You might also like
- Service ManualDocument582 pagesService ManualBogdan Popescu100% (5)
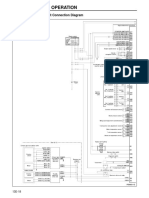
- Structure and Operation: 3. Electronic Control Unit Connection DiagramDocument16 pagesStructure and Operation: 3. Electronic Control Unit Connection DiagramAung Hlaing Min MyanmarNo ratings yet
- C7 On-Highway Engine Electrical System: Harness and Wire Electrical Schematic SymbolsDocument2 pagesC7 On-Highway Engine Electrical System: Harness and Wire Electrical Schematic SymbolsFeDe Aavina Glez100% (3)
- Hymen Facts and Conceptions PDFDocument7 pagesHymen Facts and Conceptions PDFPriscilla PumpkinNo ratings yet
- Pi Is 0889540615010732Document17 pagesPi Is 0889540615010732Sri RengalakshmiNo ratings yet
- 01.introduction To Earth ScienceDocument29 pages01.introduction To Earth ScienceIshan Chua100% (1)
- P&G Interview QuestionsDocument2 pagesP&G Interview Questionssupu100% (3)
- Beamforming For 4.9G/5G Networks: Exploiting Massive MIMO and Active Antenna TechnologiesDocument12 pagesBeamforming For 4.9G/5G Networks: Exploiting Massive MIMO and Active Antenna TechnologiesAymen Ben zinebNo ratings yet
- 2004-Skull Deformities-Emily B PDFDocument29 pages2004-Skull Deformities-Emily B PDFDavid Expósito González100% (1)
- H&M Case Study AssignmentDocument7 pagesH&M Case Study AssignmentwqvyakNo ratings yet
- Deformational Plagiocephaly: Diagnosis, Prevention, and TreatmentDocument12 pagesDeformational Plagiocephaly: Diagnosis, Prevention, and TreatmentSelene MéndezNo ratings yet
- Cranial Deformation Lekovic Et Al 2007 NeurosurgeryDocument11 pagesCranial Deformation Lekovic Et Al 2007 NeurosurgeryanychunliNo ratings yet
- Positional Plagiocephaly Evaluati - 2004 - Oral and Maxillofacial Surgery CliniDocument8 pagesPositional Plagiocephaly Evaluati - 2004 - Oral and Maxillofacial Surgery Clinilaljadeff12No ratings yet
- Crecimiento Craneo FacialDocument9 pagesCrecimiento Craneo FacialKatherine CharallaNo ratings yet
- Difficult Questions Facing The CR 2004 Oral and Maxillofacial Surgery ClinicDocument10 pagesDifficult Questions Facing The CR 2004 Oral and Maxillofacial Surgery Cliniclaljadeff12No ratings yet
- Definition and Epydemiology OxycephalyDocument14 pagesDefinition and Epydemiology Oxycephalyzaldi basalamahNo ratings yet
- Pediatric RehabDocument32 pagesPediatric RehabRainy DaysNo ratings yet
- Espina Bifida 2022Document7 pagesEspina Bifida 2022Edwin Fabian Paz UrbanoNo ratings yet
- Torticollis, Facial Asymmetry and Plagiocephaly in Normal NewbornsDocument6 pagesTorticollis, Facial Asymmetry and Plagiocephaly in Normal NewbornsJuan Pablo PérezNo ratings yet
- The "Epidemic" of Occipital Flattening: Why It Is Happening and What To Do About ItDocument5 pagesThe "Epidemic" of Occipital Flattening: Why It Is Happening and What To Do About ItDinner and a Donkey Show TheatreNo ratings yet
- Characteristics, Head Shape Measurements and Developmental Delay in 287 Consecutive Infants Attending A Plagiocephaly ClinicDocument6 pagesCharacteristics, Head Shape Measurements and Developmental Delay in 287 Consecutive Infants Attending A Plagiocephaly ClinicchiaraNo ratings yet
- Avoiding The Sequela Associated With Deformational PlagiocephalyDocument8 pagesAvoiding The Sequela Associated With Deformational PlagiocephalychiaraNo ratings yet
- The Aetiology of Adolescent Idiopathic Scoliosis: Is Sleep Position The Missing Link? The Nighttime Perfect Storm HypothesisDocument22 pagesThe Aetiology of Adolescent Idiopathic Scoliosis: Is Sleep Position The Missing Link? The Nighttime Perfect Storm HypothesisIJAR JOURNALNo ratings yet
- Jcad 14 3 14Document3 pagesJcad 14 3 14Gerardo Valenzuela GonzálezNo ratings yet
- Phimosis 5 PDFDocument4 pagesPhimosis 5 PDFNurul YaqinNo ratings yet
- Are Humans Still Evolving?Document4 pagesAre Humans Still Evolving?Tony SorgeNo ratings yet
- Craniofacial Growth, Maturation, and Change: Teens To MidadulthoodDocument4 pagesCraniofacial Growth, Maturation, and Change: Teens To MidadulthoodOmar DSNo ratings yet
- Biología Craneofacial Fan2012Document7 pagesBiología Craneofacial Fan2012andresNo ratings yet
- 2005-Positional Skull Deformities in Children Skull Deformation Without Synostosis-Juan F. Martínez-Lage PDFDocument7 pages2005-Positional Skull Deformities in Children Skull Deformation Without Synostosis-Juan F. Martínez-Lage PDFDavid Expósito GonzálezNo ratings yet
- Positional Plagiocephaly: An Analysis of The Literature On The Effectiveness of Current GuidelinesDocument9 pagesPositional Plagiocephaly: An Analysis of The Literature On The Effectiveness of Current GuidelinesManjunath VaddambalNo ratings yet
- AntropologieDocument10 pagesAntropologieBianca GherghelucaNo ratings yet
- Human Malformations - 08 - Facial BonesDocument30 pagesHuman Malformations - 08 - Facial BonesAhmed H. Ali ElbestaweyNo ratings yet
- 2007 Article 20Document14 pages2007 Article 20Valeska Acevedo GodoyNo ratings yet
- The Management of Disorders of the Child’s Cervical SpineFrom EverandThe Management of Disorders of the Child’s Cervical SpineDaniel J. HedequistNo ratings yet
- Persing 2003Document6 pagesPersing 2003AYMARA GABRIELA MORENO SANCHEZNo ratings yet
- Cranial Sutures: A Brief Review: SummaryDocument9 pagesCranial Sutures: A Brief Review: SummaryImane LoukdacheNo ratings yet
- Pathologic and Physiologic PhimosisDocument7 pagesPathologic and Physiologic Phimosisdianita507No ratings yet
- Artificial Deformation of The Human Skull: A Review (2006)Document6 pagesArtificial Deformation of The Human Skull: A Review (2006)InterestingScienceNo ratings yet
- 4 Anatomibirth DefectDocument51 pages4 Anatomibirth Defectwahyu ashariNo ratings yet
- Seminar: PathophysiologyDocument12 pagesSeminar: PathophysiologyMerlin MuktialiNo ratings yet
- Developmental Medicine & Child NeurologyDocument7 pagesDevelopmental Medicine & Child Neurologyallyssa rahmadittaNo ratings yet
- Volume 42 1 97 2Document11 pagesVolume 42 1 97 2AnindyaMustikaNo ratings yet
- The Morphogenesis of Wormian Bones A Study of Craniosynostosis and Purposeful Cranial DeformationDocument9 pagesThe Morphogenesis of Wormian Bones A Study of Craniosynostosis and Purposeful Cranial DeformationSara FabijanićNo ratings yet
- Tory 18-25, 1984,: News andDocument1 pageTory 18-25, 1984,: News andMichelle Tieden MazanecNo ratings yet
- C - Infantparent Cosleeping in An Evolutionary Perspective Implicati 1993Document20 pagesC - Infantparent Cosleeping in An Evolutionary Perspective Implicati 1993hannanatalilustNo ratings yet
- DiscursoDocument21 pagesDiscursoLeslye SimbañaNo ratings yet
- Emotional Neglect in Childhood and Cerebral Infarction in Older AgeDocument8 pagesEmotional Neglect in Childhood and Cerebral Infarction in Older AgeOlward TôNo ratings yet
- Cerebral Palsy-1 PDFDocument94 pagesCerebral Palsy-1 PDFgpediatrics myNo ratings yet
- Nonsyndromic Craniosynostosis Diagnosis - 2004 - Oral and Maxillofacial SurgerDocument17 pagesNonsyndromic Craniosynostosis Diagnosis - 2004 - Oral and Maxillofacial Surgerlaljadeff12No ratings yet
- Skeletal Abnormalities of The Upper Limbs - Neonatal Diagnosis of 49XXXXY SyndromeDocument4 pagesSkeletal Abnormalities of The Upper Limbs - Neonatal Diagnosis of 49XXXXY SyndromeFelipe TavaresNo ratings yet
- Term Paper On EugenicsDocument7 pagesTerm Paper On Eugenicsafmzydxcnojakg100% (1)
- Silent Risk: Issues About the Human Umbilical Cord (Second Edition)From EverandSilent Risk: Issues About the Human Umbilical Cord (Second Edition)No ratings yet
- Fetus Food in China - Research PaperDocument15 pagesFetus Food in China - Research PaperjanikkaNo ratings yet
- Cranio Syn Ostos IsDocument17 pagesCranio Syn Ostos IsAchmad FitrahNo ratings yet
- Theories of GrowthDocument74 pagesTheories of GrowthSunil CocoNo ratings yet
- Ultrasound in Obstet Gyne - 2006 - Ghi - Prenatal Diagnosis of Open and Closed Spina BifidaDocument5 pagesUltrasound in Obstet Gyne - 2006 - Ghi - Prenatal Diagnosis of Open and Closed Spina Bifidaakanksha nagarNo ratings yet
- Developmental Dysplasia of The Hip From Birth To Six MonthsDocument11 pagesDevelopmental Dysplasia of The Hip From Birth To Six MonthsRatnaNo ratings yet
- Plagiocefalia PDFDocument10 pagesPlagiocefalia PDFIlwen LlanquilefNo ratings yet
- HHS Public Access: 236 Children With Developmental Hydrocephalus: Causes and Clinical ConsequencesDocument22 pagesHHS Public Access: 236 Children With Developmental Hydrocephalus: Causes and Clinical ConsequencesPutri Rizky AmaliaNo ratings yet
- Disproporsi Kepala PanggulDocument14 pagesDisproporsi Kepala PanggulIntan PermataNo ratings yet
- Glandula Salivar HeterotopicaDocument2 pagesGlandula Salivar HeterotopicaJuan Esteban RamirezNo ratings yet
- Language and PsychosisDocument5 pagesLanguage and Psychosisvamp3461No ratings yet
- Craniofacial Syndromes.33Document26 pagesCraniofacial Syndromes.33andrew kilshawNo ratings yet
- Bies 20137Document15 pagesBies 20137Jerahmeel Sombilon GenillaNo ratings yet
- Starchild ReportDocument6 pagesStarchild ReportcismercNo ratings yet
- Examiners' Report Principal Examiner Feedback January 2018Document7 pagesExaminers' Report Principal Examiner Feedback January 2018WandaNo ratings yet
- Pile Capacity - An Overview - ScienceDirect TopicsDocument15 pagesPile Capacity - An Overview - ScienceDirect TopicssurNo ratings yet
- NEC G266 Quick Reference GuideDocument3 pagesNEC G266 Quick Reference GuideIonut Gabriel DascaluNo ratings yet
- Full TextDocument167 pagesFull Textjon minanNo ratings yet
- Evolution of Media INDUSTRIAL ERADocument16 pagesEvolution of Media INDUSTRIAL ERAAlec Ruht MasulaNo ratings yet
- Barriers of CommunicationDocument5 pagesBarriers of CommunicationIVY YBAÑEZNo ratings yet
- Alignment Technique - The Steam TurbineDocument2 pagesAlignment Technique - The Steam TurbineRajeswar KulanjiNo ratings yet
- Mech Syllabus R-2017 - 1Document110 pagesMech Syllabus R-2017 - 1goujjNo ratings yet
- B1.10 Exchanging MaterialsDocument4 pagesB1.10 Exchanging MaterialsYevonNo ratings yet
- I. You'll Hear A Conversation Between Two People. Listen and Fill in The Blanks (10 PTS) This Is The VOA Special English Agriculture ReportDocument7 pagesI. You'll Hear A Conversation Between Two People. Listen and Fill in The Blanks (10 PTS) This Is The VOA Special English Agriculture ReportTHỌ NGUYỄN VĂNNo ratings yet
- St. Louis College of Bulanao: Title/Topic Technical English I Introduction To Police Report WritingDocument41 pagesSt. Louis College of Bulanao: Title/Topic Technical English I Introduction To Police Report WritingNovelyn LumboyNo ratings yet
- Interjections NotesDocument2 pagesInterjections NotesKanna ImuiNo ratings yet
- PP in Ii 001Document15 pagesPP in Ii 001Dav EipNo ratings yet
- EED516-Assignment 1 - S1 2023Document2 pagesEED516-Assignment 1 - S1 2023RETRO GAMERSNo ratings yet
- Propositional LogicDocument41 pagesPropositional LogicMuneeb Javaid100% (1)
- Generic StructureDocument6 pagesGeneric StructureAndre AlvarezNo ratings yet
- Unit 1Document90 pagesUnit 1Atul Jaysing PatilNo ratings yet
- ENGLISH TOEFL Structure (3rd Exercise)Document5 pagesENGLISH TOEFL Structure (3rd Exercise)susannnnnnNo ratings yet
- Compressor-Less: Historical ApplicationsDocument70 pagesCompressor-Less: Historical Applicationssuryakantshrotriya100% (1)
- Module 3: Literature Review and CitationDocument3 pagesModule 3: Literature Review and CitationLysss EpssssNo ratings yet
- Power Distribution & Utilization: Total Power Generation of Last 10 Years and Forecast of 20 YearsDocument12 pagesPower Distribution & Utilization: Total Power Generation of Last 10 Years and Forecast of 20 YearsSYED ALIYYAN IMRAN ALINo ratings yet
- Anatomy & Physiology MCQsDocument26 pagesAnatomy & Physiology MCQsMuskan warisNo ratings yet
- Casio AT 1 Service ManualDocument28 pagesCasio AT 1 Service ManualMario Gabriel MoralliNo ratings yet