Volume 7, Issue 8, August – 2022 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
Health Outcome in India:
An Analysis of Multidimensional Inequality
Vini Sivanandan1; Vivekananda2
Abstract:- There are two significant sources of inequality Health inequality is the unjust differences in health
among individuals: one is circumstances, which is beyond between persons of different income and social groups and is
the control of an individual, and the other one is an effort attributed to disadvantages such as poverty, discrimination,
to an extent within the control of an individual. Roemer and lack of access to services and goods. Inequalities in health
(1998) emphasized equal opportunity wherein it describes are present in every society because certain parts and sections
that differences in circumstances are not a morally of the community are well accessible, whereas other sections
acceptable source of inequality. The paper attempts to or regions are deprived; however, in certain areas which
explore the multidimensional aspects of health. Further, might not have access to healthcare services but there might
this study intends to contribute to the quantitative be few individuals due to their socioeconomic status, who can
analysis of inequality by using dissimilarity indices access at par with their counterparts in areas with better
related to multinomial distributions by measuring and accessibility to health care. In contrast, an individual or group
comparing the extent of equality. Prominently older age with better access to health care but with lower
groups from 45-50 were highly represented in health socioeconomic status or a lack of awareness or self-inflicting
issues, and hypertension/heart disease, whereas in health damaging lifestyle may not effectively use the health system.
issues, injuries were predominantly represented by the This emphasises a holistic view of the health system.
age group 55-60 years of age. Health issues were most
prominently observed in rural areas compared to urban Numerous studies have examined the association
areas. The highest difference by population between background characteristics such as age, gender, and
representation between rural and urban areas was socioeconomic status to health. For example, inequalities in
observed in health issues, injuries and infection. health outcomes differ between gender and subgroups of the
population within males and females and by geographical
Keywords:- Age; Causes; Dissimilarity; Health; Inequality; areas, i.e. rural and urban areas Bora and Saikia (2015).
Multidimensional. Health inequality was more concentrated among the rich in
India for self-reported morbidity Jain et.al. (2012).
Takeaways:
Addressing policies toward the beneficiaries’ health Further, studies on multidimensional Inequality are
outcomes at a multidimensional level useful in identifying causes and solutions. For examining
Focused research to reach the most deprived. multidimensional Inequality, Fisher (1956) proposed a
A comprehensive index emphasizing concentration and multidimensional matrix. Additionally, one needs in-depth
exposure analysis to understand different individuals with different
health needs; hence just equal treatment to everyone may not
I. INTRODUCTION solve the problem as specific needs are not shared by all,
which again varies from individual to individual within a
There are two significant sources of Inequality among group. Overall, the concept of equity takes individual
individuals: one is circumstances, which is beyond the control circumstances in the context of health.
of an individual, and the other is an effort to an extent within
the control of an individual. The combination of both these Health equity requires removing obstacles to health such
factors plays a crucial role in determining the level of as poverty, discrimination, and indirect factors such as lack
Inequality. This leads to a situation wherein circumstances of access to services, decent jobs and jobs with high
dilute an individual’s effort or an individual effort overtakes occupation hazards, quality education, housing, safe
the events or vice versa. Thus, equal opportunity is a complex environments, and health care. Hence, health equity is
theory leading to Inequality, which leads to comparisons in achievable by reducing and ultimately eliminating health
indicating how different social systems and policies need to disparities and determinants that adversely affect excluded or
cope with disparities. marginalised groups.
Ray (1998) highlighted two main reasons for Inequality Individuals from different backgrounds, social groups,
first, an egalitarian society is desirable, especially if the initial and countries live with varying levels of health. The
conditions of the lives of individuals are crucial to their dimensions along which health inequalities are commonly
development, and second, inequality has functional impacts examined, between and within countries or states, by gender,
that can weaken the growth of a country. A policy aiming at education, caste, income, occupation, etc. Different theories
greater equity within the health system will lead to a decline attempt to explain group-level differences in health, including
in Inequality at the same time Espinoza (2007). psychosocial, material deprivation, health behavior,
IJISRT22AUG1032 www.ijisrt.com 1452
Volume 7, Issue 8, August – 2022 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
environmental, and selection explanations Arcaya et al. aspects of inequality, such as concentration and dissimilarity.
(2015). Considering these distinct dimensions of variation, health
inequality is inherently multidimensional. For more detailed
The complexity of multidimensional approaches when comparisons, a weighted index of systematic dissimilarity
the health determinants such as socioeconomic variables, was used due to the small sizes of some of the categories of
self-damaging individual lifestyles such as binge eating, poor groups.
hygiene, frequent exposure to harsh weather conditions,
exposure to the occupational hazard, access to health care etc. We use the data from the Social Consumption in India:
The varying level of health inequality arises when all these Health by the National Sample Survey Organization (NSSO)
determinants intersect to a varying degree leading to overall from their 75th round survey (2017- 18) to examine the
health inequalities. quantum of health inequality regarding demographic
characteristics. Social group, economic class as well as
Need for the Study geographic region.
Health inequality describes the differences, degree of The analysis is based on information collected through
variations, and disparities in the health achievements of NSS Schedule 25.0 (Household Social Consumption: Health)
individuals and groups but can be independent of any spread over the entire Indian Union, for which data were
assessment of their fairness Kawachi et al. (2002). The collected from 1,13,823 households (64,552 in rural areas and
approach to measuring health inequality varies from using the 49,271 in urban areas), covering 5,55,115 persons (3,25,883
classic study of the cross-national relationship between in rural areas and 2,29,232 in urban areas).
average national income and life expectancy Preston (1975)
to a quantitative measure approach to measure differentials in Methods
health across all units in a population. Theil index of dissimilarity was applied across
distributions to assess opportunity inequality in this paper.
A multidimensional approach to health inequality gives Theil statistic examines how equality of opportunity is
better insight into the well-being inequality within and achieved if the conditional distributions of
between populations. Socio-economic and demographic outcomes/advantages are equal across circumstance sets. All
characteristics shape health inequities in India. Socio- possible combinations of outcomes (e.g. health status with
economic demographic characteristics differentials leading to educational achievement, social group, etc.)
striking inequalities might exist due to the intersection of
various parameters. Theil statistic T is given by
The degree of inequality is measured mainly by Theil
n
Index, the concentration index Wagstaff, (1991), and the Gini 1 y p y
T * * ln p
coefficient to capture the multidimensional effect. The
multidimensional investigation leads to target public health n y
p 1 y
action, emphasising the need for greater investments in health
and related socio-economic variables, thereby strengthening Where n is the number of individuals in the population,
the effectiveness of health programs. This paper attempts to yp is the proportion of the population of the person indexed by
categories p, and y is the population’s average by
examine the degree of health inequalities across various
socio-economic parameters in India. The dissimilarity of
health outcomes identified by background characteristics will respective categories. If every individual has exactly the
help the policymakers target a focused group. Hence, the same value, T will be zero; thus represents perfect equality
paper attempts to explore the multidimensional aspects of and is the minimum value of Theil’s T. If it is represented in
health. Further, this study intends to contribute to the a particular category, T will equal ln n; this represents utmost
quantitative analysis of inequality by using dissimilarity inequality and is the maximum value of Theil’s T statistic.
indices related to multinomial distributions by measuring and
comparing the extent of equality. Further, we use the basic formula for the index of
dissimilarity given by Index of dissimilarity = ½*Abs(pi/Pi-
Objectives pj/Pj)
This study aims to identify the extent of
multidimensional inequalities across and within background where
characteristics of health outcomes. pi = the population of group i
Pi = the total population in group i for which the dissimilarity
II. DATA AND METHODS index is being calculated.
pji = the population of group j
Inequality does not originate from a single cause but Pj = the total population in group j for which the dissimilarity
from different socio and economic backgrounds resulting in index is calculated.
a complex process. We examine health outcomes in the
context of five background characteristics viz age, sex, The dissimilarity index is useful for input into
education, employment, caste, and marital status. The multidimensional analysis and is used to compare
expected multidimensional inequality can be in different distributions of different categories.
IJISRT22AUG1032 www.ijisrt.com 1453
Volume 7, Issue 8, August – 2022 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
For example, both in theil statistics the value yp and in characteristics. Whereas the value y is the average
the index of dissimilarity the value Pi and Pj is the proportion
of people who are identified by background characteristics, it proportion of weighted inequality people suffers at the same
shows the incidence of multidimensional background time. It shows the intensity of inequality of background
characteristics jointly with the incidence of illness.
III. RESULTS
Table 1: Index of Dissimilarity by Nature of Ailments and Background Characteristics in India
Ailments Age group Occupational Level of Marital Social Gender Religion
categories education Status Groups
Infection 0.200 0.186 0.030 0.214 0.037 0.025 0.030
Cancers 0.268 0.168 0.084 0.152 0.157 0.011 0.153
Blood Diseases 0.287 0.216 0.077 0.247 0.026 0.020 0.048
Endocrine 0.292 0.158 0.035 0.140 0.067 0.031 0.035
Psycho Neuro issues 0.096 0.104 0.060 0.031 0.038 0.068 0.022
Eye 0.358 0.113 0.149 0.168 0.057 0.028 0.080
Ear 0.248 0.192 0.159 0.174 0.119 0.059 0.109
Hypertension/Heart disease 0.289 0.132 0.036 0.162 0.086 0.064 0.040
Respiratory 0.238 0.164 0.131 0.087 0.062 0.059 0.056
Gastro Intestine 0.143 0.103 0.023 0.054 0.024 0.043 0.037
Skin disease 0.176 0.167 0.044 0.161 0.043 0.040 0.033
Muscular skeleton 0.206 0.122 0.055 0.131 0.032 0.022 0.038
Genito Urinary 0.143 0.119 0.077 0.121 0.039 0.028 0.038
Obstetric 0.646 0.455 0.047 0.212 0.112 - 0.070
Injuries 0.125 0.252 0.083 0.070 0.033 0.224 0.036
Other 0.088 0.065 0.042 0.030 0.058 0.022 0.017
Table 1 shows the index of dissimilarity between background characteristics. The dissimilarity index was highest and most
prominently among age groups and occupational categories. The estimates show that ailments due to obstetric causes are more
significant among age groups, occupational categories, and marital status than in any categories. This excess dissimilarity among
age groups and occupational categories is high among obstetric patients. In contrast, religion, level of education and social groups
do not explain much of the low dissimilarity values among different background characteristics.
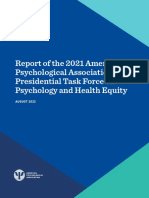
Fig 1: Theil inequality Decomposition by age groups in India
0.300
0.250
0.200
0.150
0.100
0.050
0.000
0 2 4 6 8 10 12 14 16 18
-0.050
-0.100
0 to 4 5 to 9 10 to 14 15 to 19 20 to 24 25 to 29 30 to 34
35 to 39 40 to 44 45 to 49 50 to 54 55 to 60 Theil
Theil index derived by age group and health issues shows the highest Theil value for health issues, hypertension/heart disease,
gastro intestine and injuries. In the case of hypertension/heart disease, the above-average representation was observed in older age
groups from age 45-49 onwards as reflected by the highest positive theil value compared to other lower age groups. Except for the
age group 35-39 to 45-49, all the different age groups show below-average health issues gastro intestine as reflected from their
IJISRT22AUG1032 www.ijisrt.com 1454
Volume 7, Issue 8, August – 2022 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
respective negative their values. Health issue injuries were predominantly represented by age group 55-60 which shows positive
theil value.
Fig 2: Theil inequality Decomposition by Social groups in India
0.140
0.120
0.100
0.080
0.060
0.040
0.020
0.000
-0.020
-0.040
STs SCs OBC Others Theil
Figure 2 shows the overall theil value was negative and derived for health issue infection by each social group. The theil value
derived is negative among social groups STs, SCs and others for health issue infection and positive among caste OBC. This implies
that caste OBCs have an above-average representation proportion of the population with health issue infection compared to other
social groups. Negative theil value was observed among caste STs for health issues Neurology, Heart disease, Respiratory, Muscular
skeleton, Genitourinary and injuries which implies below average representation. The highest total positive theil value was observed
for health issues, Heart disease, gastro intestine and injuries. While the highest proportion of heart disease was observed among
caste Others as reflected by positive theil value of caste others compared to other castes. Whereas caste OBC shows the highest
proportion with health issues, gastro intestine and injuries as reflected by highest positive theil values compared to different castes.
Fig 3: Theil inequality Decomposition by Marital status in India
0.200
0.150
0.100
0.050
0.000
-0.050
Never Married Currently Married Windowed Theil
The highest positive Theil value was observed in health issues, psycho neurology, heart disease, gastro intestine, muscular
skeleton, genitourinary and injuries by marital status currently married as observed in figure 3. The negative Theil value was
observed among never married in health issues heart disease and among widower in the health issues gastro intestine and injuries
which was reflected by their respective negative theil values.
IJISRT22AUG1032 www.ijisrt.com 1455
Volume 7, Issue 8, August – 2022 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
Fig 4: Theil inequality Decomposition by Religion in India
0.250
0.200
0.150
0.100
0.050
0.000
-0.050
Hindu Muslim Others Theil
As observed in figure 4, the highest Theil value was derived from health issues, injuries, Gastro urinary, Hypertension/Heart
disease, psycho Neuro, infection, and Genito intestine by religion. In the case of injuries and gastro urinary, the proportional
representation of religion others was comparatively lower for Hindus and Muslims as depicted by negative theil values. Whereas in
the case of health issues infection, there was above average representation of religion Others.
Fig 5: Theil inequality Decomposition by Education in India
0.100
0.080
0.060
0.040
0.020
0.000
-0.020
-0.040
-0.060
-0.080
-0.100
-0.120
Illitrate Primary l Middle Secondary Higher Theil
Figure 5 shows total Theil scores derived from education to be the least compared to other background characteristics. Infection
was the least among all the categories of education as reflected from respective negative theil value among all the types of education.
The below-average representation of health issue infection was observed in all the education categories, and the only above-average
representation was observed among illiterates. Below average proportion representation was observed in higher education with
health issues of hypertension/heart disease, gastro intestine and injuries as evident from their respective positive theil values.
IJISRT22AUG1032 www.ijisrt.com 1456
Volume 7, Issue 8, August – 2022 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
Fig 6: Theil inequality Decomposition by Occupation in India
0.100
0.050
0.000
-0.050
-0.100
-0.150
-0.200
-0.250
-0.300
Self Employed Unpaid Family worker Salaried
Casual Wage labour Unemploye Attended Educational institute
Domestic Duries Pensioners Others
Theil
Similarly, figure 6 shows below-average representation among all categories of occupation as represented by their respective
negative theil value thereby the overall theil value was negative predominantly for health issue infection. Occupation categories
such as Unpaid family workers and unemployed show below-average representation in health issues and psycho Neuro, as evident
from their respective negative Theil values. Above-average representation in the health issue Hypertension/heart disease was
observed among occupation categories of self-employed, domestic duties, pensioners and others. Overall the health issues among
the unemployed were negligible as compared to other types of occupation.
Fig 7: Theil inequality Decomposition by Region in India
0.200
0.180
0.160
0.140
0.120
0.100
0.080
0.060
0.040
0.020
0.000
Rural Urban Theil
Figure 7 shows the Theil value by region and the health IV. SUMMARY OF FINDINGS
issues observed most prominently among rural areas
compared to urban areas. The difference in the representation Prominently older age groups from 45-50 were highly
between rural and urban areas was the least for health issues represented in health issues, and hypertension/heart disease,
related to the ear. The highest difference was observed in whereas in health issues, injuries were predominantly
health issues, injuries and infection, with both the regions represented by the age group 55-60 years of age.
showing above-average representation but comparatively
more in rural areas.
IJISRT22AUG1032 www.ijisrt.com 1457
Volume 7, Issue 8, August – 2022 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
Caste STs show the least representation in health issues illiterates, Infection was the least among all the education
Neurology, Heart disease, Respiratory, muscular skeleton, categories. Below average proportion representation was
Genitourinary and injuries. The highest proportion of heart observed in higher education with health issues of
disease was observed among the caste Others, whereas caste hypertension/heart disease, gastro intestine and injuries.
OBC shows the highest proportion with health issues
infection, gastro intestine and injuries. Unpaid family workers and unemployed show below-
average representation in health issues, psycho Neuro, as
Health issues, psycho neurology, heart disease, gastro evident from their respective negative Theil scores. Above-
intestine, muscular skeleton, genitourinary and injuries were average representation in the health issue Hypertension/heart
predominantly observed among the currently married disease was observed among self-employed, domestic duties
population. In contrast, the least number of representation pensioners and others. Overall, the health issues among the
was observed among never married in health issues unemployed were negligible compared to other occupations.
hypertension/heart disease and among widower in health
issues gastro intestine and injuries. Health issues were most prominently observed in rural
areas compared to urban areas. The difference in the
In the case of health issues, injuries and gastro urinary, representation between rural and urban areas was the least for
the proportional representation of religion others were health issues related to the ear. The highest difference was
comparatively lower for Hindus and Muslims as depicted by observed in health issues, injuries and infection, with both the
the negative values of Theil. Whereas in case of health issues regions showing above-average representation but
infection, there was an above-average representation of comparatively more in rural areas.
religion, Hindu and below-average expression of religion
Muslim and others. Dissimilarity was higher among age groups, and
occupational categories.
Overall, theil value derived in education is the least
compared to other background characteristics. Except among
Table 2
Health Outcome Inequality Health Outcome Inequity
By Age Groups (older vs younger) Identifying predominant health issues by region, gender, social groups, genetics etc.
By Social Groups Identifying predominant health issues by access to health care, occupation-related issues
etc.
By Marital status Health issues with a focus on gender, lifestyle etc.
By Education Examining the access, awareness and right to health by level of education, employment
etc.
By Occupation Addressing occupation specific health issues
By region Examining access to health care
V. CONCLUSION REFERENCES
There are several policies targeted toward targeted [1]. Allison, R. A., & Foster, J. E. (2004). Measuring health
beneficiaries under different departments. Hence, addressing inequality using qualitative data. Journal of health
policies toward the beneficiary’s health outcomes at a economics, 23(3), 505-524.
multidimensional level may lead to a focused research and [2]. Arcaya, M. C., Arcaya, A. L., & Subramanian, S. V.
reach the most deprived. The results of this study point to (2015). Inequalities in health: definitions, concepts, and
further exploiting the dimensions of health outcomes at the theories. Global health action, 8(1), 27106.
micro-level by integrating different government health [3]. Atkinson, A., 1970. On the measurement of inequality.
schemes. A comprehensive index emphasizing concentration Journal of Economic Theory 2, 244-263.
and exposure is the need of the hour. [4]. Atkinson, A., Bourguignon, F., 1982. The comparison
of multi-dimensioned distributions of economic status.
Our health information system prioritizes collecting Review of Economic Studies 49, 183-201.
data on essential demographic and background characteristics [5]. Bleichrodt, H., & Van Doorslaer, E. (2006). A welfare
and the inherent biological determinants of health to prioritize economics foundation for health inequality
the overall factors responsible for overall health and well- measurement. Journal of Health Economics, 25(5), 945–
being. In addition, memerging data with other determinants 957.
such as education and employment outcome will highlight [6]. Bora, J K and N Saikia (2015). Gender Differentials in
how these other determinants contribute to health inequities. Self-rated Health and Self-reported Disability among
Adults in India. PLoS ONE, 10 (1).
IJISRT22AUG1032 www.ijisrt.com 1458
Volume 7, Issue 8, August – 2022 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
[7]. Braveman, P., & Gruskin, S. (2003). Defining equity in
health. Journal of Epidemiology & Community
Health, 57(4), 254-258.
[8]. Carter-Pokras, O., & Baquet, C. (2002). What is a"
health disparity"?. Public health reports, 117(5), 426.
[9]. Duncan, O. and Duncan B. (1955). A methodological
analysis of segregation indexes. American Sociological
Review 20, 210–17.
[10]. Espinoza, O. (2007). Solving the equity–equality
conceptual dilemma: A new model for analysis of the
educational process. Educational research, 49(4), 343-
363.
[11]. Fisher, F. M. (1956). Income Distribution, Value
Judgements and Welfare. Quarterly Journal of
Economics 70, 380-424.
[12]. Jain, K, S Goli and P Arokiasamy (2012). Are Self
Reported Morbidities Deceptive in Measuring
Socioeconomic Inequalities. Indian Journal of Medical
Research, 136 (5): 750-57.
[13]. Kawachi, I., Subramanian, S., & Almeida-Filho, N.
(2002). A glossary for health inequalities. Journal of
Epidemiology & Community Health, 56(9), 647–652.
[14]. Naga, R. H. A., & Yalcin, T. (2008). Inequality
measurement for ordered response health data. Journal
of Health Economics, 27(6), 1614-1625.
[15]. Pliskin, J. S., Shepard, D. S., & Weinstein, M. C. (1980).
Utility functions for life years and health status.
Operations Research, 28(1), 206–224.
[16]. Preston, S. H. (1975). The Changing Relation between
Mortality and Level of Economic Development. Population
Studies, 29(2), 231–248.
[17]. Ray, D. (1998). Development economics. Princeton
University Press.
[18]. Roemer, J (1998). Equality of Opportunity. Harvard
University Press
[19]. Wagstaff, A. (2002). Poverty and health sector
inequalities. Bulletin of the world health
organization, 80, 97-105.
[20]. Whitehead, M., & Dahlgren, G. (2006). Concepts and
principles for tackling social inequities in health:
Levelling up Part 1. World Health Organization: Studies
on social and economic determinants of population
health, 2, 460-474.
[21]. Whitehead, M. (1991). The concepts and principles of
equity and health. Health promotion international, 6(3),
217-228.
IJISRT22AUG1032 www.ijisrt.com 1459
You might also like
- How Not to Die: The Code to Your Amazing Life, Living Longer, Safer, and HealthierFrom EverandHow Not to Die: The Code to Your Amazing Life, Living Longer, Safer, and HealthierNo ratings yet
- Östlin - Paying Attention To GenderDocument6 pagesÖstlin - Paying Attention To GendermariaconstanzavasqueNo ratings yet
- Tackling Health Inequalities Through Policy, Practice and EvaluationDocument40 pagesTackling Health Inequalities Through Policy, Practice and EvaluationArianiNo ratings yet
- 17.321.2687 Ni Komang Sri WahyuniDocument19 pages17.321.2687 Ni Komang Sri Wahyunigekayu sartikaNo ratings yet
- Social Determinants of Health and Theories - EditedDocument5 pagesSocial Determinants of Health and Theories - EditedSamuel WachochoNo ratings yet
- Inequalities in Health Definitions Concepts and TheoriesDocument13 pagesInequalities in Health Definitions Concepts and TheoriesLoris Paola Romero CaballeroNo ratings yet
- Strengthening Health Information Systems To Address Health Equity ChallengesDocument16 pagesStrengthening Health Information Systems To Address Health Equity ChallengesAhlidin S.No ratings yet
- Socio-Economic Inequalities in Health and Health Service Use Among Older Adults in India - Results From The WHO Study On Global AGEing and Adult Health SurveyDocument10 pagesSocio-Economic Inequalities in Health and Health Service Use Among Older Adults in India - Results From The WHO Study On Global AGEing and Adult Health SurveyAnindita BalaganesanNo ratings yet
- Inequalities in Health Definitions Concepts and TheoriesDocument13 pagesInequalities in Health Definitions Concepts and TheoriesAlhassan MayeiNo ratings yet
- Braveman 2011 PDFDocument7 pagesBraveman 2011 PDFHenry KaweesaNo ratings yet
- Ebb PDFDocument12 pagesEbb PDFMonica TanNo ratings yet
- Global HealthDocument3 pagesGlobal HealthDinda ElahmadiNo ratings yet
- Maternal Health Inequity in IndiaDocument31 pagesMaternal Health Inequity in IndiakavalapparaNo ratings yet
- Inequity in India: The Case of Maternal and Reproductive HealthDocument31 pagesInequity in India: The Case of Maternal and Reproductive HealthPankaj PatilNo ratings yet
- Social Class & Health Status: EssayDocument6 pagesSocial Class & Health Status: EssayRavi Mana-ay EjarNo ratings yet
- Hiap PPT Module 2 Part 2Document23 pagesHiap PPT Module 2 Part 2Syed Hafizur RahmanNo ratings yet
- Report APA 2021 Psychology and Health EquityDocument13 pagesReport APA 2021 Psychology and Health EquityAldani PutriNo ratings yet
- Ijma 6 139Document26 pagesIjma 6 139amiraNo ratings yet
- Baidin2021 Article HowSelf RatedIsSelf RatedHealtDocument22 pagesBaidin2021 Article HowSelf RatedIsSelf RatedHealtGabriel MacielNo ratings yet
- 524-Book Chapter-5426-2-10-20220425Document10 pages524-Book Chapter-5426-2-10-20220425M ArztNo ratings yet
- Written Public Health Ll. U2Document7 pagesWritten Public Health Ll. U2Adanigbo MagretNo ratings yet
- NRSG 780 - Understanding Health DisparitiesDocument24 pagesNRSG 780 - Understanding Health DisparitiesjustdoyourNo ratings yet
- Health Equity LectureDocument41 pagesHealth Equity LectureKatie NolanNo ratings yet
- Jurnal B.inggrisDocument7 pagesJurnal B.inggrishellda putri arieskaNo ratings yet
- HCAD 620 Week 3's DiscussionDocument3 pagesHCAD 620 Week 3's Discussionkelvin oumaNo ratings yet
- Health_Disparities_and_Health_Education-1final (1) (1)Document13 pagesHealth_Disparities_and_Health_Education-1final (1) (1)brendahronoh254No ratings yet
- Health Equalities and InequalitiesDocument14 pagesHealth Equalities and InequalitiespatrickNo ratings yet
- Introduction to Community HealthDocument6 pagesIntroduction to Community HealthRodgers OmariNo ratings yet
- Utility and Limitations of Measures of Health Inequities A Theoretical PerspectiveDocument9 pagesUtility and Limitations of Measures of Health Inequities A Theoretical PerspectiveStephanyNo ratings yet
- Braveman, 2006 PDFDocument30 pagesBraveman, 2006 PDFAna GalliNo ratings yet
- HSH207 ThiThuyTrangLY AT1Document9 pagesHSH207 ThiThuyTrangLY AT1Huong NguyenNo ratings yet
- Ill-Health and Poverty A Literature Review On Health in Informal SettlementsDocument10 pagesIll-Health and Poverty A Literature Review On Health in Informal Settlementsc5m07hh9No ratings yet
- Structural Social Forces and Health Disparities Outline - EditedDocument9 pagesStructural Social Forces and Health Disparities Outline - EditedSammy DeeNo ratings yet
- Determinants of Health: DR Amir Akbar Shaikh Asst. Prof (Head of Department) Community DentistryDocument42 pagesDeterminants of Health: DR Amir Akbar Shaikh Asst. Prof (Head of Department) Community DentistryAriba AsifNo ratings yet
- Health Equity Sabtu16052020Document33 pagesHealth Equity Sabtu16052020m.adenfauzanNo ratings yet
- Geriatric NursingDocument8 pagesGeriatric NursingLmj75 ntNo ratings yet
- INTRODUCTION TO GLOBAL HEALTH LessonsDocument39 pagesINTRODUCTION TO GLOBAL HEALTH LessonsDeidra Borus100% (1)
- The Changing Demographic Profile of Eating Disorder Behaviors in The Community 2.23.16 PMDocument9 pagesThe Changing Demographic Profile of Eating Disorder Behaviors in The Community 2.23.16 PMShera LopezNo ratings yet
- H D H E:: Concepts and MeasurementDocument30 pagesH D H E:: Concepts and Measurementapi-217601938No ratings yet
- AJAN 25-2 Massey PDFDocument5 pagesAJAN 25-2 Massey PDFBOBNo ratings yet
- Nimhd Strategic Plan 2021 2025Document38 pagesNimhd Strategic Plan 2021 2025jeanbourgeatNo ratings yet
- 3 RepliesDocument4 pages3 Repliesezra oyaroNo ratings yet
- Marmot y Allen (2014)Document7 pagesMarmot y Allen (2014)Hospitales Federales de Referencia CCINSHAENo ratings yet
- Public Health Session 4Document19 pagesPublic Health Session 4J KNo ratings yet
- Comparing Well-Being Among Rural and Urban Indonesian Older People: A Quantitative Analysis of The Related FactorsDocument9 pagesComparing Well-Being Among Rural and Urban Indonesian Older People: A Quantitative Analysis of The Related FactorsIJPHSNo ratings yet
- Different Indicators of Socioeconomic Status and Their Relative Importance As Determinants of Health in Old AgeDocument11 pagesDifferent Indicators of Socioeconomic Status and Their Relative Importance As Determinants of Health in Old AgeWina BeziNo ratings yet
- ExclusionDocument6 pagesExclusionDr.Kirti PandeyNo ratings yet
- Group-2 11stem2202 Pt Readwrite-2Document15 pagesGroup-2 11stem2202 Pt Readwrite-2arnellejonellaNo ratings yet
- Inequalities Healthcare Dec2022Document40 pagesInequalities Healthcare Dec2022Morgan BaileyNo ratings yet
- Disability PAADocument18 pagesDisability PAAaaasNo ratings yet
- Understanding How Discrimination Can Affect HealthDocument15 pagesUnderstanding How Discrimination Can Affect HealthNna HsnNo ratings yet
- Review Health-Seeking BehaviorDocument11 pagesReview Health-Seeking BehaviorDadanMKNo ratings yet
- A Three-Stage Approach To Measuring Health Inequalities and InequitiesDocument13 pagesA Three-Stage Approach To Measuring Health Inequalities and Inequitiessean8phamNo ratings yet
- A Vital Direction For Health and Health Care: Addressing Social Determinants of Health and Health DisparitiesDocument16 pagesA Vital Direction For Health and Health Care: Addressing Social Determinants of Health and Health DisparitiesEgi NabilaNo ratings yet
- LC459 CW1 SOH (Jubair) (Feedback)Document10 pagesLC459 CW1 SOH (Jubair) (Feedback)Death StrokeNo ratings yet
- Equity of Access To Health Care: Theory & Aplication in ResearchDocument8 pagesEquity of Access To Health Care: Theory & Aplication in ResearchNoviana ZaraNo ratings yet
- Health Social WorkDocument21 pagesHealth Social WorkBekele MollaNo ratings yet
- Module 6 NRSG780Document14 pagesModule 6 NRSG780justdoyourNo ratings yet
- ADELE Hasimiyu Vol 9 2Document11 pagesADELE Hasimiyu Vol 9 2안성호No ratings yet
- Health Defined: Objectives For Promotion and PreventionDocument23 pagesHealth Defined: Objectives For Promotion and PreventionCoral Srinivasa RamaluNo ratings yet
- Visual Water: An Integration of App and Web to Understand Chemical ElementsDocument5 pagesVisual Water: An Integration of App and Web to Understand Chemical ElementsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Parastomal Hernia: A Case Report, Repaired by Modified Laparascopic Sugarbaker TechniqueDocument2 pagesParastomal Hernia: A Case Report, Repaired by Modified Laparascopic Sugarbaker TechniqueInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Smart Cities: Boosting Economic Growth through Innovation and EfficiencyDocument19 pagesSmart Cities: Boosting Economic Growth through Innovation and EfficiencyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Smart Health Care SystemDocument8 pagesSmart Health Care SystemInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Impact of Silver Nanoparticles Infused in Blood in a Stenosed Artery under the Effect of Magnetic Field Imp. of Silver Nano. Inf. in Blood in a Sten. Art. Under the Eff. of Mag. FieldDocument6 pagesImpact of Silver Nanoparticles Infused in Blood in a Stenosed Artery under the Effect of Magnetic Field Imp. of Silver Nano. Inf. in Blood in a Sten. Art. Under the Eff. of Mag. FieldInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Insights into Nipah Virus: A Review of Epidemiology, Pathogenesis, and Therapeutic AdvancesDocument8 pagesInsights into Nipah Virus: A Review of Epidemiology, Pathogenesis, and Therapeutic AdvancesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- An Analysis on Mental Health Issues among IndividualsDocument6 pagesAn Analysis on Mental Health Issues among IndividualsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Implications of Adnexal Invasions in Primary Extramammary Paget’s Disease: A Systematic ReviewDocument6 pagesImplications of Adnexal Invasions in Primary Extramammary Paget’s Disease: A Systematic ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Compact and Wearable Ventilator System for Enhanced Patient CareDocument4 pagesCompact and Wearable Ventilator System for Enhanced Patient CareInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Relationship between Teacher Reflective Practice and Students Engagement in the Public Elementary SchoolDocument31 pagesThe Relationship between Teacher Reflective Practice and Students Engagement in the Public Elementary SchoolInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Air Quality Index Prediction using Bi-LSTMDocument8 pagesAir Quality Index Prediction using Bi-LSTMInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Predict the Heart Attack Possibilities Using Machine LearningDocument2 pagesPredict the Heart Attack Possibilities Using Machine LearningInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Utilization of Date Palm (Phoenix dactylifera) Leaf Fiber as a Main Component in Making an Improvised Water FilterDocument11 pagesThe Utilization of Date Palm (Phoenix dactylifera) Leaf Fiber as a Main Component in Making an Improvised Water FilterInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Parkinson’s Detection Using Voice Features and Spiral DrawingsDocument5 pagesParkinson’s Detection Using Voice Features and Spiral DrawingsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Investigating Factors Influencing Employee Absenteeism: A Case Study of Secondary Schools in MuscatDocument16 pagesInvestigating Factors Influencing Employee Absenteeism: A Case Study of Secondary Schools in MuscatInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Harnessing Open Innovation for Translating Global Languages into Indian LanuagesDocument7 pagesHarnessing Open Innovation for Translating Global Languages into Indian LanuagesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Exploring the Molecular Docking Interactions between the Polyherbal Formulation Ibadhychooranam and Human Aldose Reductase Enzyme as a Novel Approach for Investigating its Potential Efficacy in Management of CataractDocument7 pagesExploring the Molecular Docking Interactions between the Polyherbal Formulation Ibadhychooranam and Human Aldose Reductase Enzyme as a Novel Approach for Investigating its Potential Efficacy in Management of CataractInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Terracing as an Old-Style Scheme of Soil Water Preservation in Djingliya-Mandara Mountains- CameroonDocument14 pagesTerracing as an Old-Style Scheme of Soil Water Preservation in Djingliya-Mandara Mountains- CameroonInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Diabetic Retinopathy Stage Detection Using CNN and Inception V3Document9 pagesDiabetic Retinopathy Stage Detection Using CNN and Inception V3International Journal of Innovative Science and Research TechnologyNo ratings yet
- Dense Wavelength Division Multiplexing (DWDM) in IT Networks: A Leap Beyond Synchronous Digital Hierarchy (SDH)Document2 pagesDense Wavelength Division Multiplexing (DWDM) in IT Networks: A Leap Beyond Synchronous Digital Hierarchy (SDH)International Journal of Innovative Science and Research TechnologyNo ratings yet
- The Making of Object Recognition Eyeglasses for the Visually Impaired using Image AIDocument6 pagesThe Making of Object Recognition Eyeglasses for the Visually Impaired using Image AIInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Electro-Optics Properties of Intact Cocoa Beans based on Near Infrared TechnologyDocument7 pagesElectro-Optics Properties of Intact Cocoa Beans based on Near Infrared TechnologyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Advancing Healthcare Predictions: Harnessing Machine Learning for Accurate Health Index PrognosisDocument8 pagesAdvancing Healthcare Predictions: Harnessing Machine Learning for Accurate Health Index PrognosisInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Design, Development and Evaluation of Methi-Shikakai Herbal ShampooDocument8 pagesDesign, Development and Evaluation of Methi-Shikakai Herbal ShampooInternational Journal of Innovative Science and Research Technology100% (3)
- Formulation and Evaluation of Poly Herbal Body ScrubDocument6 pagesFormulation and Evaluation of Poly Herbal Body ScrubInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Impact of Digital Marketing Dimensions on Customer SatisfactionDocument6 pagesThe Impact of Digital Marketing Dimensions on Customer SatisfactionInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- A Survey of the Plastic Waste used in Paving BlocksDocument4 pagesA Survey of the Plastic Waste used in Paving BlocksInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Comparatively Design and Analyze Elevated Rectangular Water Reservoir with and without Bracing for Different Stagging HeightDocument4 pagesComparatively Design and Analyze Elevated Rectangular Water Reservoir with and without Bracing for Different Stagging HeightInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Auto Encoder Driven Hybrid Pipelines for Image Deblurring using NAFNETDocument6 pagesAuto Encoder Driven Hybrid Pipelines for Image Deblurring using NAFNETInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Cyberbullying: Legal and Ethical Implications, Challenges and Opportunities for Policy DevelopmentDocument7 pagesCyberbullying: Legal and Ethical Implications, Challenges and Opportunities for Policy DevelopmentInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Mestrado Hang GlidingDocument82 pagesMestrado Hang GlidingJuliana Silveira100% (2)
- ANU Issue 2Document64 pagesANU Issue 2Gideon GreigNo ratings yet
- LGR Finite Ch5Document42 pagesLGR Finite Ch5FrancoSuperNo ratings yet
- Trading Rules Strategies William F EngDocument290 pagesTrading Rules Strategies William F EngDheeraj Suntha100% (10)
- AssignmentDocument34 pagesAssignmentAnshika SharmaNo ratings yet
- Mainf 517-527Document11 pagesMainf 517-527Upeksha PereraNo ratings yet
- How Computer Viruses Work and How to Prevent InfectionDocument4 pagesHow Computer Viruses Work and How to Prevent InfectionVishal guptaNo ratings yet
- Student Report Card ManagementDocument38 pagesStudent Report Card ManagementKannan Thangaraju41% (17)
- KUBOTA MU5501 4WD Tractor - T-1037-1562-2016Document9 pagesKUBOTA MU5501 4WD Tractor - T-1037-1562-2016Prashant PatilNo ratings yet
- CUMINDocument17 pagesCUMIN19BFT Food TechnologyNo ratings yet
- The Making of BuckshotDocument13 pagesThe Making of BuckshotDominicNo ratings yet
- Nanosafety Exam QuestionsDocument4 pagesNanosafety Exam QuestionsMulugetaNo ratings yet
- Airworthiness StandardsDocument15 pagesAirworthiness StandardsJason RossNo ratings yet
- Insulation Coordination in Power System - Electrical4UDocument13 pagesInsulation Coordination in Power System - Electrical4UR.SivachandranNo ratings yet
- BBP PreceduresDocument6 pagesBBP PreceduresSachin SinghNo ratings yet
- Shading DevicesDocument4 pagesShading DevicesAyush TyagiNo ratings yet
- Partial Molar PropertiesDocument6 pagesPartial Molar PropertiesNISHTHA PANDEYNo ratings yet
- Upper Limb OrthosisDocument47 pagesUpper Limb OrthosisPraneethaNo ratings yet
- Sources of FundsDocument22 pagesSources of FundsImtiaz RashidNo ratings yet
- Critical Factors Influencing Infrastructure ProvisionDocument6 pagesCritical Factors Influencing Infrastructure Provisionlulut falaNo ratings yet
- Y-16-30 WOF Maintenance ManualDocument158 pagesY-16-30 WOF Maintenance ManualSeth Barbour100% (1)
- Lesson 2.1Document16 pagesLesson 2.1Jeremie Manimbao OrdinarioNo ratings yet
- Lesson 5Document16 pagesLesson 5DANANo ratings yet
- Creating and Using Virtual DPUsDocument20 pagesCreating and Using Virtual DPUsDeepak Gupta100% (1)
- NRSG 5800 SyllabusDocument5 pagesNRSG 5800 Syllabusapi-310557802No ratings yet
- Inorganic Polymers: Classification and PropertiesDocument46 pagesInorganic Polymers: Classification and PropertiesGokul KannanNo ratings yet
- Behaviour of Rectangular Travelling Wave (Unit Step Function at Transition Points-Typical CasesDocument1 pageBehaviour of Rectangular Travelling Wave (Unit Step Function at Transition Points-Typical CasesAngela VaughnNo ratings yet
- KETRACO Clarifies Technical Queries for 400kV Transmission ProjectDocument5 pagesKETRACO Clarifies Technical Queries for 400kV Transmission Projectahmadove1No ratings yet
- Library ClassificationDocument10 pagesLibrary ClassificationKakeembo NasiifuNo ratings yet
- Codex AlexandrinusDocument294 pagesCodex AlexandrinusHevel Cava100% (2)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (17)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Summary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedRating: 4 out of 5 stars4/5 (11)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisFrom EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisRating: 5 out of 5 stars5/5 (8)
- 12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosFrom Everand12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosRating: 4.5 out of 5 stars4.5/5 (207)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)