You might also like
- Exploring The Characteristics of Millennials in Online Buying BehaviorDocument9 pagesExploring The Characteristics of Millennials in Online Buying BehaviorSha RaNo ratings yet
- ELecture 1 - Overview of Phamaceutical IndustryDocument36 pagesELecture 1 - Overview of Phamaceutical IndustryJackson TeoNo ratings yet
- Telepharmacy ResearchDocument8 pagesTelepharmacy Researchugwuja marcyNo ratings yet
- Communication and Community Engagement in Disease Outbreaks: Erma Manoncourt Rafael Obregon Ketan Chitnis EditorsDocument224 pagesCommunication and Community Engagement in Disease Outbreaks: Erma Manoncourt Rafael Obregon Ketan Chitnis EditorsQfb Victor RobledoNo ratings yet
- Bias in ResearchDocument6 pagesBias in ResearchIrfan DanialNo ratings yet
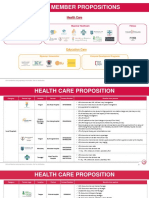
- Aia Member Propositions: Health CareDocument9 pagesAia Member Propositions: Health CareMin H. OONo ratings yet
- Psychosocial and practical experiences of students during COVID-19Document140 pagesPsychosocial and practical experiences of students during COVID-19Jeffrey Roy Adlawan LopezNo ratings yet
- The Impact of The Covid-19 Social and Physical Restrictive Measures On Cypriot Parents' and Children's' Well-BeingDocument19 pagesThe Impact of The Covid-19 Social and Physical Restrictive Measures On Cypriot Parents' and Children's' Well-BeingDemetris HadjicharalambousNo ratings yet
- Information 13 00330 v2 PDFDocument28 pagesInformation 13 00330 v2 PDFYasmine A. SabryNo ratings yet
- 8 207 - Group 1 - Research 1Document35 pages8 207 - Group 1 - Research 1april LomocsoNo ratings yet
- Guide For All ChaptersDocument39 pagesGuide For All ChaptersFrancesca PayawalNo ratings yet
- Big Data For Digital Healthcare Industry Challenges and Future PerspectivesDocument7 pagesBig Data For Digital Healthcare Industry Challenges and Future PerspectivesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Assignment 1 - Quantitative Research MethodsDocument15 pagesAssignment 1 - Quantitative Research MethodsAnushaPaulNo ratings yet
- Students' Income and Expenses StudyDocument10 pagesStudents' Income and Expenses StudyYashika DamodarNo ratings yet
- KLE Pharmacy - NPC Brochure 2022Document13 pagesKLE Pharmacy - NPC Brochure 2022Bhaskar PandeyNo ratings yet
- Disease Prediction Using Machine LearningDocument9 pagesDisease Prediction Using Machine LearningIJRASETPublicationsNo ratings yet
- Machine Learning On Adverse Drug Reactions For PharmacovigilanceDocument12 pagesMachine Learning On Adverse Drug Reactions For Pharmacovigilanceadarsh rajNo ratings yet
- The Impact of Pandemic Crisis On The Academic Competence and Mental Well (FINAL)Document26 pagesThe Impact of Pandemic Crisis On The Academic Competence and Mental Well (FINAL)Carl Joseph P. OlimpiadaNo ratings yet
- Scaleup Factors With An Industrial Perspectivescaleup Factors With An Industrial PerspectiveDocument14 pagesScaleup Factors With An Industrial Perspectivescaleup Factors With An Industrial PerspectiveItzel Melitce Martinez RomeroNo ratings yet
- I Pcs Activity Report 2018Document18 pagesI Pcs Activity Report 2018pooja chawanNo ratings yet
- Implementation of EMRs, NigeriaDocument17 pagesImplementation of EMRs, NigeriaAsmamaw K.No ratings yet
- Social Media Addiction Affects Students' Academic PerformanceDocument58 pagesSocial Media Addiction Affects Students' Academic PerformanceDianne Mae DagaNo ratings yet
- Screen MediaDocument9 pagesScreen MediaTere NavaNo ratings yet
- ResearchDocument10 pagesResearchBELARMINO LOUIE A.No ratings yet
- Gig Economy: Reshaping Strategic HRM in The Era of Industry 4.0 and Artificial IntelligenceDocument12 pagesGig Economy: Reshaping Strategic HRM in The Era of Industry 4.0 and Artificial IntelligenceSushmita TripathiNo ratings yet
- Childabuseandneglect: The Role of The Primary Care PediatricianDocument15 pagesChildabuseandneglect: The Role of The Primary Care PediatricianMilagros Saavedra RecharteNo ratings yet
- The Nursing Shortage and Its Effect On Patient CareDocument7 pagesThe Nursing Shortage and Its Effect On Patient Careapi-641842901No ratings yet
- Vaccination StrategiesDocument48 pagesVaccination StrategiesalinNo ratings yet
- Admin, 016 - 1038 - Putu Yoska Arya Harindana - Galley PDFDocument6 pagesAdmin, 016 - 1038 - Putu Yoska Arya Harindana - Galley PDFKhairan HusinNo ratings yet
- 7th Village Conference New BrochureDocument11 pages7th Village Conference New BrochureAtif JamalNo ratings yet
- Sedentary LifestyleDocument23 pagesSedentary LifestylePiona TheresNo ratings yet
- A Study On Using Queueing Theory To Reduce OPD Waiting Time in Hospital OperationsDocument5 pagesA Study On Using Queueing Theory To Reduce OPD Waiting Time in Hospital OperationsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Digital Health at WorldwebforumDocument28 pagesDigital Health at WorldwebforumCarolina SaleNo ratings yet
- Putanginang Research ToDocument9 pagesPutanginang Research ToAllen DomasingNo ratings yet
- Artificial Intelligence in Drug Discovery and DevelopmentDocument3 pagesArtificial Intelligence in Drug Discovery and DevelopmentKim KraliNo ratings yet
- Main Body of The Research PaperDocument82 pagesMain Body of The Research PaperJILLIAN JOY RUBYNo ratings yet
- Group 1 Research CassavaDocument15 pagesGroup 1 Research CassavaPresco ConsignaNo ratings yet
- Using E-Technologies in Clinical Trials Rosa 2015Document14 pagesUsing E-Technologies in Clinical Trials Rosa 2015Itzcoatl Torres AlcantaraNo ratings yet
- Role of Digital Therapeutics and The Changing Future of HealthcareDocument7 pagesRole of Digital Therapeutics and The Changing Future of HealthcareDavy DaveNo ratings yet
- Cross-Sectional Study On Knowledge, Attitude and Practice of Pharmacist at Community Pharmacy in Indonesia About COVID-19Document8 pagesCross-Sectional Study On Knowledge, Attitude and Practice of Pharmacist at Community Pharmacy in Indonesia About COVID-19International Journal of Innovative Science and Research TechnologyNo ratings yet
- A Productivity Assessment of PWD EmployeesDocument11 pagesA Productivity Assessment of PWD EmployeesSan TyNo ratings yet
- Evaluation of Feelings of Smart Phone Product Review Using SVM Technique of Sentiment AnalysisDocument14 pagesEvaluation of Feelings of Smart Phone Product Review Using SVM Technique of Sentiment AnalysisIJRASETPublicationsNo ratings yet
- Syllabus - OPIM 5894 Spring 2023Document5 pagesSyllabus - OPIM 5894 Spring 2023Noah LisleNo ratings yet
- Apollo Excellence Report 2019 e VersionDocument289 pagesApollo Excellence Report 2019 e VersionrajNo ratings yet
- Chapter 1 2 and 3Document10 pagesChapter 1 2 and 3Saysain UkayNo ratings yet
- Order 1359 (24-12-22)Document27 pagesOrder 1359 (24-12-22)khizra saeedNo ratings yet
- Review of Related Literature and StudiesDocument4 pagesReview of Related Literature and StudiesDante EcaranNo ratings yet
- G12 Final Research PaperDocument57 pagesG12 Final Research PaperIvanAlabaNo ratings yet
- CHapter 4 and 5 NalangDocument23 pagesCHapter 4 and 5 NalangAldricio MatiasNo ratings yet
- A Study On Water Resource Management and Its Issues in IndiaDocument4 pagesA Study On Water Resource Management and Its Issues in IndiaEditor IJTSRDNo ratings yet
- First Page ThesisDocument6 pagesFirst Page ThesisStanly AguilarNo ratings yet
- Research Proposal STEM1Document39 pagesResearch Proposal STEM1Jett Bernardo CortezNo ratings yet
- Big Data Healthcare Value-Based CareDocument18 pagesBig Data Healthcare Value-Based CareGEETHA RANI 218003946No ratings yet
- PreviewpdfDocument149 pagesPreviewpdfjoedesNo ratings yet
- Barangay Info System LiteratureDocument8 pagesBarangay Info System LiteratureAJNo ratings yet
- Supplementation of Feed Additives On Aquaculture Feeds: A ReviewDocument8 pagesSupplementation of Feed Additives On Aquaculture Feeds: A ReviewAndia BalabanNo ratings yet
- Students Readiness For The Face-To-Face Classes in Junior and Senior High SchoolDocument12 pagesStudents Readiness For The Face-To-Face Classes in Junior and Senior High SchoolIJAR JOURNALNo ratings yet
- Compensatory Growth and Feed Restriction in Marine Shrimp Production Using Biofloc TechnologyDocument10 pagesCompensatory Growth and Feed Restriction in Marine Shrimp Production Using Biofloc Technologyhighfive pologeeNo ratings yet
- Fake News Detection Using Python and Machine LearningDocument6 pagesFake News Detection Using Python and Machine Learningharini tNo ratings yet
- Advances 5Document15 pagesAdvances 5xdjpz44vyfNo ratings yet
- Artikel Frontier of Public HealthpdfDocument8 pagesArtikel Frontier of Public HealthpdfAnonymous EAPbx6No ratings yet
- The Impact of Pharmaceutical Cost Containment Policies On The Range of Medicines Available and Subsidized in Finland and New ZealandDocument9 pagesThe Impact of Pharmaceutical Cost Containment Policies On The Range of Medicines Available and Subsidized in Finland and New ZealandAnonymous EAPbx6No ratings yet
- S166 Osteonecrosis of The Jaw Associated With.166Document1 pageS166 Osteonecrosis of The Jaw Associated With.166Anonymous EAPbx6No ratings yet
- Health PromotionDocument14 pagesHealth PromotionAnonymous EAPbx6No ratings yet
- Morse 2001Document5 pagesMorse 2001Anonymous EAPbx6No ratings yet
- Drugs in Development For Hepatitis BDocument18 pagesDrugs in Development For Hepatitis BAnonymous EAPbx6No ratings yet
- Article - Pharmacists Knowledge On Complementary MedDocument12 pagesArticle - Pharmacists Knowledge On Complementary MedAnonymous EAPbx6No ratings yet
- Artikel Frontier of Public HealthpdfDocument8 pagesArtikel Frontier of Public HealthpdfAnonymous EAPbx6No ratings yet
- The Pros and Cons of Telepharmacy: A Canadian PerspectiveDocument29 pagesThe Pros and Cons of Telepharmacy: A Canadian PerspectiveAnonymous EAPbx6No ratings yet
- IJHPM - Volume 11 - Issue 10 - Pages 2198-2207Document10 pagesIJHPM - Volume 11 - Issue 10 - Pages 2198-2207Anonymous EAPbx6No ratings yet
- North Dakota Telepharmacy Project ModelDocument37 pagesNorth Dakota Telepharmacy Project ModelAnonymous EAPbx6No ratings yet
- Recommendations For The Treatment of Patients With Parkinson Disease During RamadanDocument5 pagesRecommendations For The Treatment of Patients With Parkinson Disease During RamadanAnonymous EAPbx6No ratings yet
- Protective Effect of Polygalae RadixDocument12 pagesProtective Effect of Polygalae RadixAnonymous EAPbx6No ratings yet
- FDA Finalizes Guidance For Hepatitis B Drug Development RAPSDocument3 pagesFDA Finalizes Guidance For Hepatitis B Drug Development RAPSAnonymous EAPbx6No ratings yet
- Acute Hepatitis Technical Briefing - 3Document35 pagesAcute Hepatitis Technical Briefing - 3Anonymous EAPbx6No ratings yet
- Efficacy and Safety of Herbal in InsomniaDocument23 pagesEfficacy and Safety of Herbal in InsomniaAnonymous EAPbx6No ratings yet
- Polygalae Radix A Review of Its Traditional UsesDocument46 pagesPolygalae Radix A Review of Its Traditional UsesAnonymous EAPbx6No ratings yet
- Evaluation of The Effectiveness and Tolerability of Glicazide During RamadanDocument10 pagesEvaluation of The Effectiveness and Tolerability of Glicazide During RamadanAnonymous EAPbx6No ratings yet
- New Roles Pharmacists: Value-Based Pay Creates OpportunitiesDocument33 pagesNew Roles Pharmacists: Value-Based Pay Creates OpportunitiesAnonymous EAPbx6No ratings yet
- Ramadan Fasting: Recommendations For Patients With Cardiovascular DiseaseDocument8 pagesRamadan Fasting: Recommendations For Patients With Cardiovascular DiseaseAnonymous EAPbx6No ratings yet
- Shahid Athar, MD, FACP, Face Author, "Islamic Perspective in Medicine" (ATP)Document25 pagesShahid Athar, MD, FACP, Face Author, "Islamic Perspective in Medicine" (ATP)She JocelynNo ratings yet
- Diabetes and RamadanDocument34 pagesDiabetes and RamadanAnonymous EAPbx6No ratings yet
- Ramadan Fasting May Benefit Musculoskeletal DiseasesDocument7 pagesRamadan Fasting May Benefit Musculoskeletal DiseasesAnonymous EAPbx6No ratings yet
- Recommendations For Management of Diabetes During Ramadan: Update 2010Document8 pagesRecommendations For Management of Diabetes During Ramadan: Update 2010Anonymous EAPbx6No ratings yet
- Diabetes and Ramadan guidelines for healthcare providersDocument53 pagesDiabetes and Ramadan guidelines for healthcare providersAnonymous EAPbx6No ratings yet
- Shahid Athar, MD, FACP, Face Author, "Islamic Perspective in Medicine" (ATP)Document25 pagesShahid Athar, MD, FACP, Face Author, "Islamic Perspective in Medicine" (ATP)She JocelynNo ratings yet
- Safety Assessment of A Proprietary Preparation of A Novel Probiotic, Bacillus Coagulans, As A Food IngredientDocument8 pagesSafety Assessment of A Proprietary Preparation of A Novel Probiotic, Bacillus Coagulans, As A Food IngredientAnonymous EAPbx6No ratings yet
- Medications Commonly Prescribed After A Stroke - GoodRxDocument11 pagesMedications Commonly Prescribed After A Stroke - GoodRxAnonymous EAPbx6No ratings yet
- Diabetes and Ramadan guidelines for healthcare providersDocument53 pagesDiabetes and Ramadan guidelines for healthcare providersAnonymous EAPbx6No ratings yet
- Introduction To The Practice of TelemedicineDocument8 pagesIntroduction To The Practice of TelemedicineRobbin BajpaiNo ratings yet
- Vision Ias Essay 2021Document91 pagesVision Ias Essay 2021M Shahid HusnainNo ratings yet
- Lakshita ReportDocument25 pagesLakshita Reportitsjusttwoofus1420No ratings yet
- Positive and Negative Impact of Technology in Medical FieldDocument4 pagesPositive and Negative Impact of Technology in Medical FieldMaxandrea Beatrice ArmillaNo ratings yet
- UNIT 1 Lecture 7 TelemedicineDocument33 pagesUNIT 1 Lecture 7 TelemedicineRithisha JaganNo ratings yet
- LABORATORY MANUAL (Ethics, Privacy and Security)Document7 pagesLABORATORY MANUAL (Ethics, Privacy and Security)Marichris CabanitNo ratings yet
- 7.1 TelemedicineDocument19 pages7.1 TelemedicineTrisha BawaNo ratings yet
- Arif Qureshi: University of UtahDocument1 pageArif Qureshi: University of UtahRuchi ShaikhNo ratings yet
- Nurs FPX 4900 Assessment 3 Assessing The Problem Technology Care Coordination and Community Resources ConsiderationsDocument6 pagesNurs FPX 4900 Assessment 3 Assessing The Problem Technology Care Coordination and Community Resources ConsiderationsEmma WatsonNo ratings yet
- Kristin Sohl - ECHO Autism: Bringing Best Autism Care To Primary CareDocument1 pageKristin Sohl - ECHO Autism: Bringing Best Autism Care To Primary CareAUCDNo ratings yet
- D1.1 Trends, Drivers, and Enablers of Digital HealthDocument34 pagesD1.1 Trends, Drivers, and Enablers of Digital HealthJohn MillerNo ratings yet
- University of San Francisco Student Health Insurance Plan For 2020 To 2021Document34 pagesUniversity of San Francisco Student Health Insurance Plan For 2020 To 2021The College FixNo ratings yet
- Maritime and Port Authority of Singapore Shipping Circular To Shipowners NO. 6 OF 2013Document13 pagesMaritime and Port Authority of Singapore Shipping Circular To Shipowners NO. 6 OF 2013gb singhNo ratings yet
- Coronavirus Frequently Asked QuestionsDocument67 pagesCoronavirus Frequently Asked Questionspearlygates12No ratings yet
- Impact of Covid-19 On Purchasing Patterns and Consumer BehaviorDocument4 pagesImpact of Covid-19 On Purchasing Patterns and Consumer BehaviorInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Individual and Family Plans Made SimpleDocument16 pagesIndividual and Family Plans Made SimpleShNo ratings yet
- Indian Healthcare Onthecuspofa Digital Transformation: WWW - Pwc.inDocument20 pagesIndian Healthcare Onthecuspofa Digital Transformation: WWW - Pwc.inswarnaNo ratings yet
- HealthTech IndiaDocument204 pagesHealthTech IndiaRohit Rsnwala75% (4)
- Digital DentistryDocument13 pagesDigital DentistryCesar Augusto Rojas MachucaNo ratings yet
- Full Report - Healthcare in The UAE and Saudi ArabiaDocument43 pagesFull Report - Healthcare in The UAE and Saudi ArabiaAlaa Ahmed100% (1)
- Healthcare & Medical Technologies - Singapore & Vietnam Selected European CompaniesDocument16 pagesHealthcare & Medical Technologies - Singapore & Vietnam Selected European CompaniesSalahNo ratings yet
- The Elements of Success:: 21 Customer Stories On Achieving Autonomous TransformationDocument34 pagesThe Elements of Success:: 21 Customer Stories On Achieving Autonomous TransformationValenNo ratings yet
- COVID-19 Federal Agency Actions & ResourcesDocument13 pagesCOVID-19 Federal Agency Actions & ResourcesSenator Rand PaulNo ratings yet
- Canadian Model Standards For TelepsychologyDocument3 pagesCanadian Model Standards For TelepsychologyJohn GavazziNo ratings yet
- The Ever-Evolving Landscape of Technology in Modern TimesDocument3 pagesThe Ever-Evolving Landscape of Technology in Modern TimesImran GhoriNo ratings yet
- 5G in IndiaDocument3 pages5G in IndiaSoham MukhopadhyayNo ratings yet
- Governor Economic Advisory Board Report 2020Document126 pagesGovernor Economic Advisory Board Report 2020A.W. CarrosNo ratings yet
- Marie Stopes International ReportDocument8 pagesMarie Stopes International ReportAustin DeneanNo ratings yet
- Establishing The Legal Framework of Telehealth in The PhilippinesDocument10 pagesEstablishing The Legal Framework of Telehealth in The Philippineshazell_aseronNo ratings yet
- OECD - Collective Action For Responsible AI in HealthDocument41 pagesOECD - Collective Action For Responsible AI in HealthAmaury Dudcoschi JuniorNo ratings yet