You might also like
- FNP Module 3Document5 pagesFNP Module 3Jewel Berbano IINo ratings yet
- Ethical Dilemma in NSG MGMTDocument4 pagesEthical Dilemma in NSG MGMTAhmad BaolayyanNo ratings yet
- Admission Procedure For The Critically Ill PatientDocument3 pagesAdmission Procedure For The Critically Ill Patientgeorgeloto12100% (1)
- Ethical Legal Assign 3Document7 pagesEthical Legal Assign 3Armie CapinpinNo ratings yet
- AssignmentDocument3 pagesAssignmentKim Rose SabuclalaoNo ratings yet
- Autonomy & The Refusal of Lifesaving TreatmentDocument8 pagesAutonomy & The Refusal of Lifesaving TreatmentdorkyguyNo ratings yet
- 10 Right To Refuse Participation in Medical ResearchDocument4 pages10 Right To Refuse Participation in Medical ResearchShiela Ocho100% (1)
- 13Document12 pages13Kamal Kumar Kamal KumarNo ratings yet
- Attending Physicians Statement Crisis Cover Renal Failure - 041222Document2 pagesAttending Physicians Statement Crisis Cover Renal Failure - 041222max leeNo ratings yet
- Patients Bill of RightsDocument1 pagePatients Bill of RightschibieNo ratings yet
- Emj Cases : Questions For Case 1Document8 pagesEmj Cases : Questions For Case 1Azmyza Azmy100% (1)
- Group Presentation - The Right To DieDocument26 pagesGroup Presentation - The Right To DieYuki WilliamsNo ratings yet
- Consent Medical ProceduresDocument2 pagesConsent Medical ProcedureserenealNo ratings yet
- 362 Ethics PresentationDocument15 pages362 Ethics Presentationapi-302320251No ratings yet
- Presentation 1Document16 pagesPresentation 1Azhari AhmadNo ratings yet
- Fake Abortion Form TemplateDocument4 pagesFake Abortion Form Templateyouismyfavcolour67% (3)
- This I BelieveDocument3 pagesThis I Believeapi-302583687No ratings yet
- Moral Deliberation 2Document6 pagesMoral Deliberation 2christie clausNo ratings yet
- Case Scenario AnalysisDocument2 pagesCase Scenario AnalysisAmbot sa ImoNo ratings yet
- Ethical Dilemmas in The Pediatric Emergency Room LGGDocument35 pagesEthical Dilemmas in The Pediatric Emergency Room LGGapi-136237609No ratings yet
- LEGMED CaseDocument16 pagesLEGMED CaseGabriel Jhick SaliwanNo ratings yet
- JHH Patient HandbookDocument32 pagesJHH Patient Handbookkxalxo7637100% (1)
- Involuntary Psychiatric Hold: Commitment Continued Based On Nurse's TestimonyDocument1 pageInvoluntary Psychiatric Hold: Commitment Continued Based On Nurse's TestimonyMei ZhangNo ratings yet
- Case Scenario Pre-Operative Case Analysis 1 (Group 1)Document5 pagesCase Scenario Pre-Operative Case Analysis 1 (Group 1)Rej GarbosaNo ratings yet
- Admission and Basic Nursing CareDocument26 pagesAdmission and Basic Nursing CareKardana PutraNo ratings yet
- Medical Ethics NotesDocument11 pagesMedical Ethics NotesMuhammad Waqar RehanNo ratings yet
- Treatment Refusal - Legal and Ethical IssuesDocument5 pagesTreatment Refusal - Legal and Ethical IssuesPulok DkNo ratings yet
- DNR: Legal and Moral Challenges To Health ProfessionalsDocument20 pagesDNR: Legal and Moral Challenges To Health ProfessionalsMarissa AsimNo ratings yet
- Advance Directives 230752 7Document47 pagesAdvance Directives 230752 7api-198352965100% (1)
- Patient Rights and ResponsibilitiesDocument4 pagesPatient Rights and Responsibilitiespizzyray640No ratings yet
- Test Bank For Priorities in Critical Care Nursing 7th Edition Linda D Urden Kathleen M Stacy Mary e LoughDocument7 pagesTest Bank For Priorities in Critical Care Nursing 7th Edition Linda D Urden Kathleen M Stacy Mary e Loughhannahmartintgmbdcxkjf100% (20)
- This Is Me Now - Danielle SwartzDocument9 pagesThis Is Me Now - Danielle Swartzapi-508771384No ratings yet
- Contoh General ConsentDocument1 pageContoh General ConsentMahendra AbdythamaNo ratings yet
- Patient's Bill of Rights: Information For PatientsDocument5 pagesPatient's Bill of Rights: Information For PatientsMamemi AlonzoNo ratings yet
- PD PaperDocument4 pagesPD PaperMafie BarreiroNo ratings yet
- Healthcare InvestigationDocument10 pagesHealthcare Investigationapi-586722985No ratings yet
- Ethical Aspects of Withholding and Withdrawing Life Sustaining TreatmentDocument15 pagesEthical Aspects of Withholding and Withdrawing Life Sustaining TreatmentwakldNo ratings yet
- Ethical PrinciplesDocument34 pagesEthical PrinciplesEniamrahs DnalonNo ratings yet
- Group 2 Dignity in Death and Dying EthicsDocument8 pagesGroup 2 Dignity in Death and Dying EthicsNicole BartolomeNo ratings yet
- Referat EticaDocument5 pagesReferat EticaCarp Petru-CosminNo ratings yet
- Rielle Bioethics AssDocument7 pagesRielle Bioethics Assdrae syNo ratings yet
- Case Study 011Document5 pagesCase Study 011salim omarNo ratings yet
- Ethical Reasoning PaperDocument10 pagesEthical Reasoning Paperapi-609576676No ratings yet
- Patient and Family Rights and ResponsibilitiesDocument5 pagesPatient and Family Rights and Responsibilitiesnabh2019 inuNo ratings yet
- Consent For Hemodialysis: Name of PatientDocument11 pagesConsent For Hemodialysis: Name of PatientSyamsul BahriNo ratings yet
- Pro Debate - AGDocument3 pagesPro Debate - AGAkilah GilzeneNo ratings yet
- Dr. Ali's Uworld Notes For Step 2 CKDocument8 pagesDr. Ali's Uworld Notes For Step 2 CKnaimNo ratings yet
- Case 4Document2 pagesCase 4Elaine MacalandaNo ratings yet
- 362 Ethics PresentationDocument15 pages362 Ethics Presentationapi-302664277No ratings yet
- Patient's Bill of Rights & ResponsibilitiesDocument2 pagesPatient's Bill of Rights & ResponsibilitiesepingNo ratings yet
- Capacity, confidentiality, consent and driving issues in healthcareDocument8 pagesCapacity, confidentiality, consent and driving issues in healthcarePiratheepan TNo ratings yet
- This I Believe at The End of The SemesterDocument4 pagesThis I Believe at The End of The Semesterapi-322673257No ratings yet
- CasesDocument7 pagesCaseswenny capplemanNo ratings yet
- Ethical Principles in HealthcareDocument15 pagesEthical Principles in HealthcareMajkel Benche CustodioNo ratings yet
- This I Believe 1Document3 pagesThis I Believe 1api-709406220No ratings yet
- Communication With and On Behalf of PatientsDocument133 pagesCommunication With and On Behalf of PatientsDes Anggraeni RuniasiwiNo ratings yet
- Resuscitation Decisions at The End of Life: The Final DecisionsDocument3 pagesResuscitation Decisions at The End of Life: The Final DecisionsDaniela DanaNo ratings yet
- Euthanasia Arguments in FavorDocument4 pagesEuthanasia Arguments in FavorDanna MaregocioNo ratings yet
- Hs 2050 This Is Me Now TemplateDocument7 pagesHs 2050 This Is Me Now Templateapi-494872599No ratings yet
- Normal Probability Distribution PDFDocument17 pagesNormal Probability Distribution PDFChe SalveronNo ratings yet
- INSTRUCTIONAL STRATEGIES To PrintDocument5 pagesINSTRUCTIONAL STRATEGIES To PrintChe SalveronNo ratings yet
- Nursing Diagnosis and InterventionsDocument4 pagesNursing Diagnosis and InterventionsChe SalveronNo ratings yet
- Laws On Philippine EducationDocument26 pagesLaws On Philippine EducationChe SalveronNo ratings yet
- Dawn Editorials+opinions With Urdu Translation.Document35 pagesDawn Editorials+opinions With Urdu Translation.Agha Khan DurraniNo ratings yet
- Laboratory-Activities 1 and 2Document18 pagesLaboratory-Activities 1 and 2Raymund Melindo RubioNo ratings yet
- Code of Ethics-American Counseling AssociationDocument51 pagesCode of Ethics-American Counseling AssociationJohn Carlo PerezNo ratings yet
- Tle 8-Beautycare-Q4-M7Document8 pagesTle 8-Beautycare-Q4-M7Belinda OrigenNo ratings yet
- Examen 2 ParteDocument3 pagesExamen 2 ParteGeraldine Sierra GomezNo ratings yet
- ABSTRACT - BOOK - 10th IcgsDocument135 pagesABSTRACT - BOOK - 10th Icgsd_kourkoutasNo ratings yet
- Hyland's 4 Kids Day & Night Cold 'N Cough Relief Liquid - 8 FL Oz TargetDocument1 pageHyland's 4 Kids Day & Night Cold 'N Cough Relief Liquid - 8 FL Oz TargetKarma JigmeyNo ratings yet
- Chapter Quiz 1. MCNDocument4 pagesChapter Quiz 1. MCNAngie SaquingNo ratings yet
- Pembrolizumab Plus Pemetrexedplatinum For Metastatic Nonsquamous NSCLC KEYNOTE 189 Japan StudyDocument11 pagesPembrolizumab Plus Pemetrexedplatinum For Metastatic Nonsquamous NSCLC KEYNOTE 189 Japan StudyasdffdsaNo ratings yet
- Lower Section Caeserian SectionDocument7 pagesLower Section Caeserian SectionSampat Kumawat100% (4)
- Lydia Hall Nursing TheoryDocument1 pageLydia Hall Nursing TheoryJohn Patrick Bernada100% (1)
- Homework Should Be Banned Pros and ConsDocument7 pagesHomework Should Be Banned Pros and Consafnofjmzeldfie100% (1)
- IEP-Anikka Rebecca Alarcon (DepEd)Document6 pagesIEP-Anikka Rebecca Alarcon (DepEd)may may abelleraNo ratings yet
- OSHC Guide: Support When Studying AbroadDocument12 pagesOSHC Guide: Support When Studying AbroadIgnacio CorreaNo ratings yet
- Cirugía de Colon Abierta Con "Fast Track" o Recuperación AceleradaDocument10 pagesCirugía de Colon Abierta Con "Fast Track" o Recuperación AceleradaManuelEduardoSanchezSotoNo ratings yet
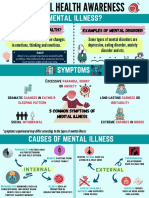
- Mental Health AwarenessDocument2 pagesMental Health Awarenessfarhatulhanimzulkifl100% (2)
- Firefighter Candidate Prep GuideDocument21 pagesFirefighter Candidate Prep GuideEric Levy100% (1)
- Rasika DietitianDocument3 pagesRasika DietitianChrill DsilvaNo ratings yet
- MDC COVID-19 Mandatory Health Safety Protocols Upon Work Resumption - V5 20200513Document13 pagesMDC COVID-19 Mandatory Health Safety Protocols Upon Work Resumption - V5 20200513Clarabelle Mae Dela RosaNo ratings yet
- The Effect of 5S On Employee Performance: An Empirical Study Among Lebanese HospitalsDocument7 pagesThe Effect of 5S On Employee Performance: An Empirical Study Among Lebanese HospitalsMuthu BaskaranNo ratings yet
- LCD in Health G10Document3 pagesLCD in Health G10Cynthia LuayNo ratings yet
- Regional Family Planning Inventory FormsDocument2 pagesRegional Family Planning Inventory FormsRANDY BAOGBOGNo ratings yet
- Sas-3.pmls1-Mls 037Document9 pagesSas-3.pmls1-Mls 037Michael MarzonNo ratings yet
- Covid-19 Annotated BibliographyDocument5 pagesCovid-19 Annotated BibliographyBrian kwenaNo ratings yet
- Agesta Sacred Codes ListDocument22 pagesAgesta Sacred Codes Listmimigogo92% (12)
- Practices of Exclusive Breastfeeding Among Lactating Mothers Attending Care at HoimaDocument7 pagesPractices of Exclusive Breastfeeding Among Lactating Mothers Attending Care at HoimaKIU PUBLICATION AND EXTENSIONNo ratings yet
- Uncut Enamel For Optimizing Bonded Composite Restoration On MultiDocument8 pagesUncut Enamel For Optimizing Bonded Composite Restoration On MultiJack GoldenNo ratings yet
- Sicat Surgical Guide Manual PDFDocument56 pagesSicat Surgical Guide Manual PDFvashishtanatomyNo ratings yet
- FlowerhornDocument10 pagesFlowerhornPaul Michael P. GarciaNo ratings yet
- CounterclaimsDocument3 pagesCounterclaimsRuthie PatootieNo ratings yet