You might also like
- (PSYCH) 6.3 Organizing Data in Psychiatric EvaluationDocument8 pages(PSYCH) 6.3 Organizing Data in Psychiatric EvaluationReggie Lyn BaricanNo ratings yet
- Psychiatric History SummaryDocument24 pagesPsychiatric History SummaryfahmiNo ratings yet
- Psychiatric History and ExaminationDocument14 pagesPsychiatric History and ExaminationPaolo Bonifacio100% (14)
- Prescribing Psychotropics: From Drug Interactions to PharmacogeneticsFrom EverandPrescribing Psychotropics: From Drug Interactions to PharmacogeneticsRating: 5 out of 5 stars5/5 (1)
- Assessment and Evaluation: 2008 Edition Rhoda K Hahn, MD Lawrence J. Albers, MDDocument85 pagesAssessment and Evaluation: 2008 Edition Rhoda K Hahn, MD Lawrence J. Albers, MDAlbghdadi CristianNo ratings yet
- Clinical Evaluation of The Psychiatric PatientDocument4 pagesClinical Evaluation of The Psychiatric Patienthannjazz100% (1)
- The Maudsley Prescribing Guidelines in PsychiatryFrom EverandThe Maudsley Prescribing Guidelines in PsychiatryRating: 4 out of 5 stars4/5 (1)
- The Psychiatric History: Functions and ComponentsDocument5 pagesThe Psychiatric History: Functions and ComponentsKeifer Turtle100% (2)
- Psychiatric History TakingDocument6 pagesPsychiatric History TakingNurul Nadzri100% (1)
- Psychiatric SheetDocument80 pagesPsychiatric SheetHigazi z'EagleNo ratings yet
- Psychiatry Made EasyDocument14 pagesPsychiatry Made EasyTinesh Rajah83% (6)
- 7718 (07) Review of Cases - Anxiety DisordersDocument34 pages7718 (07) Review of Cases - Anxiety DisordersnewazNo ratings yet
- History Taking in PsychiatryDocument3 pagesHistory Taking in PsychiatryJuan Cruz FenrirNo ratings yet
- H&P Template SummaryDocument1 pageH&P Template SummaryWilliam Yang100% (1)
- Disorders Duration/Onset Symptoms/Manifestations Treatment: Childhood DDocument7 pagesDisorders Duration/Onset Symptoms/Manifestations Treatment: Childhood DActeen Myoseen100% (1)
- Psychiatric Assessment ToolDocument53 pagesPsychiatric Assessment ToolLori100% (4)
- MSE Psychiatric InterviewingDocument26 pagesMSE Psychiatric InterviewingZonny PatelNo ratings yet
- Major Psychiatry Concepts for USMLE SuccessDocument28 pagesMajor Psychiatry Concepts for USMLE SuccessyepherenowNo ratings yet
- Psychiatry History Taking and Physical ExaminationDocument16 pagesPsychiatry History Taking and Physical ExaminationEma100% (17)
- 2011 09 PsychiatryDocument40 pages2011 09 PsychiatryGurpreet Chara100% (1)
- Psychiatric Case History NotesDocument8 pagesPsychiatric Case History NotesTysle100% (1)
- Psychiatry Study MaterialsDocument3 pagesPsychiatry Study Materialsgnanam ambalavananNo ratings yet
- History Taking and Psychiatric Interview GuideDocument18 pagesHistory Taking and Psychiatric Interview GuideMujeeb ChoudharyNo ratings yet
- Delirium and DementiaDocument12 pagesDelirium and DementiaardaineannramosNo ratings yet
- PsychiatryDocument95 pagesPsychiatryJarwoto RoestanajieNo ratings yet
- PSYCH 001 Psychiatric Interview of The Medically Ill PDFDocument10 pagesPSYCH 001 Psychiatric Interview of The Medically Ill PDFKaye Nee100% (1)
- Psychiatric Interview Kap ExtDocument61 pagesPsychiatric Interview Kap ExtNeba YenatuNo ratings yet
- Psych Interns - ManualDocument36 pagesPsych Interns - ManualDanielle Jann Manio Concepcion100% (5)
- Structured Approach To Acute Psychiatry EmergenciesDocument41 pagesStructured Approach To Acute Psychiatry EmergenciesRaimondo RomanazziNo ratings yet
- Resident's Guide To Clinical PsychiatryDocument412 pagesResident's Guide To Clinical PsychiatryJP Rajendran88% (16)
- Psychiatry textbook and reference guide collectionDocument4 pagesPsychiatry textbook and reference guide collectionIbrahimFikryNo ratings yet
- History Taking and Risk Assessment and MSE in PsychiatryDocument37 pagesHistory Taking and Risk Assessment and MSE in PsychiatrySanjay PaudelNo ratings yet
- Mental Status ExaminationDocument13 pagesMental Status ExaminationJosé Ramón Pérez-Accino100% (1)
- Ovid - Kaplan & Sadock Psychiatric InterviewDocument39 pagesOvid - Kaplan & Sadock Psychiatric InterviewIsa100% (1)
- Session 7 Psychiatric AssessmentDocument54 pagesSession 7 Psychiatric AssessmentPetroNo ratings yet
- History Taking in PsychiatryDocument3 pagesHistory Taking in PsychiatryReza Parker50% (2)
- Clinical Interview For Psychiatric AssessmentDocument63 pagesClinical Interview For Psychiatric Assessmentaadupavi100% (1)
- Clinical Methods in Psychiatry 2nd EditionDocument92 pagesClinical Methods in Psychiatry 2nd Editionprachirb100% (1)
- History Taking in PsychiatryDocument45 pagesHistory Taking in PsychiatryShashah Rau100% (3)
- Psychiatric Mnemonics & Clinical Guides ReviewDocument10 pagesPsychiatric Mnemonics & Clinical Guides ReviewAhmed HamidNo ratings yet
- Case History, MSE and Rating Scales - in Psychological AssessmentDocument29 pagesCase History, MSE and Rating Scales - in Psychological Assessmentsu84No ratings yet
- History Taking Scheme PsychiatryDocument2 pagesHistory Taking Scheme PsychiatryaliNo ratings yet
- Dopamine HypothesisDocument2 pagesDopamine HypothesisBo123456100% (2)
- Mental Status ExaminationDocument72 pagesMental Status Examinationsherief marouf100% (1)
- PMHNP Case Study Diagnosis and TreatmentDocument7 pagesPMHNP Case Study Diagnosis and TreatmentSoumyadeep BoseNo ratings yet
- Adult Psychiatry II: Paper B Syllabic Content 7.1xDocument27 pagesAdult Psychiatry II: Paper B Syllabic Content 7.1xJasonNo ratings yet
- USM Psychiatry Student GuideDocument43 pagesUSM Psychiatry Student GuideAhmad Syahmi YZ100% (1)
- PsychiatryDocument92 pagesPsychiatrykimNo ratings yet
- Psychiatric History GuideDocument8 pagesPsychiatric History GuideBobet ReñaNo ratings yet
- Psychiatry HX TakingDocument4 pagesPsychiatry HX TakingP KasikrishnarajaNo ratings yet
- HPI GuidelinesDocument5 pagesHPI GuidelinesHani NadiahNo ratings yet
- Mental Status Exam ChecklistDocument6 pagesMental Status Exam ChecklistainstusharNo ratings yet
- Mental Status Examination Rapid Record Form: CatatoniaDocument3 pagesMental Status Examination Rapid Record Form: CatatoniaNicole TangcoNo ratings yet
- Pharmacology - (5) Psychotic DrugsDocument8 pagesPharmacology - (5) Psychotic DrugsSamantha DiegoNo ratings yet
- 71 AdultPsychiatry Part1 PDFDocument42 pages71 AdultPsychiatry Part1 PDFCetVital100% (1)
- IM-Module B Summarized Notes (IBD)Document69 pagesIM-Module B Summarized Notes (IBD)DeepbluexNo ratings yet
- All-In CPT Prelims Pepsi 2024Document22 pagesAll-In CPT Prelims Pepsi 2024DeepbluexNo ratings yet
- Drug List by Therapeutic Category: Cardiovascular DrugsDocument7 pagesDrug List by Therapeutic Category: Cardiovascular DrugsAloah122346No ratings yet
- 2022 Sept 30 DpriDocument51 pages2022 Sept 30 DpriChari RivoNo ratings yet
- IM Cardiology Samplex All-In - LDocument35 pagesIM Cardiology Samplex All-In - LDeepbluexNo ratings yet
- 3-13-23 REVISED - Ward Sched 2nd SEM 3RD LOCALDocument8 pages3-13-23 REVISED - Ward Sched 2nd SEM 3RD LOCALDeepbluexNo ratings yet
- Cochane Data Extraction FormDocument11 pagesCochane Data Extraction FormDeepbluexNo ratings yet
- (Sgy Samplex Prelim 2) Surgery-Remedial-ReviewerDocument21 pages(Sgy Samplex Prelim 2) Surgery-Remedial-ReviewerDeepbluexNo ratings yet
- The family as a unit of careDocument273 pagesThe family as a unit of careDeepbluexNo ratings yet
- HEENT Checklist for Clinical MedicineDocument2 pagesHEENT Checklist for Clinical MedicineDeepbluexNo ratings yet
- 7.0 (Micro Mynotes Prelim 2) Diencephalon - Thalamus, HypothalamusDocument5 pages7.0 (Micro Mynotes Prelim 2) Diencephalon - Thalamus, HypothalamusDeepbluexNo ratings yet
- 19.2 (Micro Mynotes Midterm 2) Ascending and Descending TractsDocument10 pages19.2 (Micro Mynotes Midterm 2) Ascending and Descending TractsDeepbluexNo ratings yet
- Cardiovascular Examination A. 1. Wash Hands Before Touching Patient, B. 2. Explain What You Like To Do & ObtainDocument2 pagesCardiovascular Examination A. 1. Wash Hands Before Touching Patient, B. 2. Explain What You Like To Do & ObtainDeepbluexNo ratings yet
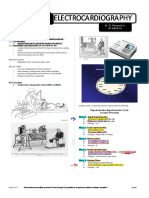
- ECG machine study of heart electrical activityDocument7 pagesECG machine study of heart electrical activityDeepbluexNo ratings yet
- 5 +Spine+&+Ext+Pe+ChecklistDocument3 pages5 +Spine+&+Ext+Pe+ChecklistDeepbluexNo ratings yet
- Normal Flora, Bacteria, and DiseaseDocument8 pagesNormal Flora, Bacteria, and DiseaseDeepbluexNo ratings yet
- GeneticsDocument4 pagesGeneticsDeepbluexNo ratings yet
- Code of Ethics for PhysiciansDocument3 pagesCode of Ethics for PhysiciansDeepbluexNo ratings yet
- Fasciolopsis Buski Echinostoma Ilocanum Heterophyes Heterophyes Metagonimus Yokogawai Haplorchis YokogawaiDocument26 pagesFasciolopsis Buski Echinostoma Ilocanum Heterophyes Heterophyes Metagonimus Yokogawai Haplorchis YokogawaiDeepbluexNo ratings yet
- WMA Code of Ethics: Duties of Physicians in General Duties of Physicians To PatientsDocument2 pagesWMA Code of Ethics: Duties of Physicians in General Duties of Physicians To PatientsDeepbluexNo ratings yet
- Theoretical FrameworkDocument3 pagesTheoretical FrameworkAngelo Marcaida LLanes100% (2)
- How social environments influence business strategiesDocument10 pagesHow social environments influence business strategiesFara HameedNo ratings yet
- Encountered Challenges On Conducting Researches On Child and Adolescent DevelopmentDocument10 pagesEncountered Challenges On Conducting Researches On Child and Adolescent DevelopmentTrixy ManagoNo ratings yet
- Howmencommit PDFDocument13 pagesHowmencommit PDFRenata RaducanuNo ratings yet
- Story How To Build Self - EsteemDocument11 pagesStory How To Build Self - EsteemShailaja RaghavendraNo ratings yet
- Delaware Tech mental health nursing guideDocument9 pagesDelaware Tech mental health nursing guidernurse1177No ratings yet
- An Analysis On Non Verbal Communication and Barriers To Communication in The MovieDocument28 pagesAn Analysis On Non Verbal Communication and Barriers To Communication in The MovieRandhir SinghNo ratings yet
- Portfolio IntroDocument2 pagesPortfolio Introapi-296553705No ratings yet
- English 12TH CBSE ProjectDocument13 pagesEnglish 12TH CBSE ProjectKaran Patil100% (1)
- The Human Disease Project: Performance Task General Biology 2Document10 pagesThe Human Disease Project: Performance Task General Biology 2John MarkNo ratings yet
- Affect vs. EmotionDocument3 pagesAffect vs. EmotionyaujaNo ratings yet
- Theory of Chris Argyris: Models of Theories-In-UseDocument3 pagesTheory of Chris Argyris: Models of Theories-In-UsenavenNo ratings yet
- Daftar Pustaka: AMZAL MORTIN ANDAS, Dr. Christantie Effendy, S.KP., M.Kes, Dr. Sri Setiyarini, S.KP., M.KesDocument5 pagesDaftar Pustaka: AMZAL MORTIN ANDAS, Dr. Christantie Effendy, S.KP., M.Kes, Dr. Sri Setiyarini, S.KP., M.KesNindy T. ImonNo ratings yet
- Results Life Skills Self AwarenessDocument6 pagesResults Life Skills Self AwarenessRashmi NNo ratings yet
- Demonstration SpeechDocument11 pagesDemonstration SpeechDaimon MwendelaNo ratings yet
- EJ1304557Document16 pagesEJ1304557Cindy MonicaNo ratings yet
- Autism Spectrum Disorder Screening Machine Learning Adaptation and DSM 5 Fulfillment PDFDocument6 pagesAutism Spectrum Disorder Screening Machine Learning Adaptation and DSM 5 Fulfillment PDFBudi SantoNo ratings yet
- Understanding Consumer BehaviorDocument5 pagesUnderstanding Consumer BehaviorTMU Faculty Mr.Vibhor JainNo ratings yet
- The Objective Structured Clinical Examination (OSCE) : AMEE Guide No. 81. Part I: An Historical and Theoretical PerspectiveDocument11 pagesThe Objective Structured Clinical Examination (OSCE) : AMEE Guide No. 81. Part I: An Historical and Theoretical PerspectiveAnonymous wGAc8DYl3VNo ratings yet
- Lect 1 Cognitive PsyDocument15 pagesLect 1 Cognitive PsyMubarrah MubarrahNo ratings yet
- 2012 - Krueger Et Al - Initial Construction of A Maladaptive Personality TraitDocument12 pages2012 - Krueger Et Al - Initial Construction of A Maladaptive Personality TraitMaria Emilia WagnerNo ratings yet
- Ockelford Music AutismDocument274 pagesOckelford Music AutismChus VegaNo ratings yet
- Constructivist theory and teaching mathematics explainedDocument3 pagesConstructivist theory and teaching mathematics explainedJun VelascoNo ratings yet
- Color OracleDocument6 pagesColor Oraclewhatrich100% (1)
- Lazear Gibbs 2007Document157 pagesLazear Gibbs 2007Edith KuaNo ratings yet
- Hansen Et Al-2019-Family and Consumer Sciences Research JournalDocument16 pagesHansen Et Al-2019-Family and Consumer Sciences Research Journalapi-480572115No ratings yet
- Leadership TheoriesDocument10 pagesLeadership TheoriesMelNo ratings yet
- Alex FDocument8 pagesAlex FMohd Akmal Mohd DinNo ratings yet
- Classroom Instruction and Management PracticesDocument16 pagesClassroom Instruction and Management PracticesSiti Noor WahidaNo ratings yet
- Ethnographic Interviewing: Asking The Right Questions To The Right People in The Right WaysDocument8 pagesEthnographic Interviewing: Asking The Right Questions To The Right People in The Right Waystahir835No ratings yet