You might also like
- Free Ebook Food As MedicineDocument53 pagesFree Ebook Food As MedicineRudi ArsanaNo ratings yet
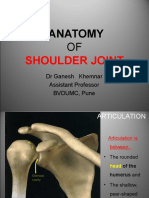
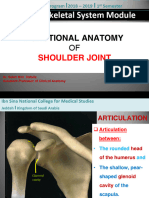
- Shoulder JointDocument37 pagesShoulder JointsandeepNo ratings yet
- Muscle Innervation Chart IIDocument7 pagesMuscle Innervation Chart IIkimsue9448No ratings yet
- 04 - Meninges - DR Najeeb NeuroanatomyDocument18 pages04 - Meninges - DR Najeeb Neuroanatomyhiba jasimNo ratings yet
- Anatomy and Histology Mock BoardsDocument29 pagesAnatomy and Histology Mock BoardsSheena PasionNo ratings yet
- Upper Limb MusclesDocument19 pagesUpper Limb MusclesVinod Sharma100% (1)
- Back Anatomy TableDocument7 pagesBack Anatomy TableJeffrey XieNo ratings yet
- 811 Anatomy of Shoulder JointDocument51 pages811 Anatomy of Shoulder JointAishwarya PatilNo ratings yet
- Gatus vs. SSS, January 26, 2011, GR No. 174725Document1 pageGatus vs. SSS, January 26, 2011, GR No. 174725abot69No ratings yet
- 397.001 - Orthopedics) Rotator Cuff TearDocument11 pages397.001 - Orthopedics) Rotator Cuff Tearvkpremiyahoo.comNo ratings yet
- Abg InterpretationDocument13 pagesAbg Interpretationgwapz23No ratings yet
- CH 19 Spinal AnaesthesiaDocument29 pagesCH 19 Spinal AnaesthesiaChristian Leepo100% (1)
- PTB Case StudyDocument11 pagesPTB Case StudyCharisse Joy Cudal100% (17)
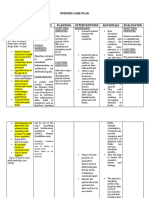
- Nursing Care Plan Diarrhea Assessment Diagnosis Planning Interventions Rationale EvaluationDocument8 pagesNursing Care Plan Diarrhea Assessment Diagnosis Planning Interventions Rationale EvaluationKrahNo ratings yet
- Voies D'abord MasqueletDocument385 pagesVoies D'abord MasqueletAlexandru MazurNo ratings yet
- UW Notes - 11 - MSK ArrangedDocument66 pagesUW Notes - 11 - MSK ArrangedDor BenayounNo ratings yet
- CN FanyDocument24 pagesCN FanymiaNo ratings yet
- Schumann 1. ExtremiitiesDocument12 pagesSchumann 1. ExtremiitiesCrystal AyalaNo ratings yet
- Muscle, Origin, InsertionDocument9 pagesMuscle, Origin, Insertionshananana1616No ratings yet
- .4 Cervical and Thoracic P3Document19 pages.4 Cervical and Thoracic P3ELIZABETH GRACE AMADORNo ratings yet
- Blue Boxes For Head and NeckDocument11 pagesBlue Boxes For Head and NeckhajajyNo ratings yet
- Brachial Plexus BlockDocument1 pageBrachial Plexus Blocksunny kumarNo ratings yet
- ANA.S4.CA22.Lower Extremity IDocument13 pagesANA.S4.CA22.Lower Extremity ICazz HeyNo ratings yet
- Posterior NeckDocument2 pagesPosterior NeckCarlo BarriosNo ratings yet
- CLAVICULADocument9 pagesCLAVICULANylla Shin Hyenna LieNo ratings yet
- 6 SDL On Muscles of Arm and ForearmDocument43 pages6 SDL On Muscles of Arm and ForearmsandyNo ratings yet
- Clinical Anatomy of Back, Spinal Cord and Spinal NervesDocument31 pagesClinical Anatomy of Back, Spinal Cord and Spinal Nervesmade ngurah100% (1)
- Elbow JointDocument6 pagesElbow JointDharm PatelNo ratings yet
- 2.08 Brachial Region (Arm) - Compartments, Muscles, Nerves, and VesselsDocument3 pages2.08 Brachial Region (Arm) - Compartments, Muscles, Nerves, and VesselsDi CanNo ratings yet
- CN 4 6Document39 pagesCN 4 6Radityo Akhmedika FauzieNo ratings yet
- Shoulder JointDocument30 pagesShoulder JointbalsaNo ratings yet
- 22-Shoulder JointDocument24 pages22-Shoulder Jointnemo shNo ratings yet
- 07-Shoulder JointDocument42 pages07-Shoulder JointVaishnaviNo ratings yet
- Bones of The Upper Limb (Oct 25, 2022)Document48 pagesBones of The Upper Limb (Oct 25, 2022)huzaifa arshadNo ratings yet
- Xray Spinal, Skull + Head CT (PBL Icm II Week 3)Document3 pagesXray Spinal, Skull + Head CT (PBL Icm II Week 3)Janetta RheaNo ratings yet
- Duttons LibroDocument2 pagesDuttons LibroGUSTAVO ANDRÉS RIVERA-DAVIDNo ratings yet
- Anatomi BahuDocument4 pagesAnatomi BahuSheila Setiawati TanzilNo ratings yet
- Lateral Region Simplified For TransDocument4 pagesLateral Region Simplified For TransJess PeltraNo ratings yet
- Anatomy Shelf NotesDocument200 pagesAnatomy Shelf Notesashwini dhoteNo ratings yet
- Anatomy Shelf NotesDocument200 pagesAnatomy Shelf NotesJad MitriNo ratings yet
- S: Spinal Cord DisordersDocument69 pagesS: Spinal Cord DisordersSteph StephanieNo ratings yet
- Shoulder DynamicsDocument17 pagesShoulder DynamicsShaista MunirNo ratings yet
- MMB (018) Elbow Joint Cubital Fossa (Practical) 2022Document39 pagesMMB (018) Elbow Joint Cubital Fossa (Practical) 2022Mohamed AhmedNo ratings yet
- 07 Shoulder JointDocument27 pages07 Shoulder JointYara WaelNo ratings yet
- Extremities Table of NervesDocument3 pagesExtremities Table of NervesFG ArciagaNo ratings yet
- Chapter 1. BackDocument17 pagesChapter 1. Backleafyislucky 91No ratings yet
- 9d Orbit-Blood Vessels & Nerves-Dr-GosaiDocument8 pages9d Orbit-Blood Vessels & Nerves-Dr-GosaiDr.B.B.GosaiNo ratings yet
- Neuroanatomy Practical 2nd ShiftDocument2 pagesNeuroanatomy Practical 2nd Shiftapi-19502000No ratings yet
- Muscles EscanillaDocument9 pagesMuscles EscanillaESCANILLA CRISTINENo ratings yet
- Diseases of The Spinal CordDocument15 pagesDiseases of The Spinal CordBai Aishwayra Haylee DalidigNo ratings yet
- Diagn0sis 0ff H3@dacheDocument7 pagesDiagn0sis 0ff H3@dacheLINDSLEY GONo ratings yet
- Brachial Plexus Injury LatestDocument37 pagesBrachial Plexus Injury LatestRajhmuniran KandasamyNo ratings yet
- Chapter 21 Back of The Neck NewDocument63 pagesChapter 21 Back of The Neck NewMohan PalanimalaiNo ratings yet
- Imaging Anatomy Musculoskeletal (B. J. Manaster, Julia Crim) (Z-Lib - Org) Split-Merge - extractPDFpagesDocument12 pagesImaging Anatomy Musculoskeletal (B. J. Manaster, Julia Crim) (Z-Lib - Org) Split-Merge - extractPDFpagesChristian ToalongoNo ratings yet
- The Elbow JointDocument4 pagesThe Elbow JointMd Ahsanuzzaman PinkuNo ratings yet
- Trochlear Nerve Cranial Nerve IV AtfDocument4 pagesTrochlear Nerve Cranial Nerve IV AtfRishi VermaNo ratings yet
- 02.muscles of Pectoral Girdle and MoreDocument71 pages02.muscles of Pectoral Girdle and MoremathivannaninthujanNo ratings yet
- Upper Extremity - Muscle Summary ChartDocument9 pagesUpper Extremity - Muscle Summary ChartpoggerNo ratings yet
- 3 Arm, Cubital Fossa & Elbow JointDocument25 pages3 Arm, Cubital Fossa & Elbow JointImkita MngqundanisoNo ratings yet
- Muscles of Pectoral RegionDocument11 pagesMuscles of Pectoral RegionTomar PrabhakarNo ratings yet
- Thorax Forms The Upper Part of The Trunk of The BodyDocument159 pagesThorax Forms The Upper Part of The Trunk of The BodymabdulmateenpkNo ratings yet
- Brainstem: External and Internal FeaturesDocument57 pagesBrainstem: External and Internal FeaturesJoaquin GuillermoNo ratings yet
- Muscles AnatomyDocument14 pagesMuscles AnatomyJiya JithinNo ratings yet
- Clinical Anatomy 5: Breast, Pectoral, and AxillaDocument3 pagesClinical Anatomy 5: Breast, Pectoral, and AxillaJohn DoeNo ratings yet
- Ana 1 Ca2 FaceDocument2 pagesAna 1 Ca2 FaceJohn DoeNo ratings yet
- Ca: Anterior Triangle of The Neck: Shift #Document3 pagesCa: Anterior Triangle of The Neck: Shift #John DoeNo ratings yet
- Ana.1.ca1.scalp and SkullDocument3 pagesAna.1.ca1.scalp and SkullJohn DoeNo ratings yet
- CVA StrokeDocument6 pagesCVA StrokeMcrstna Lim SorianoNo ratings yet
- Kumpulan InstrumenDocument10 pagesKumpulan Instrumenreni50% (2)
- Silverman DRAFTDocument7 pagesSilverman DRAFT܁No ratings yet
- 5 NFSC 470 Case Study - CeliacDocument9 pages5 NFSC 470 Case Study - Celiacapi-242530221No ratings yet
- Environmental SurveillanceDocument11 pagesEnvironmental Surveillancedr rajoreNo ratings yet
- Romero, Deinielle Ingrid M. (Hiv)Document8 pagesRomero, Deinielle Ingrid M. (Hiv)Deinielle Magdangal RomeroNo ratings yet
- Hall 2015Document9 pagesHall 2015Nach Medina SesmasNo ratings yet
- Non-Communicable Diseases and Physical Inactivity: Sir KarlDocument15 pagesNon-Communicable Diseases and Physical Inactivity: Sir KarlMarwin CandareNo ratings yet
- Radiographic Pathology For Technologists 7th Edition Kowalczyk Test BankDocument6 pagesRadiographic Pathology For Technologists 7th Edition Kowalczyk Test Bankbeatrixkhuyen9rm100% (22)
- The Life of Swami-PurushottamanandaDocument121 pagesThe Life of Swami-PurushottamanandaJogeshsahooNo ratings yet
- Eating Disorders: Manos, Bencio, Fernandes, ParaisoDocument66 pagesEating Disorders: Manos, Bencio, Fernandes, ParaisoShannen Fernandez100% (1)
- Antihypertensive DrugsDocument5 pagesAntihypertensive DrugsAiman TymerNo ratings yet
- OK - HP8003 NotesDocument71 pagesOK - HP8003 NotesjamesngNo ratings yet
- SCD Factsheet What Is SCDDocument5 pagesSCD Factsheet What Is SCDAustine OsaweNo ratings yet
- Chronic Kidney Disease : Hypertensive and Diabetic Retinopathy in PatientsDocument7 pagesChronic Kidney Disease : Hypertensive and Diabetic Retinopathy in PatientsAnonymous FgT04krgymNo ratings yet
- Nursing DiagnosisDocument5 pagesNursing DiagnosisGeovanni Rai HermanoNo ratings yet
- Urinalysis InterpretationDocument9 pagesUrinalysis InterpretationNicku MalanceaNo ratings yet
- Colon CancerDocument17 pagesColon CancerYaska MusaNo ratings yet
- RinderpestDocument5 pagesRinderpestKinara PutriNo ratings yet
- Soal Ujian Semester Kelas 12Document12 pagesSoal Ujian Semester Kelas 12Andy Hamzah FansuryNo ratings yet
- Appendicitis Menigitis Shingles (Mayo Clinic Def)Document11 pagesAppendicitis Menigitis Shingles (Mayo Clinic Def)Lucila LugoNo ratings yet
- Drug Study Vent Forgram)Document2 pagesDrug Study Vent Forgram)arvie_mirandaNo ratings yet
- Thyroidinum CasesDocument2 pagesThyroidinum CasesAgaNo ratings yet
- Nutrition Knowledge, Attitudes, and Self-Regulation As PDFDocument9 pagesNutrition Knowledge, Attitudes, and Self-Regulation As PDFJoem cNo ratings yet
- Fournier'S Gangrene: Rajah Amina SuleimanDocument27 pagesFournier'S Gangrene: Rajah Amina SuleimanAmina RajahNo ratings yet