You might also like
- Case Report Surgical Management of Lumbal Compression FractureDocument8 pagesCase Report Surgical Management of Lumbal Compression FractureYustinusrobbyNo ratings yet
- Pedicle Screw Fixation in Fracture of Thoraco-Lumbar SpineDocument21 pagesPedicle Screw Fixation in Fracture of Thoraco-Lumbar SpineNiyati SharmaNo ratings yet
- Median and Anterior Interosseous Nerve Entrapment Syndromes Versus Carpal Tunnel Syndrome: A Study of Two CasesDocument10 pagesMedian and Anterior Interosseous Nerve Entrapment Syndromes Versus Carpal Tunnel Syndrome: A Study of Two CasesNazia SalmanNo ratings yet
- Nasional 3 NIC:KOE Penetrating Cervial Spine Injury ENDocument6 pagesNasional 3 NIC:KOE Penetrating Cervial Spine Injury ENHeru Sutanto KNo ratings yet
- Talar Body Fracture Case in 10-Year-Old BoyDocument6 pagesTalar Body Fracture Case in 10-Year-Old BoyPoliceNo ratings yet
- Case Report Traumatic Fracture: Dislocation of Cervicothoracic Junction - Grand Round Presentation of C7-T1 Instabilities and Different Instrumentation TechniquesDocument6 pagesCase Report Traumatic Fracture: Dislocation of Cervicothoracic Junction - Grand Round Presentation of C7-T1 Instabilities and Different Instrumentation TechniquesMohammad Al-SofyaniNo ratings yet
- Cervical spine fractures treatment by triple vertebral body removalDocument5 pagesCervical spine fractures treatment by triple vertebral body removalalejandraNo ratings yet
- Spinal Cord Compression Due To Undiagnosed Thoracic Meningioma Following Lumbar Surgery in An Elderly Patient: A CaseDocument4 pagesSpinal Cord Compression Due To Undiagnosed Thoracic Meningioma Following Lumbar Surgery in An Elderly Patient: A CaseLuwiNo ratings yet
- Brief Resume of Intended WorkDocument7 pagesBrief Resume of Intended WorkNavin ChandarNo ratings yet
- Radial Nerve Entrapment in A Humeral Fracture Callus: Case ReportDocument4 pagesRadial Nerve Entrapment in A Humeral Fracture Callus: Case ReportMuhammad RezaNo ratings yet
- BJBJ Spine Injury Without Rad AbnormalityDocument4 pagesBJBJ Spine Injury Without Rad Abnormalitymelanie97No ratings yet
- Case Report Indri-Noha FIXDocument5 pagesCase Report Indri-Noha FIXIndri Pratiwi TobingNo ratings yet
- A Case of Eccrine Tumour Metastasis To Spine Managed With Posterior Spinal Stabilization With Recovering ParaparesisDocument3 pagesA Case of Eccrine Tumour Metastasis To Spine Managed With Posterior Spinal Stabilization With Recovering ParaparesisInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Closed Intra - Articular Fractures of The Distal End of Humerus Surgically Treated by Trans - Olecranon Approach Using The Chevron OsteotomyDocument4 pagesClosed Intra - Articular Fractures of The Distal End of Humerus Surgically Treated by Trans - Olecranon Approach Using The Chevron OsteotomyIJAR JOURNALNo ratings yet
- Unstable Burst Fractures of The Thoraco-Lumbar Junction TreatmentDocument8 pagesUnstable Burst Fractures of The Thoraco-Lumbar Junction TreatmentRafael Jardim de MouraNo ratings yet
- Spinal Tuberculosis: Imaging Features On MRIDocument6 pagesSpinal Tuberculosis: Imaging Features On MRIEster JuanitaNo ratings yet
- Atraumatic Cuff TearsDocument7 pagesAtraumatic Cuff Tearschandan noelNo ratings yet
- Journal Neurosurgery SpineDocument3 pagesJournal Neurosurgery SpineWidi Nugraha HadianNo ratings yet
- Com Minuted Patellar FractureDocument3 pagesCom Minuted Patellar FractureAhmet EkinciNo ratings yet
- Arthroscopic Bursectomy For Recalcitrant Trochanteric BursitisDocument6 pagesArthroscopic Bursectomy For Recalcitrant Trochanteric BursitisGökhan PehlivanoğluNo ratings yet
- Jain Extrapleural ApproachDocument5 pagesJain Extrapleural ApproachOj AlimbuyuguenNo ratings yet
- Anterior Deltopectoral ApproachDocument5 pagesAnterior Deltopectoral ApproachNetravathi EllurNo ratings yet
- Dystrophic Scoliosis and Rib Resection Case ReportDocument8 pagesDystrophic Scoliosis and Rib Resection Case Reportdadakan16No ratings yet
- ptrs009 03 03 PDFDocument6 pagesptrs009 03 03 PDFGusti Ayu KrisnayantiNo ratings yet
- Complications of Temporomandibular Joint Arthroscopy: A Retrospective Analytic Study of 670 Arthroscopic ProceduresDocument5 pagesComplications of Temporomandibular Joint Arthroscopy: A Retrospective Analytic Study of 670 Arthroscopic ProceduresAbhishek SinghNo ratings yet
- Edh PDFDocument4 pagesEdh PDFRiska Rahmawati PratAmaNo ratings yet
- Floating ElbowDocument5 pagesFloating ElbowpepitomuraNo ratings yet
- Jurnal SkoliosisDocument9 pagesJurnal SkoliosisLidya SiahaanNo ratings yet
- A Case of Symptomatic Multiple Tarlov Cysts Treated WithDocument6 pagesA Case of Symptomatic Multiple Tarlov Cysts Treated Withjabarin.hNo ratings yet
- Giacalone 2015Document7 pagesGiacalone 2015Joseval FilhoNo ratings yet
- J Neurol Sci (Turk)Document9 pagesJ Neurol Sci (Turk)nulaeli Siti ANo ratings yet
- Evaluating Intervertebral Foramen MeasurDocument7 pagesEvaluating Intervertebral Foramen MeasurrecepNo ratings yet
- Medi 95 E2797Document3 pagesMedi 95 E2797Rui Pedro PereiraNo ratings yet
- Short Versus Long Outcome RadiologisDocument7 pagesShort Versus Long Outcome Radiologisandy ardiansyahNo ratings yet
- Complications and Outcomes of The Transfibular Approach For Posterolateral Fractures of The Tibial Plateau PDFDocument19 pagesComplications and Outcomes of The Transfibular Approach For Posterolateral Fractures of The Tibial Plateau PDFSergio Tomas Cortés MoralesNo ratings yet
- Case Series of All-Arthroscopic Treatment For Terrible Triad of The Elbow: Indications and Clinical OutcomesDocument10 pagesCase Series of All-Arthroscopic Treatment For Terrible Triad of The Elbow: Indications and Clinical OutcomesdorfynatorNo ratings yet
- Case Report Rehabilitation Program in A Patient With Fracture of The Distal FemurDocument26 pagesCase Report Rehabilitation Program in A Patient With Fracture of The Distal FemurNatalia LoredanaNo ratings yet
- Knee Synovial Osteochorndromatosis: Case Report, Saudi ArabiaDocument4 pagesKnee Synovial Osteochorndromatosis: Case Report, Saudi ArabiaIJAR JOURNALNo ratings yet
- Aaos 2010Document220 pagesAaos 2010Yusufa ArdyNo ratings yet
- 460 FullDocument7 pages460 FullNasrull BinHzNo ratings yet
- Hangmans Fracture and Its ManagementDocument1 pageHangmans Fracture and Its ManagementPeko PekoNo ratings yet
- Art3a10 10072fs00256-014-1842-5Document9 pagesArt3a10 10072fs00256-014-1842-5api-253958760No ratings yet
- Effect of Ultrasound Image-Guided Nerve BlockDocument9 pagesEffect of Ultrasound Image-Guided Nerve BlockMarce SiuNo ratings yet
- Elbow Study 1Document8 pagesElbow Study 1Prashant SurtiNo ratings yet
- hemu-SPG PaperDocument5 pageshemu-SPG Papernayem hossainNo ratings yet
- White Cord Syndrome After Cervical DecompressionDocument7 pagesWhite Cord Syndrome After Cervical DecompressionJosé A. RodríguezNo ratings yet
- Falling From The Tightrope: Double Versus Single Tightropes in Patients With Acromioclavicular Joint Dislocations: Technique and ComplicationsDocument6 pagesFalling From The Tightrope: Double Versus Single Tightropes in Patients With Acromioclavicular Joint Dislocations: Technique and ComplicationsChrysi TsiouriNo ratings yet
- Wang JL Qiw Liu Yj: Author InformationDocument11 pagesWang JL Qiw Liu Yj: Author InformationVladFelecanNo ratings yet
- Examination AAOS 2009 SpineDocument56 pagesExamination AAOS 2009 SpineJulieta PereyraNo ratings yet
- 9 Suppl - 1 S58Document7 pages9 Suppl - 1 S58ChristopherLawrenceNo ratings yet
- Anterior Cervicothoracic Corpectomy Via Cervical ApproachDocument6 pagesAnterior Cervicothoracic Corpectomy Via Cervical ApproachSadashivayya SoppimathNo ratings yet
- Svoa Ne 02 020Document10 pagesSvoa Ne 02 020Trina ViskhawatNo ratings yet
- Intramedullary K-Wire Fixation of Metacarpal Fractures: Georg Kelsch Christoph UlrichDocument4 pagesIntramedullary K-Wire Fixation of Metacarpal Fractures: Georg Kelsch Christoph UlrichVolcNo ratings yet
- Surgery of the Cranio-Vertebral JunctionFrom EverandSurgery of the Cranio-Vertebral JunctionEnrico TessitoreNo ratings yet
- MontotenniselbowDocument7 pagesMontotenniselbowPURVA THAKURNo ratings yet
- Caekebeke 2016 JSES Distal Biceps Tendon Repair Comparison of ClinicalDocument6 pagesCaekebeke 2016 JSES Distal Biceps Tendon Repair Comparison of ClinicalKuozram No MasNo ratings yet
- A Study On Management of Bothbones Forearm Fractures With Dynamic Compression PlateDocument5 pagesA Study On Management of Bothbones Forearm Fractures With Dynamic Compression PlateIOSRjournalNo ratings yet
- MUSCULOSKELETAL TRAUMA SELF-ASSESSMENT EXAMDocument10 pagesMUSCULOSKELETAL TRAUMA SELF-ASSESSMENT EXAMAndika Adiputra ThehumuryNo ratings yet
- Abordaje CombinadoDocument5 pagesAbordaje CombinadoJulia LemboNo ratings yet
- Sinking Skin Flap Syndrome Following Decompressive Craniectomy For Acute Subdural Hemorrhage FinalDocument7 pagesSinking Skin Flap Syndrome Following Decompressive Craniectomy For Acute Subdural Hemorrhage Finalbosnia agusNo ratings yet
- DAFTAR PASIEN BEDAH SARAFDocument2 pagesDAFTAR PASIEN BEDAH SARAFbosnia agusNo ratings yet
- Sacral FractureDocument21 pagesSacral Fracturebosnia agusNo ratings yet
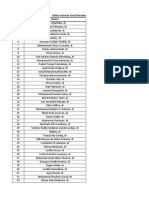
- Daftar Alamat Email Residen + NPM NC 2020Document4 pagesDaftar Alamat Email Residen + NPM NC 2020bosnia agusNo ratings yet
- BN NRDocument51 pagesBN NRbosnia agusNo ratings yet
- Neurosurgery Report: Head Injury and Cervical Fracture CasesDocument49 pagesNeurosurgery Report: Head Injury and Cervical Fracture Casesbosnia agusNo ratings yet
- Pasien Poli Kamis, 08 Desember 2022Document1 pagePasien Poli Kamis, 08 Desember 2022bosnia agusNo ratings yet
- Anterior Odontoid Screw FixationDocument22 pagesAnterior Odontoid Screw Fixationbosnia agusNo ratings yet
- ISMT12 - Day 176 - Sheila - Diseases of Gray MatterDocument16 pagesISMT12 - Day 176 - Sheila - Diseases of Gray Matterbosnia agusNo ratings yet
- Vascular pathologies of the spinal cordDocument22 pagesVascular pathologies of the spinal cordbosnia agusNo ratings yet
- STROBE Checklist Cross-SectionalDocument2 pagesSTROBE Checklist Cross-SectionalAmalia Riska G100% (1)
- ISMT12 - Day 169 - Sheila - Spinal MeningitisDocument14 pagesISMT12 - Day 169 - Sheila - Spinal Meningitisbosnia agusNo ratings yet
- ISMT12 - Day 192 - Fardhian - Lateral Retroperitoneal Approach To The Lumbar SpineDocument28 pagesISMT12 - Day 192 - Fardhian - Lateral Retroperitoneal Approach To The Lumbar Spinebosnia agusNo ratings yet
- Fibrin Clot Formation and Lysis: Basic Mechanisms: Seminars in Thrombosis and Hemostasis February 2000Document15 pagesFibrin Clot Formation and Lysis: Basic Mechanisms: Seminars in Thrombosis and Hemostasis February 2000bosnia agusNo ratings yet
- ISMT12 - Day 112 - Fardhian - Physical and Neurologic ExaminationDocument26 pagesISMT12 - Day 112 - Fardhian - Physical and Neurologic Examinationbosnia agusNo ratings yet
- A Novel Technique To Correct Kyphosis in Cervical Posterior Longitudinal LigamentDocument6 pagesA Novel Technique To Correct Kyphosis in Cervical Posterior Longitudinal Ligamentbosnia agusNo ratings yet
- Case Trauma: Yulius HermantoDocument17 pagesCase Trauma: Yulius Hermantobosnia agusNo ratings yet
- ISMT12 - Day 112 - Sheila - Case Infection Acute Communicating Hydrocephalus Due To Tuberculous MeningitisDocument29 pagesISMT12 - Day 112 - Sheila - Case Infection Acute Communicating Hydrocephalus Due To Tuberculous Meningitisbosnia agusNo ratings yet
- Update Pasien NC 25 April 2021 Untuk KonsulenDocument2 pagesUpdate Pasien NC 25 April 2021 Untuk Konsulenbosnia agusNo ratings yet
- Tumors of SpineDocument13 pagesTumors of Spinebosnia agusNo ratings yet
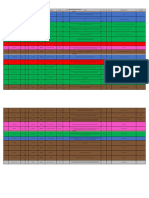
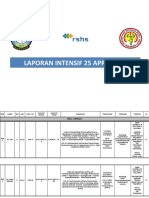
- Laporan Intensif 25 April 2021Document21 pagesLaporan Intensif 25 April 2021bosnia agusNo ratings yet
- Update Pasien Bedah Saraf 25 April 2021Document2 pagesUpdate Pasien Bedah Saraf 25 April 2021bosnia agusNo ratings yet
- Update Pasien NC 05 Maret 2021 Untuk KonsulenDocument1 pageUpdate Pasien NC 05 Maret 2021 Untuk Konsulenbosnia agusNo ratings yet
- List Laptop Kisaran 7 JutaDocument5 pagesList Laptop Kisaran 7 Jutabosnia agusNo ratings yet
- Update Pasien NC 30 Maret 2021 Per DPJPDocument2 pagesUpdate Pasien NC 30 Maret 2021 Per DPJPbosnia agusNo ratings yet
- Spinal Shock: By: DR Ismah, Ortho DepartmentDocument16 pagesSpinal Shock: By: DR Ismah, Ortho Departmentbosnia agusNo ratings yet
- Update Pasien NC 25 April 2021 Untuk KonsulenDocument2 pagesUpdate Pasien NC 25 April 2021 Untuk Konsulenbosnia agusNo ratings yet
- Siegel 2017Document8 pagesSiegel 2017bosnia agusNo ratings yet
- Spinal Shock.Document12 pagesSpinal Shock.bosnia agusNo ratings yet
- Instant Download Ebook PDF Basic Pharmacology For Nurses 17th Edition PDF ScribdDocument41 pagesInstant Download Ebook PDF Basic Pharmacology For Nurses 17th Edition PDF Scribdcicely.smith712100% (38)
- Correlation Between Neonatal Hyperbilirubinemia and Vitamin D Levels: A Meta-AnalysisDocument12 pagesCorrelation Between Neonatal Hyperbilirubinemia and Vitamin D Levels: A Meta-AnalysisAbdurrahman HasanuddinNo ratings yet
- Essential Oils and Low-Intensity Electromagnetic Pulses in The Treatment of Androgen-Dependent AlopeciaDocument10 pagesEssential Oils and Low-Intensity Electromagnetic Pulses in The Treatment of Androgen-Dependent AlopeciaHuman ResourcesNo ratings yet
- Klinik Panel PrubsnDocument24 pagesKlinik Panel PrubsnAflah JamaluddinNo ratings yet
- TaurodontDocument14 pagesTaurodontHameed WaseemNo ratings yet
- Enfermedades Proyecto InglesDocument3 pagesEnfermedades Proyecto Inglesyanis7116No ratings yet
- Nebulization TherapyDocument2 pagesNebulization TherapySamantha Nicole MendozaNo ratings yet
- Emergency Assistance Plan by TW 12oct21Document7 pagesEmergency Assistance Plan by TW 12oct21Than WinNo ratings yet
- Cebu Institute of Technology - University: Nursing Care PlanDocument2 pagesCebu Institute of Technology - University: Nursing Care PlanSergiNo ratings yet
- Bilirubin Kit PDFDocument2 pagesBilirubin Kit PDFArasNo ratings yet
- Understand The Facts - Anxiety and Depression Association of America, ADAADocument5 pagesUnderstand The Facts - Anxiety and Depression Association of America, ADAAAhmad Badius ZamanNo ratings yet
- 2A - Zahirah Rahmadian Budiman - PROBLEMS WITH PAINDocument5 pages2A - Zahirah Rahmadian Budiman - PROBLEMS WITH PAINZahirah BudimanNo ratings yet
- Placental AbnormalitiesDocument3 pagesPlacental AbnormalitiesThakoon TtsNo ratings yet
- Fenotipos de BronquiolitisDocument14 pagesFenotipos de BronquiolitisJohann MuñozNo ratings yet
- Microbiology and ParasitologyDocument9 pagesMicrobiology and ParasitologyDefensor Pison Gringgo0% (1)
- First Aid Skills Checklist PDFDocument2 pagesFirst Aid Skills Checklist PDFSridhar Tarai100% (1)
- Four Immune-Supporting Supplements in Lyme DiseaseDocument11 pagesFour Immune-Supporting Supplements in Lyme Diseaseflorinko100% (1)
- Carcinoma of Prostate: Patho Ogy - Chapter &Document29 pagesCarcinoma of Prostate: Patho Ogy - Chapter &HAMIDNo ratings yet
- File - 20190927 - 153306 - Drugs Reaction 2019Document410 pagesFile - 20190927 - 153306 - Drugs Reaction 2019ntnquynhpro100% (1)
- Complete Ophtho VM555 CoursepackDocument189 pagesComplete Ophtho VM555 Coursepacknandhus2227No ratings yet
- Venepuncture in Adults: Take A Blood Sample Using Vacuum Collection TubesDocument4 pagesVenepuncture in Adults: Take A Blood Sample Using Vacuum Collection TubesimaguestuserNo ratings yet
- Pregnancy Induced Hypertension (Pih)Document56 pagesPregnancy Induced Hypertension (Pih)shandi23100% (5)
- 5-12th Bio Chap 17 Coordination & Control (B)Document2 pages5-12th Bio Chap 17 Coordination & Control (B)Raees Ali KhanNo ratings yet
- Urinary Bladder MassDocument2 pagesUrinary Bladder Masskarl de guzmanNo ratings yet
- Dimorphic Systemic MycosesDocument65 pagesDimorphic Systemic Mycoseskedar karkiNo ratings yet
- Urinalysis: Clin. Immunol. / Lab. Work/ Renal Disorders/ Urine Analysis/ Dr. Batool Al-HaidaryDocument11 pagesUrinalysis: Clin. Immunol. / Lab. Work/ Renal Disorders/ Urine Analysis/ Dr. Batool Al-HaidaryIM CTNo ratings yet
- 10 Mcqs Canada For SampleDocument5 pages10 Mcqs Canada For SampleNavjot BrarNo ratings yet
- Recommended Immunization - Canadian Immunization Guide - Seventh Edition - 2006Document2 pagesRecommended Immunization - Canadian Immunization Guide - Seventh Edition - 2006Maja MudriNo ratings yet
- Comprehensive Index to Find Musculoskeletal ConditionsDocument16 pagesComprehensive Index to Find Musculoskeletal ConditionsMustafa Ali0% (1)
- (Answer Key) Written Competency ReticulocytesDocument25 pages(Answer Key) Written Competency ReticulocytessaharNo ratings yet