You might also like
- Ccnapi PDFDocument40 pagesCcnapi PDFZue GonzagaNo ratings yet
- Critical Care Nursing (NCM 410) Notes 1Document66 pagesCritical Care Nursing (NCM 410) Notes 1Danielle OnaNo ratings yet
- Scope of Critical Care Practice: Study GuideDocument6 pagesScope of Critical Care Practice: Study GuideDan Dan ManaoisNo ratings yet
- NCM 118 Notes PrelimDocument35 pagesNCM 118 Notes PrelimCheri-Anne Diaz100% (4)
- St. Mary's College Nursing Program Teaches Critical Care ConceptsDocument33 pagesSt. Mary's College Nursing Program Teaches Critical Care ConceptsAlyssa Gaile EspirituNo ratings yet
- NCM 118 Week 2Document51 pagesNCM 118 Week 2Francis TolentinoNo ratings yet
- NUR 411 - 1. Development of Critical Care Nursing PracticeDocument3 pagesNUR 411 - 1. Development of Critical Care Nursing PracticeEmerson De SilvaNo ratings yet
- Critical CareDocument22 pagesCritical CareJAMES ROD MARINDUQUENo ratings yet
- NUR 411 - 4. Roles of Critical Care NursesDocument4 pagesNUR 411 - 4. Roles of Critical Care NursesEmerson De SilvaNo ratings yet
- About Critical Care NursingDocument7 pagesAbout Critical Care NursingaivynNo ratings yet
- Critical Care PracticeDocument237 pagesCritical Care PracticeKirstin del CarmenNo ratings yet
- Organizing Nursing Services and Patient Care: Case MethodDocument23 pagesOrganizing Nursing Services and Patient Care: Case Methodmerin sunilNo ratings yet
- Introduction To Critical Care Student's PDFDocument52 pagesIntroduction To Critical Care Student's PDFCharles Malcolm DalugdugNo ratings yet
- Madrideo Johnry MAPEH NursesDocument7 pagesMadrideo Johnry MAPEH NursesJohn Lawrence PaduaNo ratings yet
- Framework, Scope and TrendsDocument25 pagesFramework, Scope and TrendsKinjal Vasava100% (5)
- 321-NOTSS5047697 - Job Description PDFDocument13 pages321-NOTSS5047697 - Job Description PDFFatima SilvaNo ratings yet
- Paper: Nurse Duty in WardsDocument7 pagesPaper: Nurse Duty in WardshafidhohNo ratings yet
- The Nature of Scholarship, a Career Legacy Map and Advanced Practice: An Important TriadFrom EverandThe Nature of Scholarship, a Career Legacy Map and Advanced Practice: An Important TriadNo ratings yet
- Intensive CareDocument23 pagesIntensive CareMourian AmanNo ratings yet
- Nursing Service ManagementDocument24 pagesNursing Service ManagementAnilkumar JaraliNo ratings yet
- Critical Care NursingDocument7 pagesCritical Care NursingShilpa JoshiNo ratings yet
- QualityNursingCare IdealsRealitiesImplicationsDocument17 pagesQualityNursingCare IdealsRealitiesImplicationsdanetimbuk901No ratings yet
- DEM Module 1Document48 pagesDEM Module 1Nicolo Martin BelloNo ratings yet
- Standards of Psychiatric Nursing, Current Trends in Psychiatric NursingDocument6 pagesStandards of Psychiatric Nursing, Current Trends in Psychiatric NursingSukanyareddyNo ratings yet
- Principles of Adult Surgical Critical CareFrom EverandPrinciples of Adult Surgical Critical CareNiels D. MartinNo ratings yet
- CarringDocument25 pagesCarringRaka SatriyaNo ratings yet
- Critical Care NursingDocument3 pagesCritical Care NursingRovefrances ErpeluaNo ratings yet
- NSWH RequisitionPD REQ405947Document3 pagesNSWH RequisitionPD REQ405947x.littlevyNo ratings yet
- Futuristic Nursing: By:-Firoz Qureshi Dept. Psychiatric NursingDocument37 pagesFuturistic Nursing: By:-Firoz Qureshi Dept. Psychiatric NursingpadmaNo ratings yet
- Morton Ch01Document11 pagesMorton Ch01headepartmentNo ratings yet
- Management of Nursing ServiceDocument21 pagesManagement of Nursing ServiceLylastikes DianhusadaNo ratings yet
- Critical Care Nursing ConceptsDocument5 pagesCritical Care Nursing ConceptsGodwin Babista GonzalesNo ratings yet
- Final Group Project Revision VersionDocument16 pagesFinal Group Project Revision Versionapi-217735356No ratings yet
- Finals TheoryDocument7 pagesFinals TheoryJulie Ann VisayaNo ratings yet
- AACN BSN Essentials PaperDocument9 pagesAACN BSN Essentials PaperSikany S EmmanNo ratings yet
- ISSUES IN NURSE MIDWIFE PRACTICEDocument27 pagesISSUES IN NURSE MIDWIFE PRACTICEAnusha VergheseNo ratings yet
- NCLEX-RN Exam Prep 2024-2025: 500 NCLEX-RN Test Prep Questions and Answers with ExplanationsFrom EverandNCLEX-RN Exam Prep 2024-2025: 500 NCLEX-RN Test Prep Questions and Answers with ExplanationsNo ratings yet
- Hospice Nurse Job DescriptionDocument5 pagesHospice Nurse Job DescriptionKasia KuzakaNo ratings yet
- Generalization & SpecializatiionmDocument6 pagesGeneralization & SpecializatiionmJennifer DixonNo ratings yet
- Module 2Document64 pagesModule 2nadinecortezgestiadaNo ratings yet
- NSWH RequisitionPD CAM17682Document4 pagesNSWH RequisitionPD CAM17682Anonymous YqCxXQ6wF5No ratings yet
- Critical Care Nursing CompetenciesDocument29 pagesCritical Care Nursing CompetenciesDaniela Rose OrtalNo ratings yet
- Improve Quality Life Cancer PatientsDocument16 pagesImprove Quality Life Cancer PatientsButchay LumbabNo ratings yet
- Formerly Naval State UniversityDocument9 pagesFormerly Naval State Universityjoyrena ochondraNo ratings yet
- Medical Health Clinic: a Social Care Guide Book 2: Social Care Housing and Hotels Conservatism PolicyFrom EverandMedical Health Clinic: a Social Care Guide Book 2: Social Care Housing and Hotels Conservatism PolicyNo ratings yet
- ORGANIZING NURSING SERVICES FOR PATIENT CAREDocument28 pagesORGANIZING NURSING SERVICES FOR PATIENT CAREAnusha VergheseNo ratings yet
- AKIN OTIKO B O Quality Nursing Care in NigeriaThe Ideals Realities and ImplicationsDocument19 pagesAKIN OTIKO B O Quality Nursing Care in NigeriaThe Ideals Realities and ImplicationsUmar Farouq Mohammed GalibNo ratings yet
- What is 21st Century NursingDocument3 pagesWhat is 21st Century Nursingmabel yapuraNo ratings yet
- Extended and Expanded Roles of Nurse AnpDocument10 pagesExtended and Expanded Roles of Nurse AnpSamjhana Neupane80% (5)
- Introduction To Critical Care NursingDocument10 pagesIntroduction To Critical Care NursingRENEROSE TORRES0% (1)
- NSWH RequisitionPD CAM18286Document4 pagesNSWH RequisitionPD CAM18286Charitha RanwalaNo ratings yet
- Nursing Care Plan and Nightingale's Environmental TheoryDocument4 pagesNursing Care Plan and Nightingale's Environmental TheoryBALDOZA LEO FRANCO B.No ratings yet
- Innovations in NursingDocument13 pagesInnovations in NursingShubha JeniferNo ratings yet
- What Is NursingDocument4 pagesWhat Is Nursingalya jinongNo ratings yet
- Lewis: Medical-Surgical Nursing, 10 Edition: Professional Nursing Practice Key Points Professional Nursing PracticeDocument3 pagesLewis: Medical-Surgical Nursing, 10 Edition: Professional Nursing Practice Key Points Professional Nursing PracticePrincess AgarwalNo ratings yet
- Decent Work Employment AND Transcultural Nursing: Noel S. Ayala, MSN, RN, FRINDocument195 pagesDecent Work Employment AND Transcultural Nursing: Noel S. Ayala, MSN, RN, FRINMichtropolisNo ratings yet
- Core Components-Competence NursingDocument2 pagesCore Components-Competence NursingitunuNo ratings yet
- EXTENDED AND EXPANDED ROLE OF NURSEDocument13 pagesEXTENDED AND EXPANDED ROLE OF NURSEharsh.patel180772No ratings yet
- Mental Status Examination: Your Own Words and ObservationsDocument8 pagesMental Status Examination: Your Own Words and ObservationsLadybelle GototosNo ratings yet
- Applying Restraints PDFDocument6 pagesApplying Restraints PDFLadybelle GototosNo ratings yet
- Mse Asssessment GototosDocument6 pagesMse Asssessment GototosLadybelle GototosNo ratings yet
- Age Drug StudyDocument20 pagesAge Drug StudyLadybelle GototosNo ratings yet
- Journal Writing #1 GOTOTOSDocument3 pagesJournal Writing #1 GOTOTOSLadybelle GototosNo ratings yet
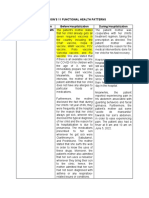
- Gordon's 11 Functional Health PatternsDocument6 pagesGordon's 11 Functional Health PatternsLadybelle GototosNo ratings yet
- Journal - Writing #2 - GOTOTOSDocument3 pagesJournal - Writing #2 - GOTOTOSLadybelle GototosNo ratings yet
- Mse 1Document27 pagesMse 1Ladybelle GototosNo ratings yet
- Question T or FDocument1 pageQuestion T or FLadybelle GototosNo ratings yet
- Sunday Reflection - GototosDocument1 pageSunday Reflection - GototosLadybelle GototosNo ratings yet
- Ladybelle Gototos: COVID-19 Vaccination Online Training Module 1 Entitled "Microplanning"Document1 pageLadybelle Gototos: COVID-19 Vaccination Online Training Module 1 Entitled "Microplanning"Ladybelle GototosNo ratings yet
- Ladybelle P. Gototos Geriatric Nursing Bsn3 Set1 NCPDocument2 pagesLadybelle P. Gototos Geriatric Nursing Bsn3 Set1 NCPLadybelle GototosNo ratings yet
- SL 102 Immediate Care of The Newborn CompetencyDocument2 pagesSL 102 Immediate Care of The Newborn CompetencyLadybelle GototosNo ratings yet
- QuizDocument3 pagesQuizLadybelle GototosNo ratings yet
- Nursing Care Plan for Phobic Anxiety DisorderDocument8 pagesNursing Care Plan for Phobic Anxiety DisorderLadybelle GototosNo ratings yet
- List of Paraphernalia Qty. ParaphernaliaDocument1 pageList of Paraphernalia Qty. ParaphernaliaLadybelle GototosNo ratings yet
- Complete Name of Father/Guardian Complete Name of Mother/ GuardianDocument1 pageComplete Name of Father/Guardian Complete Name of Mother/ GuardianLadybelle GototosNo ratings yet
- Barangay Health Center CertificationDocument1 pageBarangay Health Center CertificationLadybelle GototosNo ratings yet
- AGE Pedia CaseDocument83 pagesAGE Pedia CaseLadybelle GototosNo ratings yet
- Wedding DanceDocument14 pagesWedding DanceLadybelle GototosNo ratings yet
- Area Assessed Technique Used Normal Findings Actual Findings RemarksDocument11 pagesArea Assessed Technique Used Normal Findings Actual Findings RemarksLadybelle GototosNo ratings yet
- Pathophysiology: Tuguegarao City, Cagayan 3500Document2 pagesPathophysiology: Tuguegarao City, Cagayan 3500Ladybelle GototosNo ratings yet
- Drug Study LadyDocument8 pagesDrug Study LadyLadybelle GototosNo ratings yet
- Assumption OF THE Risk AND Waiver OF Liability Relating To Coronavirus/Covid-19Document1 pageAssumption OF THE Risk AND Waiver OF Liability Relating To Coronavirus/Covid-19Ladybelle GototosNo ratings yet
- Dengue Drug Study and NCPDocument22 pagesDengue Drug Study and NCPLadybelle GototosNo ratings yet
- University of Saint LouisDocument10 pagesUniversity of Saint LouisLadybelle GototosNo ratings yet
- LFD PediaDocument1 pageLFD PediaLadybelle GototosNo ratings yet
- Genogram: School OF Health AND Allied Sciences Bachelor of Science in Nursing - Level IiiDocument1 pageGenogram: School OF Health AND Allied Sciences Bachelor of Science in Nursing - Level IiiLadybelle GototosNo ratings yet
- Pathophysiology: School OF Health AND Allied Sciences Bachelor of Science in Nursing - Level IiiDocument4 pagesPathophysiology: School OF Health AND Allied Sciences Bachelor of Science in Nursing - Level IiiLadybelle GototosNo ratings yet
- Speaking Tasks 8 - B1+Document2 pagesSpeaking Tasks 8 - B1+Wayra EvelynNo ratings yet
- Edu 233Document147 pagesEdu 233Abdul Ola IBNo ratings yet
- Surgical Anatomy of the Thyroid GlandDocument86 pagesSurgical Anatomy of the Thyroid GlandsmrutuNo ratings yet
- Alternative Certification 2010Document12 pagesAlternative Certification 2010Michelle Seno Son GonzalesNo ratings yet
- Alexander Rybak - "Europe's Skies" Alexander Rybak - "Europe's Skies"Document1 pageAlexander Rybak - "Europe's Skies" Alexander Rybak - "Europe's Skies"Anh Ngữ Vươn CaoNo ratings yet
- English K 2 Multi Age Year A Unit 1Document46 pagesEnglish K 2 Multi Age Year A Unit 1celine celineNo ratings yet
- Ece-1 2346 ManuscriptDocument12 pagesEce-1 2346 ManuscriptOmer FaridNo ratings yet
- Audit of Receivables Pre-Assessment: Acctg35Document3 pagesAudit of Receivables Pre-Assessment: Acctg35Jeane Mae BooNo ratings yet
- Author's Purpose in WritingDocument37 pagesAuthor's Purpose in WritingJenna Alyssa BaligatNo ratings yet
- 2021 MID-YEAR - Assignment 1 Business Ethics.1Document7 pages2021 MID-YEAR - Assignment 1 Business Ethics.1shayNo ratings yet
- Problem Based Learning Integrating 21 Century Skills: Prepared By:-Alamelu Manggai Ponnusamy Santha Kumari KrishnanDocument18 pagesProblem Based Learning Integrating 21 Century Skills: Prepared By:-Alamelu Manggai Ponnusamy Santha Kumari KrishnanAlamelu Manggai PonnusamyNo ratings yet
- MSI Privacy Policy - EnglishDocument11 pagesMSI Privacy Policy - Englishojik31No ratings yet
- Short Analysis of Geoffrey Hill Septemper SongDocument2 pagesShort Analysis of Geoffrey Hill Septemper SongAnwar SahebNo ratings yet
- Engleza Clasa 1Document4 pagesEngleza Clasa 1Ioana BotarNo ratings yet
- UWORLD Notes by Subject (Main Division) (Usmle Grassroots)Document80 pagesUWORLD Notes by Subject (Main Division) (Usmle Grassroots)Mital Bhakta83% (18)
- Ozark River Bank Cases: 20210821 - Case AnalysisDocument6 pagesOzark River Bank Cases: 20210821 - Case AnalysisTresna AswinNo ratings yet
- Lloyd Vs Grace SmithDocument3 pagesLloyd Vs Grace SmithAkshay Bhasin60% (5)
- 9696 Geography Example Candidate Responses 2011 WEBDocument313 pages9696 Geography Example Candidate Responses 2011 WEBAsma Merchant67% (3)
- Whats New SAP HANA Platform Release Notes enDocument66 pagesWhats New SAP HANA Platform Release Notes enJohn Derteano0% (1)
- Hybrid - 01Document209 pagesHybrid - 01Santos ArwinNo ratings yet
- PROGRAMMING 11 - Q1 - W2 - Mod2 PDFDocument13 pagesPROGRAMMING 11 - Q1 - W2 - Mod2 PDFDianne Brucal - MatibagNo ratings yet
- GrammarDocument10 pagesGrammarRidhan RahmahNo ratings yet
- PhilosophyDocument1 pagePhilosophyElena Luneta-BibeNo ratings yet
- An Instrument of Revival BABALOLADocument46 pagesAn Instrument of Revival BABALOLAGoriola David Gbolahan83% (6)
- What Makes A Family Strong and Successful?Document1 pageWhat Makes A Family Strong and Successful?Chinmayee SrivathsaNo ratings yet
- Assessing ViolenceDocument6 pagesAssessing ViolenceKarlo Jose Dao-ayanNo ratings yet
- Robert FrostDocument8 pagesRobert FrostARIESGA, NICOLE FRANCINE M.No ratings yet
- Recovery of Possession - ComplaintDocument5 pagesRecovery of Possession - ComplaintBleizel TeodosioNo ratings yet
- Astm - C338Document3 pagesAstm - C338KuNtii Devi VerdejofNo ratings yet
- MNM3711 International MarketingDocument70 pagesMNM3711 International MarketingKefiloe MoatsheNo ratings yet