You might also like
- Endodontic RadiologyFrom EverandEndodontic RadiologyBettina BasraniNo ratings yet
- University of St. La Salle College of NursingDocument12 pagesUniversity of St. La Salle College of Nursingeboy babotNo ratings yet
- University of St. La Salle College of NursingDocument12 pagesUniversity of St. La Salle College of Nursingeboy babotNo ratings yet
- University of St. La Salle College of NursingDocument12 pagesUniversity of St. La Salle College of Nursingeboy babotNo ratings yet
- Min 3-4 CLDocument12 pagesMin 3-4 CLeboy babotNo ratings yet
- University of St. La Salle College of Nursing: Gargar, Larry Jun SumbiDocument10 pagesUniversity of St. La Salle College of Nursing: Gargar, Larry Jun Sumbieboy babotNo ratings yet
- College of St. John - Roxas: de La Salle SupervisedDocument4 pagesCollege of St. John - Roxas: de La Salle Supervisedabbyjuv28No ratings yet
- CDD Sample CaseloadDocument9 pagesCDD Sample CaseloadAijem RyanNo ratings yet
- Cases Form 2007Document5 pagesCases Form 2007Shandz de RosasNo ratings yet
- Jalbuena, Andrew MontinolaDocument20 pagesJalbuena, Andrew MontinolawestnegrosNo ratings yet
- PRC-Final Form 20111Document7 pagesPRC-Final Form 20111Jeremy_Fabio_5332No ratings yet
- Ronie PRCDocument2 pagesRonie PRCmaeronieNo ratings yet
- PRC Forms AdzuDocument14 pagesPRC Forms AdzushaneequaNo ratings yet
- De Los Santos-Sti College, Inc: ODC Form 2B or Minor FormDocument2 pagesDe Los Santos-Sti College, Inc: ODC Form 2B or Minor FormRobert Ross DulayNo ratings yet
- España Boulevard, Sampaloc, Manila, Philippines 1015 Tel. No. 406-1611 Loc.8241 Telefax: 731-5738 WebsiteDocument1 pageEspaña Boulevard, Sampaloc, Manila, Philippines 1015 Tel. No. 406-1611 Loc.8241 Telefax: 731-5738 WebsiteNyeam NyeamNo ratings yet
- STI College - Zamboanga Unicon Building, Gen. Wood Street Gov.Document2 pagesSTI College - Zamboanga Unicon Building, Gen. Wood Street Gov.Amirkhan SappayaniNo ratings yet
- Procedure Performed: Benguet State University College of NursingDocument3 pagesProcedure Performed: Benguet State University College of NursingAudi Kyle SaydovenNo ratings yet
- PRC Forms NEW GUIDELINEDocument7 pagesPRC Forms NEW GUIDELINEJellyAnnGomezNo ratings yet
- España Boulevard, Sampaloc, Manila, Philippines 1015 Tel. No. 406-1611 Loc.8241 Telefax: 731-5738 WebsiteDocument1 pageEspaña Boulevard, Sampaloc, Manila, Philippines 1015 Tel. No. 406-1611 Loc.8241 Telefax: 731-5738 WebsiteNyeam NyeamNo ratings yet
- Case FormDocument6 pagesCase Formmilkman16No ratings yet
- STI STI College - Zamboanga Unicon Building, Gen. Wood StreetDocument7 pagesSTI STI College - Zamboanga Unicon Building, Gen. Wood Streetzacht_18100% (1)
- Good Samaritan CollegesDocument3 pagesGood Samaritan Collegesdimple2718No ratings yet
- PRC Form New Format 2010 Western Mindanao State UniversityDocument5 pagesPRC Form New Format 2010 Western Mindanao State UniversityjefzisgoodNo ratings yet
- Format Compact Case Loads UPCNDocument5 pagesFormat Compact Case Loads UPCNPaul Christian P. Santos, RNNo ratings yet
- SMC Tagum PRC NewDocument6 pagesSMC Tagum PRC NewDhandei31No ratings yet
- España Boulevard, Sampaloc, Manila, Philippines 1015 Tel. No. 406-1611 Loc.8241 Telefax: 731-5738 WebsiteDocument1 pageEspaña Boulevard, Sampaloc, Manila, Philippines 1015 Tel. No. 406-1611 Loc.8241 Telefax: 731-5738 WebsiteNyeam NyeamNo ratings yet
- Manila Doctors College - PRC Form SamplesDocument6 pagesManila Doctors College - PRC Form Samplespaolo_planasNo ratings yet
- TemplatesDocument10 pagesTemplatesmagicnikkiNo ratings yet
- Colegio de Dagupan Sample CaseloadDocument6 pagesColegio de Dagupan Sample CaseloadAijem RyanNo ratings yet
- De La Salle Health Sciences Institute Surgical Scrub FormDocument2 pagesDe La Salle Health Sciences Institute Surgical Scrub FormDominic BristolNo ratings yet
- Our Lady of Fatima University: I. Major OperationsDocument5 pagesOur Lady of Fatima University: I. Major OperationsMaja AbellaNo ratings yet
- PRC FORM CVMC - EditedDocument5 pagesPRC FORM CVMC - EditedEver NavarroNo ratings yet
- Odc Form 2aDocument5 pagesOdc Form 2aquiabenjchNo ratings yet
- 4thyr. ZCMC Scrub MinorDocument1 page4thyr. ZCMC Scrub MinorLey BeltranNo ratings yet
- Zamboanga City Medical Center, Zamboanga City: Surgical Procedure PerformedDocument1 pageZamboanga City Medical Center, Zamboanga City: Surgical Procedure PerformedAlmira AhamadNo ratings yet
- O.R. Form 1B at Ateneo de Zamboanga UniversityDocument1 pageO.R. Form 1B at Ateneo de Zamboanga UniversityJaiton PagayonanNo ratings yet
- University of San Agustin College of Nursing Iloilo City As Per BON-PRC Resolution No. 357 Series of 2004 College of NursingDocument8 pagesUniversity of San Agustin College of Nursing Iloilo City As Per BON-PRC Resolution No. 357 Series of 2004 College of NursingSkaaj007No ratings yet
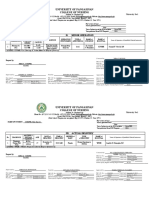
- University of Pangasinan College of Nursing: II. Minor OperationDocument6 pagesUniversity of Pangasinan College of Nursing: II. Minor Operationmiss_rizaNo ratings yet
- PRC Cases FormatDocument5 pagesPRC Cases FormatalexisalvioNo ratings yet
- Ub@ubaguio - Edu: ODC Form 2A O.R. Scrub Form MajorDocument26 pagesUb@ubaguio - Edu: ODC Form 2A O.R. Scrub Form MajorKitz GarciaNo ratings yet
- Circu-O RDocument1 pageCircu-O RSanny RamosNo ratings yet
- Actual DeliveriesDocument1 pageActual Deliverieskazuya143No ratings yet
- Exclusive For GRP ImbaDocument8 pagesExclusive For GRP Imbacsy123No ratings yet
- Republic of The Philippines: ODC Form 1 O.R. Scrub FormDocument8 pagesRepublic of The Philippines: ODC Form 1 O.R. Scrub FormghelzoneNo ratings yet
- Golden Gate Colleges P. Prieto ST., Batangas CityDocument4 pagesGolden Gate Colleges P. Prieto ST., Batangas CityR ArcegaNo ratings yet
- S M C L: Aint Ichael'S Ollege of AgunaDocument12 pagesS M C L: Aint Ichael'S Ollege of AgunaChriza Joy BartolomeNo ratings yet
- Tarlac State University: Romulo Blvd. San Vicente, Tarlac City (045) 493-1865/ Telefax. (045) 982-0110/ WWW - Tsu.edu - PHDocument5 pagesTarlac State University: Romulo Blvd. San Vicente, Tarlac City (045) 493-1865/ Telefax. (045) 982-0110/ WWW - Tsu.edu - PHXIEROINNo ratings yet
- Benguet State University College of Nursing: Procedure PerformedDocument3 pagesBenguet State University College of Nursing: Procedure PerformedAudi Kyle SaydovenNo ratings yet
- Case Format IV Deliveries AssisstedDocument1 pageCase Format IV Deliveries Assisstedakosiechel9311No ratings yet
- Major Circu BlankDocument2 pagesMajor Circu BlankAizha Noelle CataminNo ratings yet
- Sang AliDocument2 pagesSang AliSofia_Ajihil_486No ratings yet
- Ateneo Zamboanga Nursing FormsDocument17 pagesAteneo Zamboanga Nursing FormsRyan MirandaNo ratings yet
- Guiwan Main Health Center and Lying-In Clinic, Zamboanga CityDocument17 pagesGuiwan Main Health Center and Lying-In Clinic, Zamboanga CityRyan MirandaNo ratings yet
- Actual Delivery FormsDocument7 pagesActual Delivery Formswicked_shadow21No ratings yet
- Final PRC DR Sample TemplateDocument4 pagesFinal PRC DR Sample TemplatenovelloveNo ratings yet
- Philip Sugaton COMK_3E Class StrategiesDocument1 pagePhilip Sugaton COMK_3E Class StrategiesPrincess Faniega SugatonNo ratings yet
- 4 Sustainable Development GoalsDocument2 pages4 Sustainable Development GoalsPrincess Faniega SugatonNo ratings yet
- 1 s2.0 S089718972030063X MainDocument9 pages1 s2.0 S089718972030063X MainPrincess Faniega SugatonNo ratings yet
- The 3 Levels of Artwork Meaning: Factual, Conventional, SubjectiveDocument1 pageThe 3 Levels of Artwork Meaning: Factual, Conventional, SubjectivePrincess Faniega SugatonNo ratings yet
- Peter STS - S MISS PAT FinalssDocument2 pagesPeter STS - S MISS PAT FinalssPrincess Faniega SugatonNo ratings yet
- Self Assessment SwimmingDocument1 pageSelf Assessment SwimmingPrincess Faniega SugatonNo ratings yet
- Minosa LipidsDocument4 pagesMinosa LipidsPrincess Faniega SugatonNo ratings yet
- Module3 Second-Assignment BatallonDocument6 pagesModule3 Second-Assignment BatallonPrincess Faniega SugatonNo ratings yet
- Beach Volleyball 2023 Open Tournament Registration FormDocument2 pagesBeach Volleyball 2023 Open Tournament Registration FormPrincess Faniega SugatonNo ratings yet
- Laboratory Exercise 7Document3 pagesLaboratory Exercise 7Princess Faniega SugatonNo ratings yet
- Casescenario4 CushingsyndromeDocument4 pagesCasescenario4 CushingsyndromePrincess Faniega SugatonNo ratings yet
- HEALTH-TEACHING-PLAN sUGATON EVALDocument9 pagesHEALTH-TEACHING-PLAN sUGATON EVALPrincess Faniega SugatonNo ratings yet
- Assisting in Nasogastric Tube Insertion 1 1Document14 pagesAssisting in Nasogastric Tube Insertion 1 1Princess Faniega SugatonNo ratings yet
- Addtl Digestive System ExercisesDocument3 pagesAddtl Digestive System ExercisesPrincess Faniega SugatonNo ratings yet
- Types of Traction An CareDocument1 pageTypes of Traction An CarePrincess Faniega SugatonNo ratings yet
- Types of Traction An CareDocument1 pageTypes of Traction An CarePrincess Faniega SugatonNo ratings yet
- JOHART PrincessDocument2 pagesJOHART PrincessPrincess Faniega SugatonNo ratings yet
- Head and Neck Muscle IdentificationDocument3 pagesHead and Neck Muscle IdentificationPrincess Faniega SugatonNo ratings yet
- Research Revised Results and DiscussionDocument13 pagesResearch Revised Results and DiscussionPrincess Faniega SugatonNo ratings yet
- Why History Study Is Vital for Young FilipinosDocument1 pageWhy History Study Is Vital for Young FilipinosPrincess Faniega SugatonNo ratings yet
- FATHIYOWNDocument1 pageFATHIYOWNPrincess Faniega SugatonNo ratings yet
- Irs3 Module5 Philipf JDocument2 pagesIrs3 Module5 Philipf JPrincess Faniega SugatonNo ratings yet
- Princess F. Sugaton BSN1-F HWPEDocument1 pagePrincess F. Sugaton BSN1-F HWPEPrincess Faniega SugatonNo ratings yet
- Princess F. Sugaton, Joseph Ritz Bayona BSN1-FDocument1 pagePrincess F. Sugaton, Joseph Ritz Bayona BSN1-FPrincess Faniega SugatonNo ratings yet
- PEC Self-Rating Questionnaire for Entrepreneurial TraitsDocument1 pagePEC Self-Rating Questionnaire for Entrepreneurial TraitsPrincess Faniega SugatonNo ratings yet
- Comlaw Exam EndtermDocument2 pagesComlaw Exam EndtermPrincess Faniega SugatonNo ratings yet
- Case Scenario 3 GerdDocument4 pagesCase Scenario 3 GerdPrincess Faniega SugatonNo ratings yet
- Drug Study Sugaton Week 1 2ND SemDocument3 pagesDrug Study Sugaton Week 1 2ND SemPrincess Faniega SugatonNo ratings yet
- Sugaton-Home-Visit-Record-Day 2Document1 pageSugaton-Home-Visit-Record-Day 2Princess Faniega SugatonNo ratings yet
- Case Discussion GerdDocument1 pageCase Discussion GerdPrincess Faniega SugatonNo ratings yet
- Notifications Post RN BSN Semester I II Exam 2023Document1 pageNotifications Post RN BSN Semester I II Exam 2023Shahzad Jawaid KhanNo ratings yet
- Six Building Blocks of Health SystemDocument19 pagesSix Building Blocks of Health SystemChala FekaduNo ratings yet
- Referral Slip - Friendlycare FoundationDocument1 pageReferral Slip - Friendlycare Foundationmathhew bepplerNo ratings yet
- Valenzuela AOP 2022 Enhanced Form 3.2Document8 pagesValenzuela AOP 2022 Enhanced Form 3.2John Philip TiongcoNo ratings yet
- 30 Day Readmission Article ReviewDocument4 pages30 Day Readmission Article ReviewKIPNGENO EMMANUELNo ratings yet
- HSSP V 17-06-2021 FinalDocument106 pagesHSSP V 17-06-2021 FinalAlexander MachokeNo ratings yet
- Ten Physicians and Local Execs Indicted in Pharmacy Kickback Scheme - D MagazineDocument5 pagesTen Physicians and Local Execs Indicted in Pharmacy Kickback Scheme - D MagazineseenfgNo ratings yet
- Acupuncture 2023Document1 pageAcupuncture 2023Randheer Kumar AnnarapuNo ratings yet
- Dr Noor Kamil's Guide to Effective Medication CounselingDocument8 pagesDr Noor Kamil's Guide to Effective Medication Counselingdaniya nadeemNo ratings yet
- Informantional Reaserch Essay 1Document3 pagesInformantional Reaserch Essay 1api-615817090No ratings yet
- Chn-Health-Related Activities in The CommunityDocument3 pagesChn-Health-Related Activities in The CommunityBSN 1-N CASTRO, RicciNo ratings yet
- The Petty Cash BookDocument3 pagesThe Petty Cash Bookaarifah mNo ratings yet
- SSP032 M5 SDG3Document23 pagesSSP032 M5 SDG3Henry Darius NamocNo ratings yet
- Marissa Putri, MDDocument5 pagesMarissa Putri, MDMarissa Putri WahabNo ratings yet
- Daily Ward AssignmentsDocument4 pagesDaily Ward AssignmentsMia Labrador Sta CruzNo ratings yet
- NYE CAID EnrollmentReqNoticeDocument2 pagesNYE CAID EnrollmentReqNoticeLuke ParsnowNo ratings yet
- BSNL Contact NumberDocument2 pagesBSNL Contact NumberalokpyasiNo ratings yet
- Sap June 2021Document32 pagesSap June 2021self sayidNo ratings yet
- PNP Command StructureDocument2 pagesPNP Command StructureIanli QuinanolaNo ratings yet
- Baguio Sewage Treatment Plant 1Document8 pagesBaguio Sewage Treatment Plant 1Reden Salve PionNo ratings yet
- Healthcare Domain QuestionsDocument5 pagesHealthcare Domain QuestionsNikhil SatavNo ratings yet
- Design8 - Researchno2 Tertiary HospitalDocument122 pagesDesign8 - Researchno2 Tertiary HospitalBess Adrane JurolanNo ratings yet
- 2023 Calendar with Indian HolidaysDocument1 page2023 Calendar with Indian HolidaysMrunali SomawaneNo ratings yet
- Managing Individual National Address - National Address RegistrationDocument2 pagesManaging Individual National Address - National Address RegistrationAbdul Rahman100% (1)
- Bus Times: Bootle - Aigburth ValeDocument7 pagesBus Times: Bootle - Aigburth ValeJordan PooleNo ratings yet
- CASE STUDY - 1 Connecting Patient Monitoring Devices to EHRsDocument4 pagesCASE STUDY - 1 Connecting Patient Monitoring Devices to EHRs7ossam AbduNo ratings yet
- KPME (Amendment) Rules, 2018 (Eng)Document11 pagesKPME (Amendment) Rules, 2018 (Eng)Nausheen AnsariNo ratings yet
- Track Shipment Status - Consignment Status - DTDC IndiaDocument1 pageTrack Shipment Status - Consignment Status - DTDC IndiazrahamanNo ratings yet
- Dwarka Sector 21 Metro Station - Sarai Kale Khan I.S.B.T.: DW-4 Bus Time Schedule & Line MapDocument4 pagesDwarka Sector 21 Metro Station - Sarai Kale Khan I.S.B.T.: DW-4 Bus Time Schedule & Line Mapsumit kumarNo ratings yet
- Arshith Jithendran Biomed NewDocument1 pageArshith Jithendran Biomed NewLulu MizbahNo ratings yet