You might also like
- Case Study On RDS - NicuDocument32 pagesCase Study On RDS - NicuGandimarei89% (19)
- Laboratory Blood Specimen Tube Type Collection ChartDocument1 pageLaboratory Blood Specimen Tube Type Collection ChartJessie TNo ratings yet
- NUR 450 Medical Surgical Nursing II SyllabusDocument23 pagesNUR 450 Medical Surgical Nursing II SyllabusMohammad Malik0% (2)
- Inclusions HematologyDocument3 pagesInclusions HematologyMurreh100% (3)
- Admission Nursing AssessmentDocument20 pagesAdmission Nursing Assessmentmonir61No ratings yet
- 2021 Batangas Medical Center - Updated Citizens Charter HandbookDocument447 pages2021 Batangas Medical Center - Updated Citizens Charter HandbookHarlyn MagsinoNo ratings yet
- Genetics Table RenalDocument2 pagesGenetics Table RenalDavid KramerNo ratings yet
- Nephrotic Syndrome PDF 2Document2 pagesNephrotic Syndrome PDF 2MNo ratings yet
- Renal DX Flowcharts & Trigger WordsDocument4 pagesRenal DX Flowcharts & Trigger WordsAmber LeJeuneNo ratings yet
- High-Yield NephrologyDocument6 pagesHigh-Yield NephrologyAhmad SobihNo ratings yet
- Nephrotic Nephritic SyndromsDocument4 pagesNephrotic Nephritic SyndromsKimiwari100% (2)
- Renal Pathology TableDocument1 pageRenal Pathology TableFumiko CruzNo ratings yet
- Chapter 20 - The KidneyDocument24 pagesChapter 20 - The KidneyAgnieszka WisniewskaNo ratings yet
- Renal Pathology I. Clinical Manifestations of Renal DiseasesDocument18 pagesRenal Pathology I. Clinical Manifestations of Renal DiseasesKrisha Marie BadilloNo ratings yet
- DISC, Drugs, Infection, Thick Basal MembraneDocument5 pagesDISC, Drugs, Infection, Thick Basal MembraneHOPENo ratings yet
- Disease Key Identification Histology Deposits Nephritic SyndromeDocument5 pagesDisease Key Identification Histology Deposits Nephritic SyndromeSunny RatnaniNo ratings yet
- Glomerular Diseases, Cysts, Renal Stones 2Document7 pagesGlomerular Diseases, Cysts, Renal Stones 2Idris AdeoyeNo ratings yet
- Glomerular Disease and DiureticsDocument26 pagesGlomerular Disease and DiureticsDapot SianiparNo ratings yet
- Medical KidneyDocument13 pagesMedical KidneyJose SirittNo ratings yet
- Disease Cheat SheetDocument393 pagesDisease Cheat Sheetsurviving nursing school50% (2)
- GlomerulonefritisDocument8 pagesGlomerulonefritisdhya0303No ratings yet
- Glomerular Diseases My NotesDocument5 pagesGlomerular Diseases My Notesmalar_km43No ratings yet
- Types of AnaemiaDocument2 pagesTypes of AnaemiaSuhaila NaemaNo ratings yet
- Gemistocytes: Gemistocytic AstrocytomaDocument4 pagesGemistocytes: Gemistocytic AstrocytomaRojales FrancisNo ratings yet
- General Pathology EdgeDocument2 pagesGeneral Pathology EdgeskNo ratings yet
- @acute Nephritic SyndromeDocument3 pages@acute Nephritic SyndromeMazlia FarzanaNo ratings yet
- Bullous Pemphigoid Vs Epydermolysis Bullosa Acquisita: Diagnosis and How To DifferentiateDocument12 pagesBullous Pemphigoid Vs Epydermolysis Bullosa Acquisita: Diagnosis and How To DifferentiateIrene Irene100% (1)
- Glomerular 125Document14 pagesGlomerular 125Surgeeth SKNo ratings yet
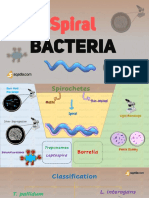
- Spiral: BacteriaDocument28 pagesSpiral: BacteriaZeth MoturiNo ratings yet
- HEMA-1 Up To PG 30.-1-31Document31 pagesHEMA-1 Up To PG 30.-1-31Angela ReyesNo ratings yet
- GlomerulonefritisDocument20 pagesGlomerulonefritisanon-127168100% (1)
- Pathology GlomerulonephritisDocument4 pagesPathology GlomerulonephritisGerardLum100% (2)
- Psychosine: Biochemistry '' Biochemistry '' Section IiDocument1 pagePsychosine: Biochemistry '' Biochemistry '' Section IiMuhammad AbubakarNo ratings yet
- Immune Recap 2Document8 pagesImmune Recap 2ibrahimNo ratings yet
- Pa Tho Physiology of GlomerulonephritisDocument1 pagePa Tho Physiology of GlomerulonephritisJhaziel BermejoNo ratings yet
- Diseases For The BoardsDocument2 pagesDiseases For The BoardsBrendan MillinerNo ratings yet
- BULLOUS DISORDER (4th Yr)Document45 pagesBULLOUS DISORDER (4th Yr)Yahya IftekharNo ratings yet
- Revision Notes Chapter 27878 1Document4 pagesRevision Notes Chapter 27878 1Yuku BabyNo ratings yet
- Asthma Drug StudyDocument2 pagesAsthma Drug StudySheril Sularte CasanesNo ratings yet
- INCREASED CELL DESTRUCTION (Hemolytic Anemia)Document4 pagesINCREASED CELL DESTRUCTION (Hemolytic Anemia)Al DavidNo ratings yet
- Orthopaedics FinalDocument124 pagesOrthopaedics Finaldbchoudhary77No ratings yet
- Renal Pathophysiology: ContentDocument20 pagesRenal Pathophysiology: ContentVittorio Di PaoloNo ratings yet
- Hypersensitivity ImunobiologiDocument14 pagesHypersensitivity Imunobiologinisa humairoNo ratings yet
- ThalassemiaDocument1 pageThalassemiaJobelle Fernandez-SantosNo ratings yet
- Blood Donor SelectionDocument15 pagesBlood Donor SelectionKat JornadalNo ratings yet
- Renal Dse and Metabolic Disorders - 1rDocument26 pagesRenal Dse and Metabolic Disorders - 1rJoan ClaveNo ratings yet
- Supp WNL.0000000000000892 Figure E-2Document1 pageSupp WNL.0000000000000892 Figure E-2SapNo ratings yet
- Obg Class-Enzyme-Complement-DosageDocument2 pagesObg Class-Enzyme-Complement-DosageKaycee Gretz LorescaNo ratings yet
- Target Cells (Codocytes) Most ReliableDocument8 pagesTarget Cells (Codocytes) Most ReliableAnonymouscatNo ratings yet
- Drug Induced Hemolytic AnemiaDocument1 pageDrug Induced Hemolytic AnemiaArnao Maria Mikaela EuniceNo ratings yet
- The Table of Frequent Questions - PathologyDocument14 pagesThe Table of Frequent Questions - PathologyCherry Kola100% (1)
- Anemia Table283Document2 pagesAnemia Table283Bridget ParkerNo ratings yet
- Monoklonal GammapatilerDocument89 pagesMonoklonal GammapatilerBurak KutluNo ratings yet
- SKEMADocument1 pageSKEMAnadhilaNo ratings yet
- Uw - Elseby Notes PediatricsDocument218 pagesUw - Elseby Notes PediatricsIvy QueenNo ratings yet
- CCO Myeloma Nursing TU13 SlidesDocument47 pagesCCO Myeloma Nursing TU13 SlidesLaura TololoiNo ratings yet
- DIC PathophysiologyDocument1 pageDIC Pathophysiologykathy100% (1)
- StaphylococcusDocument13 pagesStaphylococcusZeth MoturiNo ratings yet
- AAD BF Inborn Errors of MetabolismDocument2 pagesAAD BF Inborn Errors of Metabolismkahkashanahmed065No ratings yet
- Heavy Metal Detection Using Aas (Atomic Absorption Spectrophotometer) in Leafy VegetablesDocument30 pagesHeavy Metal Detection Using Aas (Atomic Absorption Spectrophotometer) in Leafy VegetablesKatlene Joy BaytingNo ratings yet
- LEC AUBF Renal-Diseases MIDTERMS 02Document3 pagesLEC AUBF Renal-Diseases MIDTERMS 02Jashmine May TadinaNo ratings yet
- SN 1Document9 pagesSN 1lilisNo ratings yet
- Holotrophic Breathwork Retreat 3-20-2011-1Document9 pagesHolotrophic Breathwork Retreat 3-20-2011-1Jimmy WilsonNo ratings yet
- INFLAMATORY AND STDsDocument26 pagesINFLAMATORY AND STDsNathaniel BudayNo ratings yet
- A Part 1 of Case Study by Angelene Tagle 09 08 2020Document6 pagesA Part 1 of Case Study by Angelene Tagle 09 08 2020pay tinapay100% (1)
- Career Cruising - SurgeonDocument7 pagesCareer Cruising - Surgeonapi-242421326No ratings yet
- Essentials of Microbiology 1st Edition PDFDocument648 pagesEssentials of Microbiology 1st Edition PDFJohn Khna100% (1)
- Endometriosis GuidelineDocument44 pagesEndometriosis GuidelineHen DriNo ratings yet
- Auricular Causative Diagnosis-Finding The Roots of Diseases: A Study of Clinical CasesDocument11 pagesAuricular Causative Diagnosis-Finding The Roots of Diseases: A Study of Clinical Casesyan92120No ratings yet
- Parkinson's DiseaseDocument11 pagesParkinson's DiseaseZA IDNo ratings yet
- Aggregated Disease Comparison Dataset (Updated April 1, 2020)Document830 pagesAggregated Disease Comparison Dataset (Updated April 1, 2020)Jonathan LimaNo ratings yet
- 10 Diagnosa PenyakitDocument3 pages10 Diagnosa PenyakitDiny Rachma Putri HNo ratings yet
- Virtual Notebook 1.1.3 Part 2 - Notebook - Day 2Document6 pagesVirtual Notebook 1.1.3 Part 2 - Notebook - Day 2Justice JensenNo ratings yet
- There Is Good News For Coffee LoversDocument8 pagesThere Is Good News For Coffee Loversani fitriaNo ratings yet
- Kristjansson 2009Document14 pagesKristjansson 2009AdosotoNo ratings yet
- Nursing Care Plan 1 - DiarrheaDocument7 pagesNursing Care Plan 1 - DiarrheakirbyroohNo ratings yet
- Hematocrit (HCT) (Packed Cell Volume PCV) : Objectives: ToDocument19 pagesHematocrit (HCT) (Packed Cell Volume PCV) : Objectives: ToRamadan PhysiologyNo ratings yet
- Bahasa Inggris - NurfadilahDocument6 pagesBahasa Inggris - NurfadilahHardianiNo ratings yet
- Adverse Drug Reaction Monitoring ReportingDocument3 pagesAdverse Drug Reaction Monitoring ReportingMoisés PonceNo ratings yet
- Surgical ICU Exam Content OutlineDocument6 pagesSurgical ICU Exam Content OutlineDarren DawkinsNo ratings yet
- Multiple MyelomaDocument2 pagesMultiple MyelomaKolin JandocNo ratings yet
- Asking Reporting Health Problems & Diagnosing: OlehDocument5 pagesAsking Reporting Health Problems & Diagnosing: Olehsindimei alvianiNo ratings yet
- Health: Quarter 2-Module 4Document26 pagesHealth: Quarter 2-Module 4Ma'am MimiNo ratings yet
- Lab Studies of AnemiaDocument13 pagesLab Studies of Anemiaeki1hidayatNo ratings yet
- Acetaminophen Poisoning Cases - SeptiDocument15 pagesAcetaminophen Poisoning Cases - SeptiseptianasptrNo ratings yet
- Thunderbird Medication and Vaccination ProgramDocument1 pageThunderbird Medication and Vaccination ProgramIntsik R. DominadoNo ratings yet
- Pengaruh Massage Kaki Terhadap Penurunan Insomnia Pada Lansia Di Banjar Temesi Desa Temesi Kabupaten GianyarDocument12 pagesPengaruh Massage Kaki Terhadap Penurunan Insomnia Pada Lansia Di Banjar Temesi Desa Temesi Kabupaten Gianyar119 CIKOKOLNo ratings yet
- Drug Study: Drug Name Contraindications ResponsibilityDocument2 pagesDrug Study: Drug Name Contraindications ResponsibilityJOVEMEA LIRAYNo ratings yet