You might also like
- Reyes, Kay Ma. Pearl Serranilla, Denisa Louise Tan, Francisco III Shivpura Sonia MDocument50 pagesReyes, Kay Ma. Pearl Serranilla, Denisa Louise Tan, Francisco III Shivpura Sonia MGeraldine Marie Salvo100% (1)
- Uses of EpidemiologyDocument28 pagesUses of EpidemiologyBinita Shakya0% (1)
- HealthbookDocument71 pagesHealthbookjosetelhadoNo ratings yet
- Kiiko Style Basics PPDocument17 pagesKiiko Style Basics PPjosetelhadoNo ratings yet
- Chapter 5 Epidemiology-CphDocument51 pagesChapter 5 Epidemiology-CphMarcus Randielle FloresNo ratings yet
- Ginott TheoryDocument21 pagesGinott TheoryUmmu SalmahNo ratings yet
- 125 Report Card CommentDocument16 pages125 Report Card CommentNwoye ChinenyeNo ratings yet
- 2022 Textbooks For CIIS Certificate ProgramDocument4 pages2022 Textbooks For CIIS Certificate ProgramjosetelhadoNo ratings yet
- LI Famed HypertensionDocument3 pagesLI Famed HypertensionYolanda Dwi OktaviyaniNo ratings yet
- Objectives of EpidemiologyDocument23 pagesObjectives of EpidemiologyAnitha sujith75% (4)
- The Concept of Epidemiologic Surveillance: Ari UdijonoDocument50 pagesThe Concept of Epidemiologic Surveillance: Ari UdijonoariNo ratings yet
- Chapter 5 EpidemiologyDocument7 pagesChapter 5 EpidemiologyJohn Rick OrineNo ratings yet
- Informative Speech OutlineDocument3 pagesInformative Speech Outlineapi-27792479886% (14)
- Diagoras of Melos A Contribution To The History of Ancient Atheism (Marek Winiarczyk)Document243 pagesDiagoras of Melos A Contribution To The History of Ancient Atheism (Marek Winiarczyk)josetelhadoNo ratings yet
- Richard N. Kocsis (Editor) - Applied Criminal Psychology - A Guide To Forensic Behavioral Sciences-Charles C. Thomas (2009)Document307 pagesRichard N. Kocsis (Editor) - Applied Criminal Psychology - A Guide To Forensic Behavioral Sciences-Charles C. Thomas (2009)Henry CadenasNo ratings yet
- Tungs Acupuncture For Respiratory ConditionsDocument32 pagesTungs Acupuncture For Respiratory ConditionsjosetelhadoNo ratings yet
- Jurnal Psikososial 1Document24 pagesJurnal Psikososial 1Candys KrismayanthiNo ratings yet
- Introduction To Epidemiology Dr. Abdikani Ali MbbsDocument38 pagesIntroduction To Epidemiology Dr. Abdikani Ali Mbbsabdikani hassanNo ratings yet
- Epi Lecture 1 Part IIDocument36 pagesEpi Lecture 1 Part IIMowlidAbdirahman Ali madaaleNo ratings yet
- Adherence Interventions and Outcomes of Tuberculosis Treatment in Low - and Middle-Income Countries (Lmic) : A Systematic Review ProtocolDocument6 pagesAdherence Interventions and Outcomes of Tuberculosis Treatment in Low - and Middle-Income Countries (Lmic) : A Systematic Review Protocolijmb333No ratings yet
- RR 5417Document144 pagesRR 5417Handriyato SukmaNo ratings yet
- Medi 99 E23649Document6 pagesMedi 99 E23649kornelis aribowoNo ratings yet
- Karapet DavtyanDocument8 pagesKarapet Davtyanyenni elfiraNo ratings yet
- Plos Medicine /Article/Crossref/I /Article/Tw Itter/Info /Article/Metrics/Inf Info:Doi/10.1371/J Patient Adher 1185260400000Document25 pagesPlos Medicine /Article/Crossref/I /Article/Tw Itter/Info /Article/Metrics/Inf Info:Doi/10.1371/J Patient Adher 1185260400000khattak_i89No ratings yet
- Effect of Intensive Health Education On Adherence To Treatment in Sputum Positive Pulmonary Tuberculosis PatientsDocument6 pagesEffect of Intensive Health Education On Adherence To Treatment in Sputum Positive Pulmonary Tuberculosis PatientspocutindahNo ratings yet
- Pub Med Penkes 381Document13 pagesPub Med Penkes 381Amanda praditaNo ratings yet
- Prevenvion HivDocument18 pagesPrevenvion HivAna Laura TerusiNo ratings yet
- Concepts in Health 2Document35 pagesConcepts in Health 2kuruvagadda sagarNo ratings yet
- Cigarette Smoking and Health-Promoting Behaviours Among Tuberculosis Patients in Rural AreasDocument9 pagesCigarette Smoking and Health-Promoting Behaviours Among Tuberculosis Patients in Rural AreasMaria FulgensiaNo ratings yet
- Bulsara 2016Document13 pagesBulsara 2016Rizky AmeliaNo ratings yet
- Mining of Nutritional Ingredients in FoodDocument55 pagesMining of Nutritional Ingredients in FoodChintu ReddyNo ratings yet
- CHAPTER 4 Kelompok 3Document45 pagesCHAPTER 4 Kelompok 3tri lestariNo ratings yet
- Scopus TB 1Document11 pagesScopus TB 1ahmad habibNo ratings yet
- Artigo Sobre AidsDocument7 pagesArtigo Sobre AidscamilatututNo ratings yet
- Case Study #3Document26 pagesCase Study #3Reshma MohabeirNo ratings yet
- 1-Introduction MDDocument38 pages1-Introduction MDRasheena RasheeqNo ratings yet
- Jurnal 2Document16 pagesJurnal 2Edwin Pasha Jr.No ratings yet
- Souza Et Al., 2016Document10 pagesSouza Et Al., 2016Ricardo Costa da SilvaNo ratings yet
- Recommendations and Reports OI - HIVDocument323 pagesRecommendations and Reports OI - HIVJevie KairupanNo ratings yet
- Methods 508Document2 pagesMethods 508Nurul MazniNo ratings yet
- "Epidemiology Is The Study of The Distribution and Determinants of Health-The Control of Health ProblemsDocument11 pages"Epidemiology Is The Study of The Distribution and Determinants of Health-The Control of Health ProblemsGwen Dennise MisadorNo ratings yet
- Who Cds CPC TB 99.270Document39 pagesWho Cds CPC TB 99.270Mary Rose Pantinople CejuelaNo ratings yet
- Epidemiologic Mass Treatment 2014Document11 pagesEpidemiologic Mass Treatment 2014TivHa Cii Mpuzz MandjaNo ratings yet
- Epidemiology Lec 2Document45 pagesEpidemiology Lec 2اسامة محمد السيد رمضانNo ratings yet
- Assignment ON Hospital Planning & ManagementDocument9 pagesAssignment ON Hospital Planning & ManagementBhupender MehtoNo ratings yet
- Science of Epidemiology-31.8.'16 Modified On 23.10.2016Document7 pagesScience of Epidemiology-31.8.'16 Modified On 23.10.2016Alankrit PatnaikNo ratings yet
- Evaluation of Diagnostic and Screening 2020 - 21Document28 pagesEvaluation of Diagnostic and Screening 2020 - 21Chinazor cynthia NwachukwuNo ratings yet
- 1-Introduction To PH EpidemiologyDocument33 pages1-Introduction To PH Epidemiologyrabiashoukat7888No ratings yet
- SC 3Document8 pagesSC 3khamilatusyNo ratings yet
- Weeks 2016Document15 pagesWeeks 2016InêsNo ratings yet
- 385-Article Text-3004-1-10-20200518Document5 pages385-Article Text-3004-1-10-20200518Putri AprilliaNo ratings yet
- Module 4 NRSG780Document9 pagesModule 4 NRSG780justdoyourNo ratings yet
- Evidence Based Health Maintenance Protocols (Screening) in Adult/elderlyDocument58 pagesEvidence Based Health Maintenance Protocols (Screening) in Adult/elderlyB 70 Mohit KumarNo ratings yet
- Epidemiology PPTDocument342 pagesEpidemiology PPTTazee Jiituu Tazee JiituuNo ratings yet
- Learning ObjectivesDocument20 pagesLearning ObjectivesOmar MohamedNo ratings yet
- PIIS2214109X20305052Document15 pagesPIIS2214109X20305052Ahsan RaquibNo ratings yet
- EpidemiologyDocument7 pagesEpidemiologyInoxcent MoonNo ratings yet
- Counseling Overweight Patients: Analysis of Preventive Encounters in Primary CareDocument7 pagesCounseling Overweight Patients: Analysis of Preventive Encounters in Primary CareAgil SulistyonoNo ratings yet
- Risk Factors Affecting Multi Drug Resist E36a8f6eDocument13 pagesRisk Factors Affecting Multi Drug Resist E36a8f6eDWI HERU CAHYONONo ratings yet
- 1st LectureDocument6 pages1st LectureNoreen FæţįmæNo ratings yet
- What Is Epidemiology?Document23 pagesWhat Is Epidemiology?KoushikNo ratings yet
- Abstract JURNAL SKRIPSI 2Document11 pagesAbstract JURNAL SKRIPSI 2Ade RatnasariNo ratings yet
- Current Medical DXDocument5 pagesCurrent Medical DXdanklebNo ratings yet
- Hepatitis B Vaccination Coverage Among Health-Care Personnel in The United StatesDocument12 pagesHepatitis B Vaccination Coverage Among Health-Care Personnel in The United StatesRio MulyaNo ratings yet
- LeprosyDocument20 pagesLeprosyHafiz Sulistio UtomoNo ratings yet
- Barriers To Antiretroviral Therapy AdherenceDocument56 pagesBarriers To Antiretroviral Therapy AdherenceAlexandra LionelNo ratings yet
- Tuberculosis Thesis TitleDocument5 pagesTuberculosis Thesis Titletjgyhvjef100% (2)
- Rockson Ohene Asante 2235026 - Epidemiology Assignment by Pratap Kumar Jena SirDocument11 pagesRockson Ohene Asante 2235026 - Epidemiology Assignment by Pratap Kumar Jena SirRockson Ohene AsanteNo ratings yet
- THC:CBD in Daily Practice: Available Data From UK, Germany and SpainDocument3 pagesTHC:CBD in Daily Practice: Available Data From UK, Germany and SpainjosetelhadoNo ratings yet
- Thomas Nadulski, Fritz Pragst, Gordon Weinberg, Patrik Roser, Martin Schnelle, Eva-Maria Fronk, and Andreas Michael StadelmannDocument12 pagesThomas Nadulski, Fritz Pragst, Gordon Weinberg, Patrik Roser, Martin Schnelle, Eva-Maria Fronk, and Andreas Michael StadelmannjosetelhadoNo ratings yet
- The EsophagusDocument3 pagesThe EsophagusjosetelhadoNo ratings yet
- TealistDocument8 pagesTealistjosetelhadoNo ratings yet
- Medical Cannabinoids in Children and Adolescents: A Systematic ReviewDocument18 pagesMedical Cannabinoids in Children and Adolescents: A Systematic ReviewjosetelhadoNo ratings yet
- Proteobacteria: Microbial Signature of Dysbiosis in Gut MicrobiotaDocument8 pagesProteobacteria: Microbial Signature of Dysbiosis in Gut MicrobiotajosetelhadoNo ratings yet
- Jacques Ellul Anarchism and Christianity enDocument17 pagesJacques Ellul Anarchism and Christianity enjosetelhadoNo ratings yet
- The Effect of Acupuncture On The Quality of Life On Patients Recovering From COVID-19Document5 pagesThe Effect of Acupuncture On The Quality of Life On Patients Recovering From COVID-19josetelhadoNo ratings yet
- Efficacy and Adverse Effects of Ginkgo Biloba For Cognitive Impairment and Dementia: A Systematic Review and Meta-AnalysisDocument15 pagesEfficacy and Adverse Effects of Ginkgo Biloba For Cognitive Impairment and Dementia: A Systematic Review and Meta-AnalysisjosetelhadoNo ratings yet
- The Open Insulin Project: A Case Study For Biohacked' MedicinesDocument8 pagesThe Open Insulin Project: A Case Study For Biohacked' MedicinesjosetelhadoNo ratings yet
- Up-Regulating The Human Intestinal Microbiome Using Whole Plant Foods, Polyphenols, And/or FiberDocument7 pagesUp-Regulating The Human Intestinal Microbiome Using Whole Plant Foods, Polyphenols, And/or FiberjosetelhadoNo ratings yet
- Qi and The Virtual in Daoist and Zen LiteratureDocument10 pagesQi and The Virtual in Daoist and Zen LiteraturejosetelhadoNo ratings yet
- U.S. vs. International Prescription Drug PricesDocument77 pagesU.S. vs. International Prescription Drug PricesjosetelhadoNo ratings yet
- Ice 2016 171Document6 pagesIce 2016 171josetelhadoNo ratings yet
- Phytochemical and Pharmacological Studies On Radix Angelica SinensisDocument11 pagesPhytochemical and Pharmacological Studies On Radix Angelica SinensisjosetelhadoNo ratings yet
- The Challenge of EpidemiologyDocument16 pagesThe Challenge of EpidemiologyjosetelhadoNo ratings yet
- Granule List PinyinDocument3 pagesGranule List PinyinjosetelhadoNo ratings yet
- The Wuwei Medical Manuscripts A Brief inDocument61 pagesThe Wuwei Medical Manuscripts A Brief injosetelhadoNo ratings yet
- The Earliest Stone Medical InscriptionDocument16 pagesThe Earliest Stone Medical InscriptionjosetelhadoNo ratings yet
- Gambian DHS 2019-20Document4 pagesGambian DHS 2019-20josetelhadoNo ratings yet
- Body and Mind in Early China and GreeceDocument51 pagesBody and Mind in Early China and GreecejosetelhadoNo ratings yet
- Head 12650Document8 pagesHead 12650josetelhadoNo ratings yet
- RobrichesDocument3 pagesRobrichesGiannis DimitriadisNo ratings yet
- Taller WHS InglésDocument2 pagesTaller WHS InglésStephanie Otero FreayNo ratings yet
- 137 - e New AsresDocument3 pages137 - e New AsresMichael Edward De VillaNo ratings yet
- Ebook PDF Nursing Diagnosis Manual Planning Individualizing and Documenting Client Care 6th EditionDocument35 pagesEbook PDF Nursing Diagnosis Manual Planning Individualizing and Documenting Client Care 6th Editionbarbara.slagle967No ratings yet
- Revista Clínica EspañolaDocument17 pagesRevista Clínica EspañolaGaspar PonceNo ratings yet
- Best PDF of All TimeDocument13 pagesBest PDF of All TimeIsaac glad son izziNo ratings yet
- The Right To Effective Behavioral TreatmentDocument4 pagesThe Right To Effective Behavioral TreatmentFrancesca LeograndeNo ratings yet
- Tonsilitis & Allergic Rhinitis NCPDocument11 pagesTonsilitis & Allergic Rhinitis NCPJorgia SalardaNo ratings yet
- Clinical Staging of Oral Submucous Fibrosis: A Review: Shivakumar.G.C., and Sahana.SDocument4 pagesClinical Staging of Oral Submucous Fibrosis: A Review: Shivakumar.G.C., and Sahana.Smorza rahbrNo ratings yet
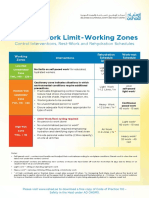
- Thermal Work Limit-Working Zones: Control Interventions, Rest-Work and Rehydration SchedulesDocument1 pageThermal Work Limit-Working Zones: Control Interventions, Rest-Work and Rehydration SchedulesSuprkliNo ratings yet
- Newest Aoi Cheat Sheet 2021Document18 pagesNewest Aoi Cheat Sheet 2021celestieceloveres29No ratings yet
- Roflumilast in Moderate-To-severe COPD Treated With Long Acting Broncho DilatorsDocument18 pagesRoflumilast in Moderate-To-severe COPD Treated With Long Acting Broncho DilatorsMichael LjuslinNo ratings yet
- Career Development Plan For Shs Students (Sy 2019 - 2020) General ObjectivesDocument3 pagesCareer Development Plan For Shs Students (Sy 2019 - 2020) General ObjectivesBeryl AbucejoNo ratings yet
- Diseño Del Nuevo Hospital en ViequesDocument16 pagesDiseño Del Nuevo Hospital en ViequesRedacción WaloNo ratings yet
- Futures Triangle 2.0 Integrating The Futures Triangle With Scenario PlanningDocument11 pagesFutures Triangle 2.0 Integrating The Futures Triangle With Scenario Planningefecto ButterflyNo ratings yet
- The Healthy PersonalityDocument14 pagesThe Healthy PersonalityMaria Edessa TumbaliNo ratings yet
- Food Safety - Sample of Food Safety Incident Report May 2023.v1.0Document10 pagesFood Safety - Sample of Food Safety Incident Report May 2023.v1.0aalampathan76No ratings yet
- Andersen 2002Document7 pagesAndersen 2002Stefania PDNo ratings yet
- Musculoskeletal Implications of Preterm Infant Positioning in The NICUDocument13 pagesMusculoskeletal Implications of Preterm Infant Positioning in The NICUAna LyaNo ratings yet
- Factor Vii DeficiencyDocument12 pagesFactor Vii DeficiencyKaren SalazarNo ratings yet
- The Oriental Insurance Company Limited: UIN: OICHLIP445V032021Document4 pagesThe Oriental Insurance Company Limited: UIN: OICHLIP445V032021Ramit PramanickNo ratings yet
- Mamas Pizza Nutrition FactsDocument2 pagesMamas Pizza Nutrition FactsMonicaNo ratings yet
- Practice Test 04 - Esc 20: phần nghe có tín hiệu. nhạc kết thúc bài ngheDocument19 pagesPractice Test 04 - Esc 20: phần nghe có tín hiệu. nhạc kết thúc bài nghestillaphenomenon50% (2)
- MODULE 1: Physical Education: It's Values To The Developmental and Adjustment of IndividualDocument5 pagesMODULE 1: Physical Education: It's Values To The Developmental and Adjustment of IndividualReyann RabagoNo ratings yet
- Aceite Mineral 70 NF - Carta Sobre NSF Registro - Lubline - Ingles PDFDocument2 pagesAceite Mineral 70 NF - Carta Sobre NSF Registro - Lubline - Ingles PDFRicardo BohorquezNo ratings yet
- Discharge PlanDocument1 pageDischarge PlanlaehaaaNo ratings yet