You might also like
- Jurnal AncDocument9 pagesJurnal AncRezki Jayanti JahidinNo ratings yet
- Utilization of Maternal and Child Health (MCH) Books For Pregnant Women in The Working Area of The Siulak Gedang Health CenterDocument6 pagesUtilization of Maternal and Child Health (MCH) Books For Pregnant Women in The Working Area of The Siulak Gedang Health CenterInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 35 86 6 PBDocument7 pages35 86 6 PBkelompok2ners42No ratings yet
- Maternal mortality determinants in Bondowoso DistrictDocument14 pagesMaternal mortality determinants in Bondowoso DistrictNasmurizalNo ratings yet
- Knowledge on Janani Suraksha Yojana among antenatal mothersDocument18 pagesKnowledge on Janani Suraksha Yojana among antenatal motherspallavi sharmaNo ratings yet
- Relationship between Pregnant Women's Knowledge and Regularity of Antenatal Care ChecksDocument6 pagesRelationship between Pregnant Women's Knowledge and Regularity of Antenatal Care ChecksintanNo ratings yet
- Maternal Health Services Utilization and Its Contributing Factors Among Adolescent MothersDocument11 pagesMaternal Health Services Utilization and Its Contributing Factors Among Adolescent MothersIJPHSNo ratings yet
- Kel1 - Pemanfaatan Aplikasi MPDN Sebagai Upaya Percepatan Penurunan 3Document18 pagesKel1 - Pemanfaatan Aplikasi MPDN Sebagai Upaya Percepatan Penurunan 3Jose YazidNo ratings yet
- Jurnal Metodologi Penelitian (Afria Novita)Document24 pagesJurnal Metodologi Penelitian (Afria Novita)Afria NovitaNo ratings yet
- Original Article: Pregnancy Outcome Between Booked and Unbooked Cases in A Tertiary Level HospitalDocument6 pagesOriginal Article: Pregnancy Outcome Between Booked and Unbooked Cases in A Tertiary Level HospitalNatukunda DianahNo ratings yet
- ABSTRACT: Posyandu Is One Form of Health Efforts Resourceful Community Which Is A RealDocument6 pagesABSTRACT: Posyandu Is One Form of Health Efforts Resourceful Community Which Is A RealUtsmanNo ratings yet
- 2.jurnal Kepkel4Document7 pages2.jurnal Kepkel4Himatul AliyahNo ratings yet
- Latar Belakang 2Document6 pagesLatar Belakang 2Fitri NurullitaNo ratings yet
- Faktor-Faktor Yang Berhubungan Dengan Perilaku Penggunaan Alat Kontrasepsi Pada Wanita Usia Subur Di Puskesmas Jombang-Kota Tangerang SelatanDocument9 pagesFaktor-Faktor Yang Berhubungan Dengan Perilaku Penggunaan Alat Kontrasepsi Pada Wanita Usia Subur Di Puskesmas Jombang-Kota Tangerang Selatanbiostatistika 2019No ratings yet
- Antenatal Services Un PMSMADocument5 pagesAntenatal Services Un PMSMAtkak1995No ratings yet
- Maternal mortality factors in Klaten RegencyDocument14 pagesMaternal mortality factors in Klaten RegencyNasmurizalNo ratings yet
- Faktor-Faktor Yang Berhubungan Dengan Pemanfaatan Posyandu Oleh Ibu Balita Di Kelurahan Kurao Wilayah Kerja Puskesmas Nanggalo Kota Padang Tahun 2015Document10 pagesFaktor-Faktor Yang Berhubungan Dengan Pemanfaatan Posyandu Oleh Ibu Balita Di Kelurahan Kurao Wilayah Kerja Puskesmas Nanggalo Kota Padang Tahun 2015Irna KhairaniNo ratings yet
- Midwife Roles To Decline Maternal Mortality RateDocument5 pagesMidwife Roles To Decline Maternal Mortality RateIJPHSNo ratings yet
- CULTURAL PERSPECTIVESDocument9 pagesCULTURAL PERSPECTIVESApri AnnurNo ratings yet
- Factors Hindering Maternal and Child Health StandardsDocument9 pagesFactors Hindering Maternal and Child Health StandardsVidi YatiNo ratings yet
- 1 PB PDFDocument8 pages1 PB PDFRheny RasidNo ratings yet
- One Client (Osoc) Di Wilayah Kerja Puskesmas SidoharjoDocument7 pagesOne Client (Osoc) Di Wilayah Kerja Puskesmas SidoharjodwiNo ratings yet
- 30-Article Text-59-1-10-20201115Document9 pages30-Article Text-59-1-10-20201115Regita cahyani achmadNo ratings yet
- Ijerph 15 02450 PDFDocument14 pagesIjerph 15 02450 PDFDeby WicaksonoNo ratings yet
- Public Health Journal Article Explores Influence of Media on Toddler Mothers' KnowledgeDocument11 pagesPublic Health Journal Article Explores Influence of Media on Toddler Mothers' KnowledgeUKMPPD Untan Agustus 2018No ratings yet
- Comprehensive Midwifery CareDocument11 pagesComprehensive Midwifery CareYovi pransiska JambiNo ratings yet
- Faktor Penghambat Yankes Maternal Di PKM OwDocument7 pagesFaktor Penghambat Yankes Maternal Di PKM OwAisyah BadmasNo ratings yet
- Faktor Mempengaruhi Kunjungan Ibu Membawa Balita Ke Posyandu Kelurahan Tanjung Pauh Tahun 2018Document8 pagesFaktor Mempengaruhi Kunjungan Ibu Membawa Balita Ke Posyandu Kelurahan Tanjung Pauh Tahun 2018SantriNo ratings yet
- Analisis Faktor Yang Menyebabkan Stunting Di Wilayah Kerja Puskesmas KemangkonDocument9 pagesAnalisis Faktor Yang Menyebabkan Stunting Di Wilayah Kerja Puskesmas KemangkonRindu PandianganNo ratings yet
- Path Analysis On The Determinants of Pap Smear Utilization For Cervical Cancer Early Detection in Women of Reproductive AgeDocument12 pagesPath Analysis On The Determinants of Pap Smear Utilization For Cervical Cancer Early Detection in Women of Reproductive AgeaufaaNo ratings yet
- Inter Journal 5Document9 pagesInter Journal 5NasmurizalNo ratings yet
- Faktor Faktor Yang Berhubungan DenganDocument13 pagesFaktor Faktor Yang Berhubungan DenganrenithawulandarNo ratings yet
- Studi Penggunaan SIJARI EMAS oleh Bidan dalam Rujukan KegawatdaruratanDocument8 pagesStudi Penggunaan SIJARI EMAS oleh Bidan dalam Rujukan KegawatdaruratanAnonymous UHnQSkxLBDNo ratings yet
- 1742-Article Text-3925-1-10-20220217Document6 pages1742-Article Text-3925-1-10-20220217gloryvaraaNo ratings yet
- Inter Journal 1Document7 pagesInter Journal 1NasmurizalNo ratings yet
- Jurnal Kedokteran Dan Kesehatan IndonesiaDocument10 pagesJurnal Kedokteran Dan Kesehatan IndonesiaAmelia MeilaniNo ratings yet
- Learning disabilities in maternal and child health servicesDocument22 pagesLearning disabilities in maternal and child health servicesMuhammad Yusuf UculimaNo ratings yet
- 1997 6488 1 PBDocument8 pages1997 6488 1 PBMuhammad SawalNo ratings yet
- Okolie Stephaine 1-3Document11 pagesOkolie Stephaine 1-3Confidence BlessingNo ratings yet
- Degree - Resea DessDocument48 pagesDegree - Resea DessDessalewNo ratings yet
- ID Hubungan Faktor Sosial Ekonomi Ibu HamilDocument7 pagesID Hubungan Faktor Sosial Ekonomi Ibu HamilUmmahNo ratings yet
- 87-Article Text-166-1-10-20200416Document7 pages87-Article Text-166-1-10-20200416Gholi ZakiyahNo ratings yet
- Faktor-Faktor Yang Mempengaruhi Pelayanan Antenatal Di Daerah Perdesaan: Studi Kualitatif Di Dua Puskemas Kabupaten TrenggalekDocument9 pagesFaktor-Faktor Yang Mempengaruhi Pelayanan Antenatal Di Daerah Perdesaan: Studi Kualitatif Di Dua Puskemas Kabupaten TrenggalekDewi R. AdityaNo ratings yet
- The Enabling Factors in Improving Maternal and Child Health in Lamboya District, West SumbaDocument19 pagesThe Enabling Factors in Improving Maternal and Child Health in Lamboya District, West Sumbaeva agustinaNo ratings yet
- Artikel - Seny Komalasari SA - 215130016P - S1 Kesehatan MasyarakatDocument11 pagesArtikel - Seny Komalasari SA - 215130016P - S1 Kesehatan MasyarakatSenny KomalasariNo ratings yet
- Hub Peng&Sikap Ibu DG K4Document9 pagesHub Peng&Sikap Ibu DG K4Fitri Nur HidayahNo ratings yet
- Perspektif Perawat Tentang Manejemen Terpadu Balita Sakit Di Puskesmas Wilayah Kabupaten Bantul YogyakartaDocument6 pagesPerspektif Perawat Tentang Manejemen Terpadu Balita Sakit Di Puskesmas Wilayah Kabupaten Bantul Yogyakartadenilay richardoNo ratings yet
- 2159-Article Text-4965-1-10-20230310Document7 pages2159-Article Text-4965-1-10-20230310najwaazzahra2121No ratings yet
- A Study On Knowledge and Practices of Antenatal CaDocument9 pagesA Study On Knowledge and Practices of Antenatal Cameera dukareNo ratings yet
- Community Health Worker Empowerment Through Collaborative Models With Community MidwiferyDocument8 pagesCommunity Health Worker Empowerment Through Collaborative Models With Community MidwiferyIJPHSNo ratings yet
- 28-Article Text-99-1-10-20160413.id - enDocument6 pages28-Article Text-99-1-10-20160413.id - enHARYATINo ratings yet
- Jurnal Kesehatan Masyarakat: Determinant of Teenage PregnanciesDocument7 pagesJurnal Kesehatan Masyarakat: Determinant of Teenage PregnanciesAc IrawanNo ratings yet
- 10.+GALLEY Fery+FerdiansyahDocument7 pages10.+GALLEY Fery+Ferdiansyahkelompok2ners42No ratings yet
- Tugas Bu Dian - Nasmira (Akk5 Ekstensi)Document19 pagesTugas Bu Dian - Nasmira (Akk5 Ekstensi)muhammad yusufNo ratings yet
- Pancasakti Journal of Public Health Science and Research: Miftahul Jannah, Erlina Wanti Harahap, Razia Begum SuroyoDocument5 pagesPancasakti Journal of Public Health Science and Research: Miftahul Jannah, Erlina Wanti Harahap, Razia Begum SuroyoElyani TambunanNo ratings yet
- Perawatan Kehamilan Dalam Perspektif Budaya Madura Di Desa Tambak Dan Desa Rapalaok Kecamatan Omben Kabupaten Sampang PDFDocument13 pagesPerawatan Kehamilan Dalam Perspektif Budaya Madura Di Desa Tambak Dan Desa Rapalaok Kecamatan Omben Kabupaten Sampang PDFZacky MarzukiNo ratings yet
- Peran Suami dalam Perawatan Kehamilan IstriDocument9 pagesPeran Suami dalam Perawatan Kehamilan IstriDiky ArdinansyahNo ratings yet
- Tugas Review Report SholehatulDocument12 pagesTugas Review Report SholehatulnesyaanandaNo ratings yet
- 1 PBDocument11 pages1 PBdimaNo ratings yet
- Neonatal Nursing: Scope and Standards of PracticeFrom EverandNeonatal Nursing: Scope and Standards of PracticeRating: 4 out of 5 stars4/5 (1)
- CRN Man PDM 002 Design Management ManualDocument102 pagesCRN Man PDM 002 Design Management ManualReda GuellilNo ratings yet
- Teaching: Health Education ReviewerDocument12 pagesTeaching: Health Education ReviewerphoebeNo ratings yet
- Education 2788023Document26 pagesEducation 2788023RasdianaNo ratings yet
- CSTP 3 Meadows 5 4 22Document7 pagesCSTP 3 Meadows 5 4 22api-528348325No ratings yet
- Bronfenbrenner Ecological TheoryDocument9 pagesBronfenbrenner Ecological TheoryLorena SoqueNo ratings yet
- Discriminant Validity Assessment in PLS-SEM: A Comprehensive Composite-Based ApproachDocument9 pagesDiscriminant Validity Assessment in PLS-SEM: A Comprehensive Composite-Based Approachabdallah elgendyNo ratings yet
- SITXCOM010 Student GuideDocument18 pagesSITXCOM010 Student GuideDilbar PathakNo ratings yet
- Setswana Puo Ya Gae - Mophato 2 Kgweditharo 3 2021Document7 pagesSetswana Puo Ya Gae - Mophato 2 Kgweditharo 3 2021Meddie Ya KatlegoNo ratings yet
- Manual de PPAPDocument71 pagesManual de PPAPirvingemmanuel gonzalezNo ratings yet
- Edu 105 L2Document2 pagesEdu 105 L2Keannu EstoconingNo ratings yet
- UGC List of Journals 20200715Document70 pagesUGC List of Journals 20200715chakradhar JadhavNo ratings yet
- Implementasi Data Mining Menggunakan Algoritma Apriori Untuk Mengetahui Pola Peminjaman BukuDocument10 pagesImplementasi Data Mining Menggunakan Algoritma Apriori Untuk Mengetahui Pola Peminjaman BukuChristin IrcNo ratings yet
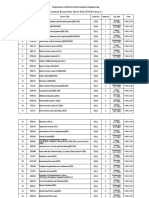
- Terminal Exams Date Sheet-Fall 2020 (Version-1) : Department of Electrical and Computer EngineeringDocument6 pagesTerminal Exams Date Sheet-Fall 2020 (Version-1) : Department of Electrical and Computer EngineeringMuhammad Zaeem AkmalNo ratings yet
- Impact of Modular Learning on Slow LearnersDocument3 pagesImpact of Modular Learning on Slow LearnersAbdulrahman Abarani AdamNo ratings yet
- Beyond The Hype: A Guide To Understanding and Successfully Implementing Artificial Intelligence Within Your BusinessDocument20 pagesBeyond The Hype: A Guide To Understanding and Successfully Implementing Artificial Intelligence Within Your BusinessNitin RamnaniNo ratings yet
- Ai Set A QPDocument6 pagesAi Set A QPwicked sunny33% (3)
- 26167159Document23 pages26167159rainamarie.galit.abNo ratings yet
- Human Robot InteractionDocument418 pagesHuman Robot InteractionEduardo Andres GerleinNo ratings yet
- Chatbot AssistantDocument9 pagesChatbot AssistantKanhaiya VermaNo ratings yet
- Ucsp Week 6Document3 pagesUcsp Week 6KimberlyNo ratings yet
- Demography and Health Services StatisticsDocument74 pagesDemography and Health Services StatisticsHamse AdenNo ratings yet
- Biology in the 21st Century: Post Genomic EraDocument3 pagesBiology in the 21st Century: Post Genomic EraNani NaniNo ratings yet
- Reference - PidcockArticle - InfoGridDocument2 pagesReference - PidcockArticle - InfoGridIhar KuznecovNo ratings yet
- Eapp SLHT Q2 Week 5 6Document21 pagesEapp SLHT Q2 Week 5 6Emz Sandoval AmanteNo ratings yet
- Approaches to Studying Political SystemsDocument15 pagesApproaches to Studying Political SystemsKaren TolentinoNo ratings yet
- Robots and service innovation in health careDocument5 pagesRobots and service innovation in health caredavid frybergNo ratings yet
- TNCT Third Quarter Summative TestDocument4 pagesTNCT Third Quarter Summative TestSyvon SabitNo ratings yet
- ECE 1003 Week 2Document16 pagesECE 1003 Week 2TEMNo ratings yet
- A Brief Introduction To Behavioural Accounting & The Academic Achievements of Professor Chen's TeamDocument45 pagesA Brief Introduction To Behavioural Accounting & The Academic Achievements of Professor Chen's TeamMohammed I. AzamNo ratings yet
- Module - Unit 1 - Facilitating - Learner - Centered TeachingDocument6 pagesModule - Unit 1 - Facilitating - Learner - Centered TeachingImee EusebioNo ratings yet