmelissa chlNo ratings yet
- Samudra-Pasai at The Dawn of The European AgeDocument39 pagesSamudra-Pasai at The Dawn of The European AgemalaystudiesNo ratings yet
- CP AssignmentDocument5 pagesCP AssignmentMSSM EngineeringNo ratings yet
- Annexure I Project Details DateDocument4 pagesAnnexure I Project Details DateAshish SinghaniaNo ratings yet
- Electric Vehicle Charging Station BplanDocument19 pagesElectric Vehicle Charging Station BplanAjithNo ratings yet
- S L Dixon Fluid Mechanics and Thermodynamics of TurbomachineryDocument4 pagesS L Dixon Fluid Mechanics and Thermodynamics of Turbomachinerykuma alemayehuNo ratings yet
- CHECK - Chapter 11 TCD AnswersDocument6 pagesCHECK - Chapter 11 TCD AnswersbonolomphaNo ratings yet
- Festival Implementation PlanDocument5 pagesFestival Implementation Planapi-318058589No ratings yet
- W1 - V1 MultipleWorksheets SolnDocument3 pagesW1 - V1 MultipleWorksheets SolnAKHIL RAJ SNo ratings yet
- Chemistry For PhotographersDocument184 pagesChemistry For PhotographersBahar ShoghiNo ratings yet
- GRADE 1 MUSIC Week 1 Learning PacketsDocument16 pagesGRADE 1 MUSIC Week 1 Learning PacketsQuennie Rose EderNo ratings yet
- Syllabus Math 305Document4 pagesSyllabus Math 305Nataly SusanaNo ratings yet
- Understand Fox Behaviour - Discover WildlifeDocument1 pageUnderstand Fox Behaviour - Discover WildlifeChris V.No ratings yet
- 04 10 ALINT DatasheetDocument2 pages04 10 ALINT DatasheetJoakim LangletNo ratings yet
- Anin, Cris Adrian U. Experiment Water Flirtation ELECTIVE 103Document2 pagesAnin, Cris Adrian U. Experiment Water Flirtation ELECTIVE 103Cris Adrian Umadac AninNo ratings yet
- What Are The Challenges and Opportunities of ResearchingDocument5 pagesWhat Are The Challenges and Opportunities of ResearchingmelkyNo ratings yet
- Fix LHA Whole PagesDocument81 pagesFix LHA Whole PagesvuonghhNo ratings yet
- CATIA V5-6R2015 Basics - Part I : Getting Started and Sketcher WorkbenchFrom EverandCATIA V5-6R2015 Basics - Part I : Getting Started and Sketcher WorkbenchRating: 4 out of 5 stars4/5 (10)
- SketchUp Success for Woodworkers: Four Simple Rules to Create 3D Drawings Quickly and AccuratelyFrom EverandSketchUp Success for Woodworkers: Four Simple Rules to Create 3D Drawings Quickly and AccuratelyRating: 1.5 out of 5 stars1.5/5 (2)
- Certified Solidworks Professional Advanced Weldments Exam PreparationFrom EverandCertified Solidworks Professional Advanced Weldments Exam PreparationRating: 5 out of 5 stars5/5 (1)
- FreeCAD | Step by Step: Learn how to easily create 3D objects, assemblies, and technical drawingsFrom EverandFreeCAD | Step by Step: Learn how to easily create 3D objects, assemblies, and technical drawingsRating: 5 out of 5 stars5/5 (1)
- Product Manufacturing and Cost Estimating using CAD/CAE: The Computer Aided Engineering Design SeriesFrom EverandProduct Manufacturing and Cost Estimating using CAD/CAE: The Computer Aided Engineering Design SeriesRating: 4 out of 5 stars4/5 (4)
- Beginning AutoCAD® 2020 Exercise WorkbookFrom EverandBeginning AutoCAD® 2020 Exercise WorkbookRating: 2.5 out of 5 stars2.5/5 (3)
- Autodesk Inventor 2020: A Power Guide for Beginners and Intermediate UsersFrom EverandAutodesk Inventor 2020: A Power Guide for Beginners and Intermediate UsersNo ratings yet
- Autodesk Fusion 360: A Power Guide for Beginners and Intermediate Users (3rd Edition)From EverandAutodesk Fusion 360: A Power Guide for Beginners and Intermediate Users (3rd Edition)Rating: 5 out of 5 stars5/5 (2)