You might also like
- NIH Public Access: Author ManuscriptDocument13 pagesNIH Public Access: Author ManuscriptCarolina LilloNo ratings yet
- Spsi 622 Page Quattlebaum-Severecommunicationdisorders W Ecolog Inventory ExDocument25 pagesSpsi 622 Page Quattlebaum-Severecommunicationdisorders W Ecolog Inventory Exapi-270949898No ratings yet
- Module 11 Augmentative and Alternative CommunicationDocument2 pagesModule 11 Augmentative and Alternative CommunicationJaja DavidNo ratings yet
- 2022 Butt AAC RSDocument5 pages2022 Butt AAC RSAndrea MedinaNo ratings yet
- AAC Technologies For Young Children PDFDocument18 pagesAAC Technologies For Young Children PDFDayna DamianiNo ratings yet
- RautakoskiDocument3 pagesRautakoskiyashomathiNo ratings yet
- AAC Alternative and Augmentative CommunicationDocument7 pagesAAC Alternative and Augmentative CommunicationDeepika GovindarajanNo ratings yet
- Aac - Assessment and Decision MakingDocument28 pagesAac - Assessment and Decision MakingRudran SubramanianNo ratings yet
- Augmentative - Alternative CommunicationDocument6 pagesAugmentative - Alternative CommunicationDenisse Paz Hurtado BravoNo ratings yet
- Drager Organizacion PanelesDocument16 pagesDrager Organizacion PanelesCristian GvNo ratings yet
- CTT tp2Document3 pagesCTT tp2wulanNo ratings yet
- BF TitleDocument26 pagesBF TitleIsha JainNo ratings yet
- The Picture Exchange Communication System-SummaryDocument3 pagesThe Picture Exchange Communication System-SummarySheela Marasigan PagkalinawanNo ratings yet
- The Use of Augmentative and Alternative Communication Methods With Infants and Toddlers With Disabilities: A Research ReviewDocument13 pagesThe Use of Augmentative and Alternative Communication Methods With Infants and Toddlers With Disabilities: A Research ReviewCOS ADRIANANo ratings yet
- Lecture 1 - Intro of AACDocument19 pagesLecture 1 - Intro of AACraniaNo ratings yet
- Chapter 3 - Assistive Technology For CommunicationDocument64 pagesChapter 3 - Assistive Technology For CommunicationOLASIMAN, SHAN ANGELNo ratings yet
- Supporting Social Competence in Children Who Use AacDocument9 pagesSupporting Social Competence in Children Who Use Aacapi-249986210100% (1)
- Antecedente - Efecto Del Modelo Del LenguajeDocument15 pagesAntecedente - Efecto Del Modelo Del LenguajeVanessa Llantoy ParraNo ratings yet
- Educ 3 - Chapter 3.3 - Trends and IssuesDocument11 pagesEduc 3 - Chapter 3.3 - Trends and IssuesMYLE MANAYONNo ratings yet
- HEALTH EDUCATION Rev.Document5 pagesHEALTH EDUCATION Rev.Northwestern Training Center IncNo ratings yet
- Speak App A Development of Mobile ApplicationDocument6 pagesSpeak App A Development of Mobile ApplicationWemerson MonteiroNo ratings yet
- 2017 Longitudinal Development of Communication in Children With Cerebral Palsy Between 24 and 53 Months - Predicting Speech OutcomesDocument17 pages2017 Longitudinal Development of Communication in Children With Cerebral Palsy Between 24 and 53 Months - Predicting Speech OutcomesJulian Caro MorenoNo ratings yet
- Overcoming Communication Barriers: Working With Patients With Intellectual DisabilitiesDocument5 pagesOvercoming Communication Barriers: Working With Patients With Intellectual DisabilitiesYuFan TanNo ratings yet
- Autism PDFDocument4 pagesAutism PDFViji ThulasiramanNo ratings yet
- Sentence Construction in SCAADocument13 pagesSentence Construction in SCAAmariaNo ratings yet
- Navigating Terminology and Promoting Evidence-Based Practice For Child Language Disorders: Challenges and Solutions For EducatorsDocument7 pagesNavigating Terminology and Promoting Evidence-Based Practice For Child Language Disorders: Challenges and Solutions For EducatorsIsraa AlmuzainiNo ratings yet
- AAC and Autism: Compelling Issues, Promising Practices and Future DirectionsDocument4 pagesAAC and Autism: Compelling Issues, Promising Practices and Future DirectionsvcuadrosvNo ratings yet
- Using Augmentative Communication With Infants and Young Children With Down SyndromeDocument0 pagesUsing Augmentative Communication With Infants and Young Children With Down SyndromeDini KohandiNo ratings yet
- Lasker, Garret, Fox (2007)Document9 pagesLasker, Garret, Fox (2007)Lorenzo Nifto AmmàrNo ratings yet
- ACN Pat Prov PDFDocument16 pagesACN Pat Prov PDFnersitiulfahNo ratings yet
- Communicating With People Who Use Augmentative and Alternative Communication (AAC)Document4 pagesCommunicating With People Who Use Augmentative and Alternative Communication (AAC)Charlie HaddadNo ratings yet
- Augmentative and Alternative Communication: Characteristics ChartDocument13 pagesAugmentative and Alternative Communication: Characteristics ChartMatias A. Rodriguez CherokyNo ratings yet
- AAC Tech For Young Children With MultidisabilityDocument14 pagesAAC Tech For Young Children With Multidisabilityapi-26018051No ratings yet
- Assistive Technology Devices For AutismDocument11 pagesAssistive Technology Devices For AutismAutism Parenting100% (1)
- Other Ways of Speaking FinalDocument52 pagesOther Ways of Speaking FinalMatías ArgüelloNo ratings yet
- Bishop 2001 PatDocument10 pagesBishop 2001 PatcynthiaNo ratings yet
- Study ScheduleDocument15 pagesStudy ScheduleJericho Martin FrancoNo ratings yet
- Using SymbolsDocument12 pagesUsing SymbolsParena Jane MelisseNo ratings yet
- Augmentative and Alternative Communication For Individuals With Autism Spectrum Disorder and Intellectual DisabilityDocument7 pagesAugmentative and Alternative Communication For Individuals With Autism Spectrum Disorder and Intellectual Disabilityvotetreasure05hwanNo ratings yet
- Picture Exchange Communication SystemDocument42 pagesPicture Exchange Communication SystemCelani TrajanoNo ratings yet
- 23 - Linguagem e PECS - InglDocument12 pages23 - Linguagem e PECS - InglPatricia ZuanettiNo ratings yet
- The Use of Augmentative and Alternative Communication As A Resource For The Children Literature Books InterpretationDocument8 pagesThe Use of Augmentative and Alternative Communication As A Resource For The Children Literature Books Interpretationfabianounesp2No ratings yet
- Clinical Effectiveness of AAC Intervention in Minimally Verbal Children With ASD: A Systematic ReviewDocument14 pagesClinical Effectiveness of AAC Intervention in Minimally Verbal Children With ASD: A Systematic ReviewGwyneth PañaNo ratings yet
- Childhood Apraxia of Speech 02Document4 pagesChildhood Apraxia of Speech 02Fono Amanda RoseNo ratings yet
- La Disposición Juiciosa de Los Símbolos en Una Pantalla de Comunicación Aumentativa y Alternativa Simulada Optimiza La Atención Visual de Las Personas Con Síndrome de DownDocument17 pagesLa Disposición Juiciosa de Los Símbolos en Una Pantalla de Comunicación Aumentativa y Alternativa Simulada Optimiza La Atención Visual de Las Personas Con Síndrome de DownValentina HurtadoNo ratings yet
- AAC Supports For Engaging Students With Autism Spectrum Disorders (ASD) in Group InstructionDocument6 pagesAAC Supports For Engaging Students With Autism Spectrum Disorders (ASD) in Group InstructionOrnella ThysNo ratings yet
- Supporting Secondary School Students With Language ImpairmentDocument6 pagesSupporting Secondary School Students With Language ImpairmentGabriela Mosqueda CisternaNo ratings yet
- Article 2 ReviewDocument5 pagesArticle 2 ReviewNora HynesNo ratings yet
- ASD and Funcional LangageDocument26 pagesASD and Funcional Langageflower21No ratings yet
- When Will He Talk? An Evidence-Based Tutorial For Measuring Progress Toward Use of Spoken Words in Preverbal Children With Autism Spectrum DisorderDocument18 pagesWhen Will He Talk? An Evidence-Based Tutorial For Measuring Progress Toward Use of Spoken Words in Preverbal Children With Autism Spectrum DisorderPaulina Guerra Santa MaríaNo ratings yet
- SC01 Lasker JoanneDocument27 pagesSC01 Lasker JoanneMichael MerlinNo ratings yet
- WK 2Document4 pagesWK 2api-377141164No ratings yet
- Behavior Modification: The Picture Exchange Communication SystemDocument21 pagesBehavior Modification: The Picture Exchange Communication SystemIulia StoianNo ratings yet
- PECS Info BrochureDocument5 pagesPECS Info BrochureJaqueline RosalNo ratings yet
- Autism-Strategies For CommunicationDocument21 pagesAutism-Strategies For CommunicationMs.Aishwarya Nallamuthu, Dept. of SLHS, SRIHERNo ratings yet
- Communication Function Classification System (CFCS) For Individuals With Cerebral PalsyDocument4 pagesCommunication Function Classification System (CFCS) For Individuals With Cerebral PalsyNoerwanty Yustitiana RidwanNo ratings yet
- Manual AAC For Caregivers 2019Document21 pagesManual AAC For Caregivers 2019Anda100% (1)
- Journal of Communication Disorders: SciencedirectDocument14 pagesJournal of Communication Disorders: SciencedirectGrethell UrcielNo ratings yet
- Technology and Therapy - The Use of ACC Devices - Regis College OnlineDocument7 pagesTechnology and Therapy - The Use of ACC Devices - Regis College Onlineashenafi.aNo ratings yet
- Angelman Syndrome: Communication, Educational, and Related ConsiderationsFrom EverandAngelman Syndrome: Communication, Educational, and Related ConsiderationsNo ratings yet
- Jaafar Et Al-2016-The Cochrane Library - Sup-1Document3 pagesJaafar Et Al-2016-The Cochrane Library - Sup-1Kiki PuchiNo ratings yet
- Interventions For The Cessation of Non-Nutritive Sucking Habits in ChildrenDocument46 pagesInterventions For The Cessation of Non-Nutritive Sucking Habits in ChildrenKiki PuchiNo ratings yet
- Integrating Speech-Language Pathology Services in Palliative End-of-Life CareDocument12 pagesIntegrating Speech-Language Pathology Services in Palliative End-of-Life CareKiki PuchiNo ratings yet
- Building Capacity in AAC A Person Centred Approach To Supporting Participation by People With Complex Communication NeedsDocument14 pagesBuilding Capacity in AAC A Person Centred Approach To Supporting Participation by People With Complex Communication NeedsKiki PuchiNo ratings yet
- 2020 A New Simple Screening Tool-4QTDocument11 pages2020 A New Simple Screening Tool-4QTKiki PuchiNo ratings yet
- Effect of A Thin Neck Pacifier On Primary Dentition RCTDocument10 pagesEffect of A Thin Neck Pacifier On Primary Dentition RCTKiki PuchiNo ratings yet
- A Preliminary Comparison of ReadingDocument8 pagesA Preliminary Comparison of ReadingKiki PuchiNo ratings yet
- AAC Efficacy Research Challenges For The NewDocument2 pagesAAC Efficacy Research Challenges For The NewKiki PuchiNo ratings yet
- Aac Position-Paper enDocument12 pagesAac Position-Paper enKiki PuchiNo ratings yet
- A Child Needs To Be Given A Chance To Succeed Parents of Individuals Who Use AAC Describe The Benefits and Challenges of Learning AAC TechnologiesDocument14 pagesA Child Needs To Be Given A Chance To Succeed Parents of Individuals Who Use AAC Describe The Benefits and Challenges of Learning AAC TechnologiesKiki PuchiNo ratings yet
- 2015 P EAT 10 DeglutiçãoDocument10 pages2015 P EAT 10 DeglutiçãoKiki PuchiNo ratings yet
- AAC and LiteracyDocument10 pagesAAC and LiteracyKiki PuchiNo ratings yet
- Fatores Risco PEG 2018Document10 pagesFatores Risco PEG 2018Kiki PuchiNo ratings yet
- 1 s2.0 S0003999313002864 MainDocument8 pages1 s2.0 S0003999313002864 MainKiki PuchiNo ratings yet
- 2005-Voice in SmokersDocument7 pages2005-Voice in SmokersKiki PuchiNo ratings yet
- 1 s2.0 S1751722212000455 MainDocument4 pages1 s2.0 S1751722212000455 MainKiki PuchiNo ratings yet
- (2006) An Internet-Based Telerehabilitation System For The Assessment of Motor Speech Disorders - A Pilot StudyDocument13 pages(2006) An Internet-Based Telerehabilitation System For The Assessment of Motor Speech Disorders - A Pilot StudyKiki PuchiNo ratings yet
- 5 Point Scale PowerpointDocument40 pages5 Point Scale PowerpointMíchílín Ní Threasaigh100% (1)
- Cranial Nerves - Function and Dysfunctions, 3E (2010) (PDF) (UnitedVRG)Document262 pagesCranial Nerves - Function and Dysfunctions, 3E (2010) (PDF) (UnitedVRG)Alvaro RivCalle87% (15)
- O.B Assignement MBA - May 2019 - Case Study v35Document4 pagesO.B Assignement MBA - May 2019 - Case Study v35ahmedNo ratings yet
- Free English TextbooksDocument110 pagesFree English TextbooksLolapNo ratings yet
- Feist Theories of Personality Chapter 1Document2 pagesFeist Theories of Personality Chapter 1Rashia LubuguinNo ratings yet
- Vika-Glick Larsen Johnson Branstiter 2005Document7 pagesVika-Glick Larsen Johnson Branstiter 2005kharaldsdottirNo ratings yet
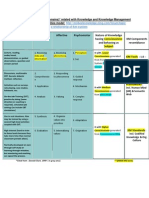
- Bloom's Taxonomy (Learning Domains) Related With Knowledge and Knowledge Management (KM)Document1 pageBloom's Taxonomy (Learning Domains) Related With Knowledge and Knowledge Management (KM)Md SantoNo ratings yet
- Imagenes Psicologia FisiologicaDocument18 pagesImagenes Psicologia FisiologicaMayra VillegasNo ratings yet
- Brezan Stukovnik Vodusek - NFB, EEG CORRELATES OF HYPNOSIS, ROGLA CONGRESS ON PSYCHOTHERAPY AND NEUROSCIENCEDocument2 pagesBrezan Stukovnik Vodusek - NFB, EEG CORRELATES OF HYPNOSIS, ROGLA CONGRESS ON PSYCHOTHERAPY AND NEUROSCIENCEsimon brežanNo ratings yet
- Strategy Strand Focus Content Standard Learning Standard Integrated Learning Standard Objective Activities Materials ReflectionDocument4 pagesStrategy Strand Focus Content Standard Learning Standard Integrated Learning Standard Objective Activities Materials ReflectionJunior JR JNo ratings yet
- An Investigation Into Student Teachers' Emotional Intelligence of Teaching Training Program: A Case Study at Loikaw..Document16 pagesAn Investigation Into Student Teachers' Emotional Intelligence of Teaching Training Program: A Case Study at Loikaw..Shreesh PatilNo ratings yet
- Behavioural Aspects of Language Attitude Mean DescriptionDocument6 pagesBehavioural Aspects of Language Attitude Mean Descriptionjhehan galmanNo ratings yet
- Geriatric AssessmentDocument28 pagesGeriatric AssessmentSanjanaa ZadNo ratings yet
- Practice Test Questions Downloaded From FILIPINO NURSES CENTRALDocument17 pagesPractice Test Questions Downloaded From FILIPINO NURSES CENTRALFilipino Nurses CentralNo ratings yet
- The Quest For A Quantum Neural NetworkDocument21 pagesThe Quest For A Quantum Neural NetworkKristóf GalambosNo ratings yet
- Hassan Elwan NeuroDocument181 pagesHassan Elwan Neuroaymanose914No ratings yet
- ABPD2103 PersonalityDocument10 pagesABPD2103 PersonalityRADHWANo ratings yet
- How Does Client Expressed Emotional Arousal Relate To Outcome in Experiential Therapy For Depression?Document19 pagesHow Does Client Expressed Emotional Arousal Relate To Outcome in Experiential Therapy For Depression?JeanYanNo ratings yet
- Communicative FunctionsmeansDocument4 pagesCommunicative FunctionsmeansmedotoNo ratings yet
- Central Coherence in Adults With A High-Functioning Autism Spectrum Disorder. in A Search For A Non-Self-Reporting Screening ToolDocument8 pagesCentral Coherence in Adults With A High-Functioning Autism Spectrum Disorder. in A Search For A Non-Self-Reporting Screening ToolNp Luis Gómez0% (1)
- Chapter 3 Lesson 2Document6 pagesChapter 3 Lesson 2Tim Ang100% (1)
- AntipsychoticsDocument4 pagesAntipsychoticsRana MuhammadNo ratings yet
- Psychology 1010 Signature Assignment 2 Studying TechniquesDocument4 pagesPsychology 1010 Signature Assignment 2 Studying Techniquesapi-316878786100% (1)
- AI Lec1Document16 pagesAI Lec1CG Art VfxNo ratings yet
- Emergent and Early LiteracyDocument3 pagesEmergent and Early LiteracyJERIC A. REBULLOSNo ratings yet
- The Balanced Musician EssayDocument2 pagesThe Balanced Musician EssayAlexander DavadillaNo ratings yet
- AP Psych Unit 6 VocabDocument3 pagesAP Psych Unit 6 VocabBrooke EmisonNo ratings yet
- Sudn 11Document280 pagesSudn 11triddle1969100% (2)
- Mental State ExaminationDocument2 pagesMental State ExaminationThomasNo ratings yet
- Possibilities: Limitations andDocument12 pagesPossibilities: Limitations andHazel Kinilog88% (8)