You might also like
- Chapter 2 PDFDocument64 pagesChapter 2 PDFsubiNo ratings yet
- The Management of Chronic Diseases: Organizational Innovation and EfficiencyFrom EverandThe Management of Chronic Diseases: Organizational Innovation and EfficiencyNo ratings yet
- Liya Os Complete 2Document61 pagesLiya Os Complete 2Twinkle VlogsNo ratings yet
- Integrating Emergency Management and Disaster Behavioral Health: One Picture through Two LensesFrom EverandIntegrating Emergency Management and Disaster Behavioral Health: One Picture through Two LensesNo ratings yet
- Review Self ManagementDocument25 pagesReview Self ManagementAlaa AlanaziNo ratings yet
- HospitalDocument27 pagesHospitaljyothiNo ratings yet
- Internship ContentDocument27 pagesInternship ContentmtpjusailaNo ratings yet
- Strategi Clinical Governance Dalam Perbaikan Mutu Pelayanan Rumah Sakit (Clinical Governance Strategy in Improving of Hospital Care Quality)Document6 pagesStrategi Clinical Governance Dalam Perbaikan Mutu Pelayanan Rumah Sakit (Clinical Governance Strategy in Improving of Hospital Care Quality)Rima RaisyiahNo ratings yet
- Management in Hospital Nursing: Group 3Document20 pagesManagement in Hospital Nursing: Group 3Puji PrisylNo ratings yet
- Community Health NursingDocument4 pagesCommunity Health NursingDaniel Andre S. SomorayNo ratings yet
- CHN Reviewer Midterm TopicsDocument19 pagesCHN Reviewer Midterm TopicsSamantha VeraNo ratings yet
- Assessing The Caring Behaviors of Critical Care NursesDocument10 pagesAssessing The Caring Behaviors of Critical Care NursesMarc Andreo MalalaNo ratings yet
- Kashish KewalramaniDocument36 pagesKashish Kewalramanipriyanshu kesarwaniNo ratings yet
- Promkes Jurnal 3Document13 pagesPromkes Jurnal 3Sundawati AmdNo ratings yet
- MBA (2-Year Full-Time) : A Term PaperDocument25 pagesMBA (2-Year Full-Time) : A Term PaperpriyankaNo ratings yet
- Research Proposal - Health CareDocument12 pagesResearch Proposal - Health Carenirmaldeval100% (1)
- A Preliminary Study On Applying Holistic Health Care Model On Medical Education Behavioral Intention: A Theoretical Perspective of Planned BehaviorDocument7 pagesA Preliminary Study On Applying Holistic Health Care Model On Medical Education Behavioral Intention: A Theoretical Perspective of Planned BehaviorJean o LeraNo ratings yet
- Jungalwal Committee Report PDFDocument47 pagesJungalwal Committee Report PDFAnand gowdaNo ratings yet
- Study Guide 1 CHN 2Document9 pagesStudy Guide 1 CHN 2Hilario. Hayascent.Reign.M.No ratings yet
- Reflection Paper Hospital AdministrationDocument9 pagesReflection Paper Hospital AdministrationIvy PulidoNo ratings yet
- Factors Affecting Professional Ethics in Nursing Practice in Iran: A Qualitative StudyDocument7 pagesFactors Affecting Professional Ethics in Nursing Practice in Iran: A Qualitative StudyAliyahDennishaPhillipsNo ratings yet
- Research Report Healthcare Delivery Management To Improve The Primary Healthcare Services and Universal Health Care in ThailandDocument49 pagesResearch Report Healthcare Delivery Management To Improve The Primary Healthcare Services and Universal Health Care in Thailandsri_cbm0% (1)
- Management Control System - A Case Study of Rural Hospital of Salboni Block, Paschim MedinipurDocument6 pagesManagement Control System - A Case Study of Rural Hospital of Salboni Block, Paschim MedinipurKankana DeNo ratings yet
- The Interprofessional Approach To Patient ManagementDocument16 pagesThe Interprofessional Approach To Patient ManagementDarwin D. J. LimNo ratings yet
- IndianJCommunityMed 2015 40 2 85 153869Document7 pagesIndianJCommunityMed 2015 40 2 85 153869Duy HoNo ratings yet
- Major Stakeholders in HCSDocument13 pagesMajor Stakeholders in HCSVeeresh TopalakattiNo ratings yet
- Chapter 4: Issues in Contemporary Nursing Leadership: Situating The Topic: The Nature of The IssueDocument31 pagesChapter 4: Issues in Contemporary Nursing Leadership: Situating The Topic: The Nature of The IssueMaria PisanoNo ratings yet
- MAnoj Project ReportDocument35 pagesMAnoj Project Report01ayush.07No ratings yet
- Nurses Perceptions of Self Management and Self Management Su - 2021 - GeriatricDocument8 pagesNurses Perceptions of Self Management and Self Management Su - 2021 - GeriatricMaRice Mar RiceNo ratings yet
- Hospital Adminstration1Document99 pagesHospital Adminstration1Afreen Muxtaq100% (3)
- Major Stakeholders Satyajit MamDocument11 pagesMajor Stakeholders Satyajit MamAnchal thakurNo ratings yet
- Health Insurance and Third Party Administrators Issues and ChallengesDocument25 pagesHealth Insurance and Third Party Administrators Issues and ChallengesANish AhmedNo ratings yet
- Hme 2301 Topic 1Document8 pagesHme 2301 Topic 1Mofy AllyNo ratings yet
- Ethics For Hospital AdministrationDocument46 pagesEthics For Hospital AdministrationAnonymous ibmeej9100% (3)
- Jungalwal Committee ReportDocument47 pagesJungalwal Committee ReportKiran KumbharNo ratings yet
- District Mental Health Program - Need To Look Into Strategies in The Era of Mental Health Care Act, 2017 and Moving Beyond Bellary ModelDocument2 pagesDistrict Mental Health Program - Need To Look Into Strategies in The Era of Mental Health Care Act, 2017 and Moving Beyond Bellary ModelHarish KumarNo ratings yet
- Describes The Nursing CareDocument3 pagesDescribes The Nursing CareDiamond CraftNo ratings yet
- Case ManagementDocument7 pagesCase ManagementDev RNo ratings yet
- Hunter2012 The Integrative Medicine Team-Is Biomedical Dominance InevitableDocument6 pagesHunter2012 The Integrative Medicine Team-Is Biomedical Dominance InevitableSiu KiuNo ratings yet
- THE Impact OF Organizational Structure AND Administrative Polices of Hospitals On Delivering Quality of Service For Patients SatisfactionDocument10 pagesTHE Impact OF Organizational Structure AND Administrative Polices of Hospitals On Delivering Quality of Service For Patients SatisfactionAng Timotius Raymond AngkajayaNo ratings yet
- DI Virtual Health AcceleratedDocument20 pagesDI Virtual Health Acceleratedchetan NNo ratings yet
- Muthoot PRJCTDocument78 pagesMuthoot PRJCTAlex ValiyaveettilNo ratings yet
- NCM 104 Module 1m-2mDocument84 pagesNCM 104 Module 1m-2mJr CaniaNo ratings yet
- Organisational Behaviour Understanding People in Healthcare OrganisationsDocument17 pagesOrganisational Behaviour Understanding People in Healthcare OrganisationsJehan L.No ratings yet
- Homoeopathyin Public HealthDocument13 pagesHomoeopathyin Public HealthMegha MittalNo ratings yet
- Caring Behavior and Associated Factors Among Nurses Working in Jimma University Specialized Hospital, Oromia, Southwest Ethiopia, 2019Document7 pagesCaring Behavior and Associated Factors Among Nurses Working in Jimma University Specialized Hospital, Oromia, Southwest Ethiopia, 2019Ryrey Abraham PacamanaNo ratings yet
- Predictors of Nurse'S Caring Behavior Towards Patients With CriticalillnessDocument11 pagesPredictors of Nurse'S Caring Behavior Towards Patients With CriticalillnesssryNo ratings yet
- NURS-FPX 4010 Interdisciplinary Plan ProposalDocument8 pagesNURS-FPX 4010 Interdisciplinary Plan ProposalIrene WafulaNo ratings yet
- Sister Blessing Project.Document41 pagesSister Blessing Project.ayanfeNo ratings yet
- Communityhealthnursing 130426041331 Phpapp02Document46 pagesCommunityhealthnursing 130426041331 Phpapp02Fredrick WedderburnNo ratings yet
- OBM752 HM Unit-I NotesDocument12 pagesOBM752 HM Unit-I NotesRajanNo ratings yet
- Obm752 Hospital Management 1629103400 HMT NotesDocument104 pagesObm752 Hospital Management 1629103400 HMT NotesAyisha SiddhikaNo ratings yet
- COMMUNITY HEALTH NURSING CONCEPTS Topic 2Document25 pagesCOMMUNITY HEALTH NURSING CONCEPTS Topic 2Ciedelle Honey Lou DimaligNo ratings yet
- 0rder 271 NRS-493 - PROFESSIONAL CAPSTONE & PRACTICUMDocument18 pages0rder 271 NRS-493 - PROFESSIONAL CAPSTONE & PRACTICUMjoshua chegeNo ratings yet
- The Specialty of Community Health NursingDocument14 pagesThe Specialty of Community Health Nursingbanana cueNo ratings yet
- PRESENTATION: Health System Assessment Framework For Integrated CareDocument19 pagesPRESENTATION: Health System Assessment Framework For Integrated CareADB Health Sector GroupNo ratings yet
- Swot Analysis in Establishment of Nursing Service Quality in RS. TK. III DR Reksodiwiryo PadangDocument6 pagesSwot Analysis in Establishment of Nursing Service Quality in RS. TK. III DR Reksodiwiryo PadangInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- PUB 128 Topic 4Document74 pagesPUB 128 Topic 4Alfred NyagawaNo ratings yet
- Comprehensive Health Care ServicesDocument18 pagesComprehensive Health Care ServicesHamisu Tafashiya100% (1)
- Knowledge and Anxiety of The Covid-19 Vaccination Program For Teachers and Employees of SD Kreatif Muhammadiyah GombongDocument5 pagesKnowledge and Anxiety of The Covid-19 Vaccination Program For Teachers and Employees of SD Kreatif Muhammadiyah GombongNopriyan PujokusumaNo ratings yet
- Pentingnya Vaksinasi Dalam Membentuk Adaptive ImmunityDocument6 pagesPentingnya Vaksinasi Dalam Membentuk Adaptive ImmunityNopriyan PujokusumaNo ratings yet
- Corrigendum To Determinants of All-Cause In-HospitDocument3 pagesCorrigendum To Determinants of All-Cause In-HospitNopriyan PujokusumaNo ratings yet
- Hospital Management: January 2022Document6 pagesHospital Management: January 2022Nopriyan PujokusumaNo ratings yet
- UI Design of Business Intelligence For Various Levels Hospital ManagerDocument13 pagesUI Design of Business Intelligence For Various Levels Hospital ManagerNopriyan PujokusumaNo ratings yet
- 10 Hospital ManagementDocument22 pages10 Hospital ManagementNopriyan PujokusumaNo ratings yet
- ReferenceDocument4 pagesReferenceNopriyan PujokusumaNo ratings yet
- Stress ManagementDocument33 pagesStress ManagementShaells JoshiNo ratings yet
- Adhesive Film & TapeDocument6 pagesAdhesive Film & TapeJothi Vel MuruganNo ratings yet
- Story 1Document3 pagesStory 1api-296631749No ratings yet
- Case StudyDocument2 pagesCase StudyFadhlin Sakina SaadNo ratings yet
- Ultrasonic Based Distance Measurement SystemDocument18 pagesUltrasonic Based Distance Measurement SystemAman100% (2)
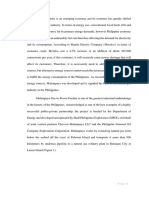
- Malampaya Case StudyDocument15 pagesMalampaya Case StudyMark Kenneth ValerioNo ratings yet
- Data Structures and Algorithms SyllabusDocument9 pagesData Structures and Algorithms SyllabusBongbong GalloNo ratings yet
- Ajsl DecisionMakingModel4RoRoDocument11 pagesAjsl DecisionMakingModel4RoRolesta putriNo ratings yet
- Module 4 How To Make Self-Rescue Evacuation Maps?Document85 pagesModule 4 How To Make Self-Rescue Evacuation Maps?RejieNo ratings yet
- Elementary Electronics 1968-09-10Document108 pagesElementary Electronics 1968-09-10Jim ToewsNo ratings yet
- AT10 Meat Tech 1Document20 pagesAT10 Meat Tech 1Reubal Jr Orquin Reynaldo100% (1)
- FT FocusDocument19 pagesFT Focusobi1kenobyNo ratings yet
- Unit 2 Operations of PolynomialsDocument28 pagesUnit 2 Operations of Polynomialsapi-287816312No ratings yet
- Cuentos CADEDocument6 pagesCuentos CADEMäuricio E. González VegaNo ratings yet
- Book Review Fiction New HereDocument7 pagesBook Review Fiction New HereFILZAH SYAUQINA BINTI SUBLY Pelajar KPTM IpohNo ratings yet
- UK Tabloids and Broadsheet NewspapersDocument14 pagesUK Tabloids and Broadsheet NewspapersBianca KissNo ratings yet
- Topic 6 Nested For LoopsDocument21 pagesTopic 6 Nested For Loopsthbull02No ratings yet
- Encapsulation of Objects and Methods in C++Document46 pagesEncapsulation of Objects and Methods in C++Scott StanleyNo ratings yet
- Andromeda: Druid 3 Warborn06Document5 pagesAndromeda: Druid 3 Warborn06AlanNo ratings yet
- Present Perfect Tense ExerciseDocument13 pagesPresent Perfect Tense Exercise39. Nguyễn Đăng QuangNo ratings yet
- Eureka Math Grade 2 Module 3 Parent Tip Sheet 1Document2 pagesEureka Math Grade 2 Module 3 Parent Tip Sheet 1api-324573119No ratings yet
- Chapter 10 Planetary Atmospheres: Earth and The Other Terrestrial WorldsDocument27 pagesChapter 10 Planetary Atmospheres: Earth and The Other Terrestrial WorldsEdwin ChuenNo ratings yet
- Presentation No. 3 - Songs and ChantsDocument44 pagesPresentation No. 3 - Songs and Chantsandie hinchNo ratings yet
- Template Remarks For IIDocument18 pagesTemplate Remarks For IIjasleeneceNo ratings yet
- Quarter 4 Week 1 EnglishDocument62 pagesQuarter 4 Week 1 EnglishJanine Jordan Canlas-BacaniNo ratings yet
- Eco EssayDocument3 pagesEco EssaymanthanNo ratings yet
- Npad PGP2017-19Document3 pagesNpad PGP2017-19Nikhil BhattNo ratings yet
- Technical and Business WritingDocument3 pagesTechnical and Business WritingMuhammad FaisalNo ratings yet
- Blank FacebookDocument2 pagesBlank Facebookapi-355481535No ratings yet
- Islcollective Present SimpleDocument2 pagesIslcollective Present Simplecrisan mirunaNo ratings yet
- Intraoperative RecordDocument2 pagesIntraoperative Recordademaala06100% (1)
- 12 Months to $1 Million: How to Pick a Winning Product, Build a Real Business, and Become a Seven-Figure EntrepreneurFrom Everand12 Months to $1 Million: How to Pick a Winning Product, Build a Real Business, and Become a Seven-Figure EntrepreneurRating: 4 out of 5 stars4/5 (2)
- The Millionaire Fastlane, 10th Anniversary Edition: Crack the Code to Wealth and Live Rich for a LifetimeFrom EverandThe Millionaire Fastlane, 10th Anniversary Edition: Crack the Code to Wealth and Live Rich for a LifetimeRating: 4.5 out of 5 stars4.5/5 (90)
- To Pixar and Beyond: My Unlikely Journey with Steve Jobs to Make Entertainment HistoryFrom EverandTo Pixar and Beyond: My Unlikely Journey with Steve Jobs to Make Entertainment HistoryRating: 4 out of 5 stars4/5 (26)
- Secrets of the Millionaire Mind: Mastering the Inner Game of WealthFrom EverandSecrets of the Millionaire Mind: Mastering the Inner Game of WealthRating: 4.5 out of 5 stars4.5/5 (1027)
- Summary of Zero to One: Notes on Startups, or How to Build the FutureFrom EverandSummary of Zero to One: Notes on Startups, or How to Build the FutureRating: 4.5 out of 5 stars4.5/5 (100)
- Take Your Shot: How to Grow Your Business, Attract More Clients, and Make More MoneyFrom EverandTake Your Shot: How to Grow Your Business, Attract More Clients, and Make More MoneyRating: 5 out of 5 stars5/5 (22)
- Transformed: Moving to the Product Operating ModelFrom EverandTransformed: Moving to the Product Operating ModelRating: 4 out of 5 stars4/5 (1)
- Cryptocurrency for Beginners: A Complete Guide to Understanding the Crypto Market from Bitcoin, Ethereum and Altcoins to ICO and Blockchain TechnologyFrom EverandCryptocurrency for Beginners: A Complete Guide to Understanding the Crypto Market from Bitcoin, Ethereum and Altcoins to ICO and Blockchain TechnologyRating: 4.5 out of 5 stars4.5/5 (300)
- Summary of The Four Agreements: A Practical Guide to Personal Freedom (A Toltec Wisdom Book) by Don Miguel RuizFrom EverandSummary of The Four Agreements: A Practical Guide to Personal Freedom (A Toltec Wisdom Book) by Don Miguel RuizRating: 4.5 out of 5 stars4.5/5 (112)
- The Millionaire Fastlane: Crack the Code to Wealth and Live Rich for a LifetimeFrom EverandThe Millionaire Fastlane: Crack the Code to Wealth and Live Rich for a LifetimeRating: 4.5 out of 5 stars4.5/5 (58)
- The Master Key System: 28 Parts, Questions and AnswersFrom EverandThe Master Key System: 28 Parts, Questions and AnswersRating: 5 out of 5 stars5/5 (62)
- 24 Assets: Create a digital, scalable, valuable and fun business that will thrive in a fast changing worldFrom Everand24 Assets: Create a digital, scalable, valuable and fun business that will thrive in a fast changing worldRating: 5 out of 5 stars5/5 (20)
- SYSTEMology: Create time, reduce errors and scale your profits with proven business systemsFrom EverandSYSTEMology: Create time, reduce errors and scale your profits with proven business systemsRating: 5 out of 5 stars5/5 (48)
- ChatGPT Side Hustles 2024 - Unlock the Digital Goldmine and Get AI Working for You Fast with More Than 85 Side Hustle Ideas to Boost Passive Income, Create New Cash Flow, and Get Ahead of the CurveFrom EverandChatGPT Side Hustles 2024 - Unlock the Digital Goldmine and Get AI Working for You Fast with More Than 85 Side Hustle Ideas to Boost Passive Income, Create New Cash Flow, and Get Ahead of the CurveNo ratings yet
- Rich Dad's Before You Quit Your Job: 10 Real-Life Lessons Every Entrepreneur Should Know About Building a Multimillion-Dollar BusinessFrom EverandRich Dad's Before You Quit Your Job: 10 Real-Life Lessons Every Entrepreneur Should Know About Building a Multimillion-Dollar BusinessRating: 4.5 out of 5 stars4.5/5 (407)
- Every Tool's a Hammer: Life Is What You Make ItFrom EverandEvery Tool's a Hammer: Life Is What You Make ItRating: 4.5 out of 5 stars4.5/5 (249)
- Summary: Choose Your Enemies Wisely: Business Planning for the Audacious Few: Key Takeaways, Summary and AnalysisFrom EverandSummary: Choose Your Enemies Wisely: Business Planning for the Audacious Few: Key Takeaways, Summary and AnalysisRating: 4.5 out of 5 stars4.5/5 (3)
- The Science of Positive Focus: Live Seminar: Master Keys for Reaching Your Next LevelFrom EverandThe Science of Positive Focus: Live Seminar: Master Keys for Reaching Your Next LevelRating: 5 out of 5 stars5/5 (51)
- Summary of The Subtle Art of Not Giving A F*ck: A Counterintuitive Approach to Living a Good Life by Mark Manson: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary of The Subtle Art of Not Giving A F*ck: A Counterintuitive Approach to Living a Good Life by Mark Manson: Key Takeaways, Summary & Analysis IncludedRating: 4.5 out of 5 stars4.5/5 (38)
- Brand Identity Breakthrough: How to Craft Your Company's Unique Story to Make Your Products IrresistibleFrom EverandBrand Identity Breakthrough: How to Craft Your Company's Unique Story to Make Your Products IrresistibleRating: 4.5 out of 5 stars4.5/5 (48)
- Enough: The Simple Path to Everything You Want -- A Field Guide for Perpetually Exhausted EntrepreneursFrom EverandEnough: The Simple Path to Everything You Want -- A Field Guide for Perpetually Exhausted EntrepreneursRating: 5 out of 5 stars5/5 (24)
- 7 Secrets to Investing Like Warren BuffettFrom Everand7 Secrets to Investing Like Warren BuffettRating: 4.5 out of 5 stars4.5/5 (121)
- The E-Myth Revisited: Why Most Small Businesses Don't Work andFrom EverandThe E-Myth Revisited: Why Most Small Businesses Don't Work andRating: 4.5 out of 5 stars4.5/5 (709)
- Summary of The E-Myth Revisited: Why Most Small Businesses Don't Work and What to Do About It by Michael E. GerberFrom EverandSummary of The E-Myth Revisited: Why Most Small Businesses Don't Work and What to Do About It by Michael E. GerberRating: 5 out of 5 stars5/5 (39)
- Summary: Who Not How: The Formula to Achieve Bigger Goals Through Accelerating Teamwork by Dan Sullivan & Dr. Benjamin Hardy:From EverandSummary: Who Not How: The Formula to Achieve Bigger Goals Through Accelerating Teamwork by Dan Sullivan & Dr. Benjamin Hardy:Rating: 5 out of 5 stars5/5 (2)
- Your Next Five Moves: Master the Art of Business StrategyFrom EverandYour Next Five Moves: Master the Art of Business StrategyRating: 5 out of 5 stars5/5 (802)
- Level Up: How to Get Focused, Stop Procrastinating, and Upgrade Your LifeFrom EverandLevel Up: How to Get Focused, Stop Procrastinating, and Upgrade Your LifeRating: 5 out of 5 stars5/5 (22)
- Built to Serve: Find Your Purpose and Become the Leader You Were Born to BeFrom EverandBuilt to Serve: Find Your Purpose and Become the Leader You Were Born to BeRating: 5 out of 5 stars5/5 (24)
- Startup: How To Create A Successful, Scalable, High-Growth Business From ScratchFrom EverandStartup: How To Create A Successful, Scalable, High-Growth Business From ScratchRating: 4 out of 5 stars4/5 (114)