You might also like
- Pharmacology 1 Unit 5 Psycho Pharma Cological Agents Notes by MahendraDocument39 pagesPharmacology 1 Unit 5 Psycho Pharma Cological Agents Notes by MahendraKim Nicole Villaflores0% (1)
- Literature OCD and Related DisordersDocument23 pagesLiterature OCD and Related DisordersHana alassafNo ratings yet
- The Diagnosis of Multiple Personality DisorderDocument16 pagesThe Diagnosis of Multiple Personality DisorderChristoph HockNo ratings yet
- How Can We Use Neurotransmitters in Emotion and Reward System To Study DepressionDocument22 pagesHow Can We Use Neurotransmitters in Emotion and Reward System To Study DepressionGlobal Research and Development ServicesNo ratings yet
- Half LifeDocument43 pagesHalf LifeMinal Nadeem100% (1)
- Vision and Hearing Disorders FinalsDocument7 pagesVision and Hearing Disorders FinalsMary Reigns BuhatNo ratings yet
- Pharmaceutical Companies' InformationDocument6 pagesPharmaceutical Companies' InformationShamsher AhmedNo ratings yet
- Ethics Pract Ethical Distress Oct 2003 eDocument8 pagesEthics Pract Ethical Distress Oct 2003 eAndi FikarNo ratings yet
- Pharma CompilationDocument113 pagesPharma CompilationGulayan, Renz Bryelle T.No ratings yet
- Emergency Drugs: Drug Classification USE Stock Dose Nursing ConsiderationDocument4 pagesEmergency Drugs: Drug Classification USE Stock Dose Nursing Considerationrhennifer100% (1)
- Definitions: Sources: 2021 Lecture PPT, Comprehensive Gynecology 7 Ed Chapter 14, M. Aldana TransDocument7 pagesDefinitions: Sources: 2021 Lecture PPT, Comprehensive Gynecology 7 Ed Chapter 14, M. Aldana TransDaryl Gay NanoNo ratings yet
- (SURG) 5.4b Management of Soft Tissue SarcomaDocument6 pages(SURG) 5.4b Management of Soft Tissue SarcomaKenneth TorresNo ratings yet
- Fammed Family Life CycleDocument3 pagesFammed Family Life CycleTMC PGI GENER MICKONo ratings yet
- Adrenal Hyperfunction: Cushing'S SyndromeDocument10 pagesAdrenal Hyperfunction: Cushing'S SyndromeJoaquim RodriguezNo ratings yet
- 6.1 Skeletal SystemDocument4 pages6.1 Skeletal SystemEly FructuosoNo ratings yet
- 15 Penyakit Ulkus Peptikum (Regimen Pengobatan H.pylory)Document738 pages15 Penyakit Ulkus Peptikum (Regimen Pengobatan H.pylory)Nhoer100% (1)
- Pharmacology in Nursing and Medication AdministrationDocument170 pagesPharmacology in Nursing and Medication AdministrationskuladilzNo ratings yet
- APP-MS-047-01 B Crash Cart Checklist CAPSADocument3 pagesAPP-MS-047-01 B Crash Cart Checklist CAPSASam Alrabigi100% (1)
- Biomedical Sciences Content 2014Document3 pagesBiomedical Sciences Content 2014Bhavesh Nidhi0% (2)
- The Healing Power of Eros 1522 4821 17 144Document6 pagesThe Healing Power of Eros 1522 4821 17 144Harsh saxenaNo ratings yet
- Micro Microbial Mechanisms of Pathogenicity NOTESDocument6 pagesMicro Microbial Mechanisms of Pathogenicity NOTESAriane NobleNo ratings yet
- معايير سباهيDocument28 pagesمعايير سباهيAnonymous hF5zAdvwCCNo ratings yet
- Analyzing Urinalysis ComponentsDocument7 pagesAnalyzing Urinalysis ComponentsDee GeeNo ratings yet
- Supportive, Palliative Care & Survivorship in Prostate Cancer ICI April 2022 ZADocument39 pagesSupportive, Palliative Care & Survivorship in Prostate Cancer ICI April 2022 ZAMichaelNo ratings yet
- 5 Steps: Medical Care Decision Making For Families and Guardians. July 2013Document2 pages5 Steps: Medical Care Decision Making For Families and Guardians. July 2013Dr Jerome MellorNo ratings yet
- M.10B Drugs Used in Gastrointestinal DisordersDocument3 pagesM.10B Drugs Used in Gastrointestinal DisordersDasha VeeNo ratings yet
- Concept Map Aplastic Anemia 212 1Document1 pageConcept Map Aplastic Anemia 212 1S AustinNo ratings yet
- PEDIATRIC SURGERY - A Comprehensive Textbook For africa.-SPRINGER NATURE (2019) - 631-827Document197 pagesPEDIATRIC SURGERY - A Comprehensive Textbook For africa.-SPRINGER NATURE (2019) - 631-827adhytiyani putriNo ratings yet
- CONNECTIVE TISSUE LEC WEEK 4Document5 pagesCONNECTIVE TISSUE LEC WEEK 4Abigrael TangcoNo ratings yet
- Geriatric Nursing: Theories of AgingDocument4 pagesGeriatric Nursing: Theories of AgingNikkaDablioNo ratings yet
- Collaborative Care Clinical Manifestations: Concept MapDocument3 pagesCollaborative Care Clinical Manifestations: Concept MapMaica LectanaNo ratings yet
- Primary Skin Lesions GuideDocument39 pagesPrimary Skin Lesions GuideJorelle MarquezNo ratings yet
- 1A Non ChordataDocument62 pages1A Non ChordataDeepak ThakurNo ratings yet
- Bacteria-Borne Diseases Handout 2022Document3 pagesBacteria-Borne Diseases Handout 2022Anna CrisNo ratings yet
- Finals Week 10Document8 pagesFinals Week 10MARIE NELLIE MOSTRADONo ratings yet
- Injectable FormulationsDocument40 pagesInjectable FormulationsAutumn WishNo ratings yet
- OS 214 - Renal Module - Imaging of The KUBDocument9 pagesOS 214 - Renal Module - Imaging of The KUB2012No ratings yet
- First Aid: Dr. Dipika ShahDocument47 pagesFirst Aid: Dr. Dipika ShahDr. Niyati PatelNo ratings yet
- Medical Surgical Nursing Module 19Document4 pagesMedical Surgical Nursing Module 19weissNo ratings yet
- Topical Gels As Drug Delivery System A Comprehensive ReviewDocument7 pagesTopical Gels As Drug Delivery System A Comprehensive ReviewEditor IJTSRDNo ratings yet
- Psych ReportDocument80 pagesPsych ReportPaul Carlo GonzalesNo ratings yet
- Ent Diseases of The Oral and Pharynx Dr. UyDocument7 pagesEnt Diseases of The Oral and Pharynx Dr. UyAileen EmyNo ratings yet
- Drug Addiction As A Pathology of Staged NeuroplasticityDocument15 pagesDrug Addiction As A Pathology of Staged NeuroplasticityPamGarcíaNo ratings yet
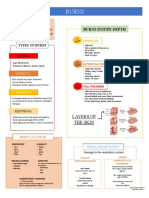
- BurnsDocument3 pagesBurnsCerezo, Cherrieus Ann C.No ratings yet
- Oncology Outpatient Provider Note 02-02-2023Document5 pagesOncology Outpatient Provider Note 02-02-2023Randell ManjarresNo ratings yet
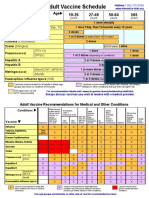
- Adult Vaccine Schedule Eng PDFDocument2 pagesAdult Vaccine Schedule Eng PDFAbdur RehmanNo ratings yet
- Nervous System DrugsDocument21 pagesNervous System Drugsemma rose lutellaNo ratings yet
- Drugs and Substance AbuseDocument68 pagesDrugs and Substance AbuseIano IanoNo ratings yet
- Week 4 - Pharma LecDocument11 pagesWeek 4 - Pharma LecJayla MarieNo ratings yet
- Pharmacology Transes - Unit 1Document13 pagesPharmacology Transes - Unit 1venturaphoenixNo ratings yet
- Week 2 - Drugs and The BodyDocument18 pagesWeek 2 - Drugs and The BodyDino MicaNo ratings yet
- 2 Areas of PharmacologyDocument3 pages2 Areas of PharmacologyAdiel CalsaNo ratings yet
- Drug Absorption, Distribution, and First-Pass EliminationDocument60 pagesDrug Absorption, Distribution, and First-Pass EliminationRuqayya AdamuNo ratings yet
- (1M) TO Pharmacology: Al-Hamad, Rawan CDocument7 pages(1M) TO Pharmacology: Al-Hamad, Rawan CLowell Jay Narciso LimosneroNo ratings yet
- Pharmacokinetics and Drug Disposition ExplainedDocument15 pagesPharmacokinetics and Drug Disposition Explainedsachin kumarNo ratings yet
- Pharmacology Terminology GuideDocument81 pagesPharmacology Terminology GuideGrazzie BearbitchNo ratings yet
- Pharmacokinetics: Drug Absorption, Distribution, Metabolism and EliminationDocument25 pagesPharmacokinetics: Drug Absorption, Distribution, Metabolism and EliminationYoshiNo ratings yet
- Introduction To Pharmacology, 10 R's To Drugs, Nursing ProcessDocument16 pagesIntroduction To Pharmacology, 10 R's To Drugs, Nursing ProcessJasmin AdoraNo ratings yet
- Pharmacokinetics: Biological MembraneDocument18 pagesPharmacokinetics: Biological MembraneRahul PalsNo ratings yet
- Pharma Rebyu MDDocument7 pagesPharma Rebyu MDseanne kskwkwkaNo ratings yet
- PHARMACOLOGY (1)Document9 pagesPHARMACOLOGY (1)aliyahalexie6No ratings yet
- Oral Drug Absorption Factors and ClassificationDocument11 pagesOral Drug Absorption Factors and ClassificationClarilaine JavierNo ratings yet
- NCM 106 Drugs and The BodyDocument46 pagesNCM 106 Drugs and The BodyYra JhaneNo ratings yet
- Pharmacokinetics: What The Body Does To A DrugDocument108 pagesPharmacokinetics: What The Body Does To A Drugallen tdlNo ratings yet
- AbsorptionDocument61 pagesAbsorptionGreenNo ratings yet
- BiopharmaceuticsDocument9 pagesBiopharmaceuticsAbigail OreelNo ratings yet
- Congenital hypothyroidism and amino acid metabolism disorders in newbornsDocument15 pagesCongenital hypothyroidism and amino acid metabolism disorders in newbornsErika Mae Deleña MarcoNo ratings yet
- Dizon BSN 2 A Activity 8 Local History and Cultural HeritageDocument3 pagesDizon BSN 2 A Activity 8 Local History and Cultural HeritageErika Mae Deleña MarcoNo ratings yet
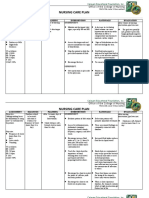
- NCP - MedicinewardDocument3 pagesNCP - MedicinewardErika Mae Deleña MarcoNo ratings yet
- Drug Study - Spirulina and VcoDocument2 pagesDrug Study - Spirulina and VcoErika Mae Deleña MarcoNo ratings yet
- Pedia Ward Templates 2Document2 pagesPedia Ward Templates 2Erika Mae Deleña MarcoNo ratings yet
- Medication CardDocument2 pagesMedication CardErika Mae Deleña MarcoNo ratings yet
- Novel Antiangiogenic Agents: Current Clinical Development: George W. Sledge, Jr. MD Indiana University Cancer CenterDocument27 pagesNovel Antiangiogenic Agents: Current Clinical Development: George W. Sledge, Jr. MD Indiana University Cancer CenterHaidir MuhammadNo ratings yet
- Adult Cardiac Arrest Circular Algorithm: Monitor CPR QualityDocument1 pageAdult Cardiac Arrest Circular Algorithm: Monitor CPR QualityAlexis HospitalNo ratings yet
- Medical BillDocument1 pageMedical BillRitik Raj SinghNo ratings yet
- Apteka - Participants - Profile1Document26 pagesApteka - Participants - Profile1Gurukrushna PatnaikNo ratings yet
- Services of Meher Pharma InternationalDocument1 pageServices of Meher Pharma InternationalMohammad Shahbaz AlamNo ratings yet
- Drug StudyDocument8 pagesDrug StudyAysaaa DCNo ratings yet
- Pain Management in Thoracic Surgery2 Dr. Ngurah Rai ArtikaDocument2 pagesPain Management in Thoracic Surgery2 Dr. Ngurah Rai ArtikajacksonmpNo ratings yet
- Bridging For Patients On DOACs/NOACsDocument1 pageBridging For Patients On DOACs/NOACsZieshNo ratings yet
- Diabetes Mellitus With Peripheral Neuropathy: Presented By: Amol LavateDocument12 pagesDiabetes Mellitus With Peripheral Neuropathy: Presented By: Amol Lavatelavate amol bhimraoNo ratings yet
- Discharge Counseling Evaluation Done by Pharmacist at Dr. Cipto Mangunkusumo National Central Public Hospital General Hospital JakartaDocument6 pagesDischarge Counseling Evaluation Done by Pharmacist at Dr. Cipto Mangunkusumo National Central Public Hospital General Hospital JakartaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Effect of Dexmedetomidine On Perioperative Hemodynamics in Patients Undergoing CraniotomyDocument8 pagesThe Effect of Dexmedetomidine On Perioperative Hemodynamics in Patients Undergoing Craniotomysrc085No ratings yet
- Ipmr AbbreviationsDocument2 pagesIpmr Abbreviationsapi-258242054No ratings yet
- Adrenergic Receptor AntagonistsDocument9 pagesAdrenergic Receptor AntagonistsPatterson MachariaNo ratings yet
- English For Nursing 2: Vocational English Teacher's BookDocument15 pagesEnglish For Nursing 2: Vocational English Teacher's BookSelina Nguyễn VuNo ratings yet
- Advanced 1 Workbook Unit 7Document10 pagesAdvanced 1 Workbook Unit 7daniela almendaresNo ratings yet
- 1658725996421Document43 pages1658725996421aniket singh100% (1)
- AI MCQ Pharma (Lec1)Document8 pagesAI MCQ Pharma (Lec1)raneemalnaamnehNo ratings yet
- Cognitive Analytic Therapy - 13 Oct 2015Document36 pagesCognitive Analytic Therapy - 13 Oct 2015aliyaban.filesNo ratings yet
- 429-743-1-SM (2) OJS Hermanto Jurnal Metris Unika AtmaJaya Jakarta PDFDocument8 pages429-743-1-SM (2) OJS Hermanto Jurnal Metris Unika AtmaJaya Jakarta PDFHermanto RuslanNo ratings yet
- Assessing Pain: Maria Criselda Reicelle Q. Avelino, MAN, RNDocument38 pagesAssessing Pain: Maria Criselda Reicelle Q. Avelino, MAN, RNAbcd TolibasNo ratings yet
- University of Asia Pacific Admission Test For Fall 2019Document1 pageUniversity of Asia Pacific Admission Test For Fall 2019JeasonNo ratings yet
- TX To OTC Switch LIst - USDocument6 pagesTX To OTC Switch LIst - USSudeep BhattacharyyaNo ratings yet
- Kci Vac Therapy Vtiaf UpdatedDocument2 pagesKci Vac Therapy Vtiaf UpdatedHi BeyoNo ratings yet
- OM For Empanelment of Ayurvedic, Yoga and Naturopathy Day Care Centers Under CGHS (20 Nov 2020)Document5 pagesOM For Empanelment of Ayurvedic, Yoga and Naturopathy Day Care Centers Under CGHS (20 Nov 2020)mechsrinuNo ratings yet