You might also like
- Contraception and Sterilization FinalDocument2 pagesContraception and Sterilization FinalRasheedAladdinNGuiomalaNo ratings yet
- Acute Abnormal Uterine Bleeding (Aub) : AlgorithmDocument8 pagesAcute Abnormal Uterine Bleeding (Aub) : AlgorithmPhiyaNo ratings yet
- Note Oct 20, 2020Document4 pagesNote Oct 20, 2020Maha AlzarafiNo ratings yet
- Objectives: Common Medications in Obstetrics & GynecologyDocument9 pagesObjectives: Common Medications in Obstetrics & Gynecologygazi haseebNo ratings yet
- Trans On OB-1 Family-PlanningDocument12 pagesTrans On OB-1 Family-PlanningPriscilla Jean UmenganNo ratings yet
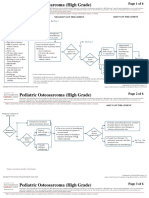
- CA Treatment Osteosarcoma Pedi Web AlgorithmDocument6 pagesCA Treatment Osteosarcoma Pedi Web AlgorithmyaseenNo ratings yet
- Family Planning: By: Khalid Jemal (MD, Assistant Prof. of Obstetrics & Gynecology)Document73 pagesFamily Planning: By: Khalid Jemal (MD, Assistant Prof. of Obstetrics & Gynecology)Degefaw BikoyNo ratings yet
- Bulacan State University College of NursingDocument4 pagesBulacan State University College of NursingAmbeguia ElijahNo ratings yet
- Page 1 of 22: Risk Assessment Prevention/Prophylaxis of Anticipatory Nausea/VomitingDocument22 pagesPage 1 of 22: Risk Assessment Prevention/Prophylaxis of Anticipatory Nausea/VomitingEmaNo ratings yet
- Coc 1Document17 pagesCoc 1Ahmed AnwarNo ratings yet
- Contraception Lec 1Document38 pagesContraception Lec 1fh2785519No ratings yet
- Abdominal PDFDocument1 pageAbdominal PDFChakra BaktiNo ratings yet
- Hormonal Contraception Webinar KOGS 13.10Document44 pagesHormonal Contraception Webinar KOGS 13.10Alice KaariaNo ratings yet
- Carolyn R. Zalameda-Castro, MDDocument9 pagesCarolyn R. Zalameda-Castro, MDeza floresNo ratings yet
- Contraception & HRTDocument14 pagesContraception & HRTWheezy BruhNo ratings yet
- ContraceptiveDocument53 pagesContraceptiveAbas AhmedNo ratings yet
- Contraception CMEDocument57 pagesContraception CMEstephaniesoniamethewNo ratings yet
- (Gyne) Family Planning (Dra Ona - Dra Castro) Updated Version (2022)Document14 pages(Gyne) Family Planning (Dra Ona - Dra Castro) Updated Version (2022)NoreenNo ratings yet
- 4 Family PlanningDocument7 pages4 Family Planninghk5vnxp2x5No ratings yet
- Ca Treatment Breast Noninvasive Web AlgorithmDocument6 pagesCa Treatment Breast Noninvasive Web Algorithmmarcelo chavez diazNo ratings yet
- Contraception: Sara Alhaddab Lama AlshwairikhDocument9 pagesContraception: Sara Alhaddab Lama AlshwairikhRyubusa HayabusaNo ratings yet
- Contraception OBG PresentationDocument15 pagesContraception OBG Presentationfawkesrox03No ratings yet
- Overview of Contraceptive Methods TableDocument3 pagesOverview of Contraceptive Methods Tablelarazahabi0% (1)
- Bahan Tugas Tokolitik Ulfadiya Putri 1Document25 pagesBahan Tugas Tokolitik Ulfadiya Putri 1hopa shopNo ratings yet
- Hormonal ContraceptivesDocument6 pagesHormonal ContraceptivesGoia PullNo ratings yet
- Correct Use of Misoprostol For Induction of Labour KLMNSDocument31 pagesCorrect Use of Misoprostol For Induction of Labour KLMNSsabellanabimanya9No ratings yet
- Contraception: Nur Hafizah Ainaa Abu HassanDocument53 pagesContraception: Nur Hafizah Ainaa Abu Hassanshravani100% (1)
- HO 4 Essential Intrapartum Care 6may2013Document12 pagesHO 4 Essential Intrapartum Care 6may2013Lot RositNo ratings yet
- SURGERY Breast DiseasesDocument25 pagesSURGERY Breast DiseasesBiplav SinghNo ratings yet
- Reproductive Health PowerNotes by KT SirDocument2 pagesReproductive Health PowerNotes by KT Sirjumihuss08No ratings yet
- Predisposing-Factors 20231129 134609 0000Document1 pagePredisposing-Factors 20231129 134609 0000Mary Mathel Del RosarioNo ratings yet
- Drug Study Tromadol + ParacetamolDocument2 pagesDrug Study Tromadol + Paracetamol6fq2cmfgn4No ratings yet
- 10 1097@MD 0000000000019643Document7 pages10 1097@MD 0000000000019643Bayu PermanaNo ratings yet
- Estrogen ProgesteronDocument12 pagesEstrogen Progesterondokter wawanNo ratings yet
- Ass DrugDocument1 pageAss Drug2080315No ratings yet
- Intercourse and IslamDocument52 pagesIntercourse and IslamEngr. Khandaker Marsus75% (4)
- Ca - Treatment-Breast-Inflammatory-Web-AlgorithmDocument19 pagesCa - Treatment-Breast-Inflammatory-Web-AlgorithmAgustin SierraNo ratings yet
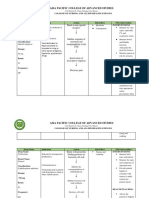
- Drug Study: College of NursingDocument2 pagesDrug Study: College of NursingGab AggabaoNo ratings yet
- ContraceptivesDocument7 pagesContraceptivesdhavalNo ratings yet
- If Bleeding Persists, or If Woman Requests It, Medical Treatment Can Be ConsideredDocument2 pagesIf Bleeding Persists, or If Woman Requests It, Medical Treatment Can Be ConsideredChon ChiNo ratings yet
- CM OBGYN 8,9 Copy.Document8 pagesCM OBGYN 8,9 Copy.jamierogers427No ratings yet
- Contraception: Objective at The End of This Lecture The 5 Year Student Should Be Able ToDocument22 pagesContraception: Objective at The End of This Lecture The 5 Year Student Should Be Able ToAmmarNo ratings yet
- Which Initial Therapy To Choose To Crohns and UCDocument63 pagesWhich Initial Therapy To Choose To Crohns and UCfahmyhhablassNo ratings yet
- 33 - FSRH-CEU Progesterone Implant 2014Document32 pages33 - FSRH-CEU Progesterone Implant 2014Muhammad Javed GabaNo ratings yet
- DS 2ND SemDocument8 pagesDS 2ND SemRhobic ManansalaNo ratings yet
- DS 3 Ectopic PregnancyDocument2 pagesDS 3 Ectopic PregnancyJohn Kenley FerryNo ratings yet
- GO ClindamycinDocument9 pagesGO ClindamycinSAMANTHA T. MODESTONo ratings yet
- Reports Edited CPH RDocument50 pagesReports Edited CPH RMicah Lou CalambaNo ratings yet
- Uhh I AgreeDocument3 pagesUhh I AgreeTyler VintNo ratings yet
- DeadDocument1 pageDeadTyler VintNo ratings yet
- Infographic EndonutritionDocument1 pageInfographic EndonutritionLuis Felipe TorresNo ratings yet
- Acute Painful Scrotum: ALGORITHM-Suspicion For Testicular TorsionDocument13 pagesAcute Painful Scrotum: ALGORITHM-Suspicion For Testicular TorsionM. ANDRI PRASETYONo ratings yet
- شيت اوبس وقايناDocument19 pagesشيت اوبس وقايناFares OsmanNo ratings yet
- ContraceptionDocument34 pagesContraceptionMimo HemadNo ratings yet
- Drug Study DRDocument14 pagesDrug Study DRJb RosillosaNo ratings yet
- Birth ControlDocument13 pagesBirth Controlapi-374195102No ratings yet
- VTE - Treating With The Right Anticoagulant and Duration (May 2018)Document6 pagesVTE - Treating With The Right Anticoagulant and Duration (May 2018)Dexter SiaNo ratings yet
- Effects of The Etonogestrel Contraceptive Implant (Implanon) On Bone Metabolism During Lactation: A Prospective StudyDocument5 pagesEffects of The Etonogestrel Contraceptive Implant (Implanon) On Bone Metabolism During Lactation: A Prospective StudyFahmi Nur SuwandiNo ratings yet
- Ch 1 - Q & Answers 1 -محولDocument51 pagesCh 1 - Q & Answers 1 -محولEman Shalaby100% (1)
- Glossary of Patient SafetyDocument352 pagesGlossary of Patient SafetyEman ShalabyNo ratings yet
- 10-Mostafa ... New Questions & Its Answer-1Document16 pages10-Mostafa ... New Questions & Its Answer-1Eman ShalabyNo ratings yet
- SHCherbal HealthDocument281 pagesSHCherbal HealthEman ShalabyNo ratings yet
- Q-Solution 3 - 3Document44 pagesQ-Solution 3 - 3Eman ShalabyNo ratings yet
- Essential Medicines List 2020Document67 pagesEssential Medicines List 2020Eman ShalabyNo ratings yet
- 60137 - قائمة الأدوية السعوديةDocument565 pages60137 - قائمة الأدوية السعوديةEman ShalabyNo ratings yet
- Drugs Without An Approved GenericDocument234 pagesDrugs Without An Approved GenericEman ShalabyNo ratings yet
- Mapping The ATC Classification To The UMLS Metathesaurus: Some Pragmatic ApplicationsDocument10 pagesMapping The ATC Classification To The UMLS Metathesaurus: Some Pragmatic ApplicationsEman ShalabyNo ratings yet
- 97Document480 pages97Eman ShalabyNo ratings yet
- Risk Minimization Activity (ARMML)Document11 pagesRisk Minimization Activity (ARMML)Eman ShalabyNo ratings yet
- NAC Asthma COPD Meds Chart November 2020 WebDocument1 pageNAC Asthma COPD Meds Chart November 2020 WebEman ShalabyNo ratings yet
- لیست کد های ATCDocument123 pagesلیست کد های ATCEman ShalabyNo ratings yet
- Abdominal Pain - Male: PAIN SEVERITY Is Defined AsDocument13 pagesAbdominal Pain - Male: PAIN SEVERITY Is Defined AsEman ShalabyNo ratings yet
- Lippincott Illustrated Reviews (PDFDrive) - Pages-396Document1 pageLippincott Illustrated Reviews (PDFDrive) - Pages-396Eman ShalabyNo ratings yet
- Lippincott Illustrated Reviews (PDFDrive) - Pages-396Document2 pagesLippincott Illustrated Reviews (PDFDrive) - Pages-396Eman ShalabyNo ratings yet
- Adventures in Tandem NursingDocument3 pagesAdventures in Tandem NursingPesawaran VacationNo ratings yet
- Midwifery Terminology: Mrs.V.Elizebeth Rani ReaderDocument14 pagesMidwifery Terminology: Mrs.V.Elizebeth Rani ReaderSamira MohamudNo ratings yet
- 2.2 NCM 109 - Complications During Pregnancy, Labor and Delivery and Postpartum PeriodsDocument10 pages2.2 NCM 109 - Complications During Pregnancy, Labor and Delivery and Postpartum PeriodsSittie Haneen TabaraNo ratings yet
- Diagnosis of PregnancyDocument4 pagesDiagnosis of PregnancyIsrael WoseneNo ratings yet
- This Study Resource WasDocument4 pagesThis Study Resource WasOrange AlvarezNo ratings yet
- Chapter 23Document5 pagesChapter 23kristiannedenNo ratings yet
- Product BrochureDocument2 pagesProduct BrochureSangeen AliNo ratings yet
- The Effect of A Training Program During Pregnancy On The Attitude and Intention of NulliparousDocument8 pagesThe Effect of A Training Program During Pregnancy On The Attitude and Intention of NulliparousNoraNo ratings yet
- Maternal Newborn NursingDocument11 pagesMaternal Newborn NursingRaf Luis100% (4)
- NCM 107 (Related Learning Experience) : in Partial Fulfillment of The Requirement inDocument4 pagesNCM 107 (Related Learning Experience) : in Partial Fulfillment of The Requirement inTiffany Joy QuiliopeNo ratings yet
- Kaplan1998 PDFDocument6 pagesKaplan1998 PDFAmsir LimbongNo ratings yet
- Obstracteded LabourDocument4 pagesObstracteded LabourNishaThakuriNo ratings yet
- Pap Smear Test and InformationDocument7 pagesPap Smear Test and Informationiangould12No ratings yet
- Concept MapDocument1 pageConcept MapkriizNo ratings yet
- From Egg and Sperm To NewbornDocument63 pagesFrom Egg and Sperm To NewbornCristine Joy GuinoNo ratings yet
- Leopold'S Maneuvers: How Common Is It in Our Daily Practice?Document4 pagesLeopold'S Maneuvers: How Common Is It in Our Daily Practice?Aina HaravataNo ratings yet
- Anatomy and Physiology of Female Reproductive System:: VaginaDocument5 pagesAnatomy and Physiology of Female Reproductive System:: VaginaphallicNo ratings yet
- Polycystic Ovary SyndromeDocument13 pagesPolycystic Ovary SyndromeNAYSHA YANET CHAVEZ RONDINELNo ratings yet
- Mnemonics PDFDocument18 pagesMnemonics PDFEyob Mizan83% (6)
- Family Planning Lesson PlanDocument23 pagesFamily Planning Lesson PlanIvan Bautista Cortez73% (15)
- ANM SyllabusDocument9 pagesANM SyllabusMonica ZineNo ratings yet
- Reproductive Health Questions With AnswersDocument3 pagesReproductive Health Questions With AnswersPrajwal d100% (1)
- Menstrual Hygiene Amongst The School Going Adolescent Girls in Rural AreaDocument5 pagesMenstrual Hygiene Amongst The School Going Adolescent Girls in Rural AreaMuhammad GhiffariNo ratings yet
- Fetal SurvillanceDocument26 pagesFetal SurvillanceBetelhem EjiguNo ratings yet
- NCM QuizDocument7 pagesNCM QuizKyla Marie NabongNo ratings yet
- Normal Labour: PRESENTED BY DR Tsitsi Vimbayi ChatoraDocument13 pagesNormal Labour: PRESENTED BY DR Tsitsi Vimbayi ChatoraChatora Tsitsi VimbayiNo ratings yet
- Gynae & Obs Bcqs BookletDocument58 pagesGynae & Obs Bcqs BookletKiran Ayub100% (1)
- Sample Soap NoteDocument12 pagesSample Soap NoteSedaka Donaldson0% (1)
- Session 4: Pregnancy and Antenatal CareDocument21 pagesSession 4: Pregnancy and Antenatal CareqonitaNo ratings yet
- Commed PPT (Deepthi)Document22 pagesCommed PPT (Deepthi)Nivedha RajanNo ratings yet