You might also like
- RAC Exams QuestionsDocument14 pagesRAC Exams QuestionsExamsure975% (4)
- Quality Control ChecklistDocument3 pagesQuality Control Checklistsheila marie canibasNo ratings yet
- Question BankDocument5 pagesQuestion BankUmesh ChikhlikarNo ratings yet
- Critical Aspect Analytical Test Review: Jakarta 14 December 2017 Speaker: Heru Purnomo, STDocument24 pagesCritical Aspect Analytical Test Review: Jakarta 14 December 2017 Speaker: Heru Purnomo, STMohammad Naufal AliefNo ratings yet
- Assessment Tool For Licensing A General Clinical LaboratoryDocument13 pagesAssessment Tool For Licensing A General Clinical LaboratorySALMAN JOHAYR100% (1)
- Comparison Bet. US FDA, USP & ICH GuidelinesDocument10 pagesComparison Bet. US FDA, USP & ICH GuidelinesRavi KantNo ratings yet
- DLL UCSP Week 6Document3 pagesDLL UCSP Week 6Andrey Cabuntocan100% (3)
- 01 Master SOP FinDocument6 pages01 Master SOP FinPramod Athiyarathu100% (1)
- New Pathology Lab PresentationDocument38 pagesNew Pathology Lab Presentationsagar hingrajiaNo ratings yet
- Class: 8 Science Chapter - 8 Cell - Structure and FunctionsDocument10 pagesClass: 8 Science Chapter - 8 Cell - Structure and FunctionsAmiteshwar SinghNo ratings yet
- Nnaca Sop 302Document6 pagesNnaca Sop 302Thusitha LakpriyaNo ratings yet
- Assessment ToolDocument13 pagesAssessment Toolal gulNo ratings yet
- Oig Method Validation Procedure 01 PDFDocument10 pagesOig Method Validation Procedure 01 PDFMargaretaSianneNo ratings yet
- Practical Approaches to Method Validation and Essential Instrument QualificationFrom EverandPractical Approaches to Method Validation and Essential Instrument QualificationNo ratings yet
- Quality Assurance QuestionnaireDocument5 pagesQuality Assurance QuestionnaireAbdelkader FattoucheNo ratings yet
- Quality Assurance Program JPH Diagnostic CenterDocument8 pagesQuality Assurance Program JPH Diagnostic CenterKathleen Rose Tuy-RefulgenteNo ratings yet
- UT Protocol API QUTE EquivelentDocument2 pagesUT Protocol API QUTE EquivelentreiazhNo ratings yet
- Application Form For For Testing Labs ISO17025Document14 pagesApplication Form For For Testing Labs ISO17025PK Jha100% (2)
- Manual de Usuario GEM 3500Document15 pagesManual de Usuario GEM 3500Andrea PerezNo ratings yet
- Laboratory Quality/Management: A Workbook with an Eye on AccreditationFrom EverandLaboratory Quality/Management: A Workbook with an Eye on AccreditationRating: 5 out of 5 stars5/5 (1)
- Depyrogenation TunnelDocument6 pagesDepyrogenation TunnelPrachi MishraNo ratings yet
- Ic Doc Form Routes 2and4 2Document1 pageIc Doc Form Routes 2and4 2مصطفي خندقاويNo ratings yet
- Imb Routes 4 and 5 WorkDocument1 pageImb Routes 4 and 5 WorksjbfhsbvNo ratings yet
- Imls 2 4 5 Work Experience Doc FormDocument3 pagesImls 2 4 5 Work Experience Doc FormRenier Joseph Dela RosaNo ratings yet
- HT Route 2 DocDocument2 pagesHT Route 2 DocbejlvwirsharklasersomNo ratings yet
- CT Clinical ExperienceDocument7 pagesCT Clinical ExperiencejlhartnessNo ratings yet
- IFIA Training Record Book English-August 2010Document10 pagesIFIA Training Record Book English-August 2010Anthony Pozo0% (1)
- Blood Gas AnalyzerDocument13 pagesBlood Gas Analyzeranon_708486566No ratings yet
- PM 7/98 (4) Specific Requirements For Laboratories Preparing Accreditation For A Plant Pest Diagnostic ActivityDocument34 pagesPM 7/98 (4) Specific Requirements For Laboratories Preparing Accreditation For A Plant Pest Diagnostic ActivityGlobal QualityNo ratings yet
- Pro64-A-03 - Processing - A - CBC - CNT - SOPDocument7 pagesPro64-A-03 - Processing - A - CBC - CNT - SOPBassam AlharaziNo ratings yet
- SOP 18.1 - Attachment A Audit Preparation ChecklistDocument3 pagesSOP 18.1 - Attachment A Audit Preparation ChecklistNIMNo ratings yet
- Procedures For Examination and Qualification: JULY 2019Document16 pagesProcedures For Examination and Qualification: JULY 2019Eunica FadriquelaNo ratings yet
- 00-V016 Quality EHS Record Control Procedure Rev 180311Document5 pages00-V016 Quality EHS Record Control Procedure Rev 180311Tuong NguyenNo ratings yet
- F401e AC6 Medical Laboratory eDocument7 pagesF401e AC6 Medical Laboratory eAhmedA.HassanNo ratings yet
- AC 2.1 V.8.2 Application Form and Accreditation AgreementDocument9 pagesAC 2.1 V.8.2 Application Form and Accreditation AgreementAnonymous cP2LRltNo ratings yet
- Template of Cleaning Validation ProtocolDocument7 pagesTemplate of Cleaning Validation Protocol王仁宏No ratings yet
- Clinical ChemistryDocument4 pagesClinical ChemistryMary CabalceNo ratings yet
- ABRET Examination PoliciesDocument39 pagesABRET Examination PoliciesDiana CarolinaNo ratings yet
- Quality Management System Procedure: (Laboratory Name)Document3 pagesQuality Management System Procedure: (Laboratory Name)jeric bañaderaNo ratings yet
- STR 2.4 - Specific Technical Requirements For Accreditation of Haematology LaboratoriesDocument16 pagesSTR 2.4 - Specific Technical Requirements For Accreditation of Haematology LaboratoriesTauke SengNo ratings yet
- QP 04Document15 pagesQP 04zakwanmustafaNo ratings yet
- 71 SD 0 010 e Proficiency Tests 20140414 v1.2Document9 pages71 SD 0 010 e Proficiency Tests 20140414 v1.2Royal BimhahNo ratings yet
- RPT ApplicationDocument7 pagesRPT ApplicationEdNo ratings yet
- Question for Training with AnswerDocument4 pagesQuestion for Training with AnswerZETTYNo ratings yet
- Post Analytical Best Practices: Labs For Life PPT SeriesDocument48 pagesPost Analytical Best Practices: Labs For Life PPT SeriesSaravnan RajendranNo ratings yet
- NABL 151 - Application Form For Testing LaboratoriesDocument14 pagesNABL 151 - Application Form For Testing Laboratorieszilangamba_s4535No ratings yet
- Cobas e 411Document2 pagesCobas e 411Santos CruzNo ratings yet
- Pharmaceutical Preformulation and FormulationDocument10 pagesPharmaceutical Preformulation and FormulationPrashansa ShresthaNo ratings yet
- 2023 Self-Assessment Guidance For Candidates PDFDocument18 pages2023 Self-Assessment Guidance For Candidates PDFCNo ratings yet
- Purchasing and ReceiptDocument7 pagesPurchasing and ReceiptOsman AitaNo ratings yet
- Rapid AbgDocument11 pagesRapid AbgDeoMikhailAngeloNuñezNo ratings yet
- EUROLAB Cook BookDoc No 1 Selection Verification and Validation of MethodsRev 2017Document3 pagesEUROLAB Cook BookDoc No 1 Selection Verification and Validation of MethodsRev 2017nedkovbgNo ratings yet
- Unit 14 Quality Assurance in The Transfusion Service: Terry Kotrla, MS, MT (ASCP) BBDocument35 pagesUnit 14 Quality Assurance in The Transfusion Service: Terry Kotrla, MS, MT (ASCP) BBdebbie o. azcunaNo ratings yet
- Submission of Histopathology SamplesDocument4 pagesSubmission of Histopathology SamplesGarima GoelNo ratings yet
- 1 3 180 v6 Signalling Principles TesterDocument28 pages1 3 180 v6 Signalling Principles Testeravvaru.stockmarketNo ratings yet
- A Borges AccreditationDocument23 pagesA Borges AccreditationcandiddreamsNo ratings yet
- CookBook 01 Selection-Verification-Validation-Methods - 09-2018 PDFDocument3 pagesCookBook 01 Selection-Verification-Validation-Methods - 09-2018 PDFAzhani AlangNo ratings yet
- Presentation 1 Maham Fatima 1Document7 pagesPresentation 1 Maham Fatima 1mahamx72No ratings yet
- Pharmaceutical Process Validation - Lecture SlidesDocument19 pagesPharmaceutical Process Validation - Lecture SlidesMD Fahad MiajiNo ratings yet
- Textbook of Urgent Care Management: Chapter 31, Laboratory OverviewFrom EverandTextbook of Urgent Care Management: Chapter 31, Laboratory OverviewNo ratings yet
- AMAL SULIMAN ALFIHED-Female34 Years-221465Document1 pageAMAL SULIMAN ALFIHED-Female34 Years-221465manalNo ratings yet
- Amal Saad-Female40 Years-229847Document1 pageAmal Saad-Female40 Years-229847manalNo ratings yet
- Shooq Abdullah-Female17 Years-229834Document1 pageShooq Abdullah-Female17 Years-229834manalNo ratings yet
- MAHDI MOHD-Male28 Years-230366Document1 pageMAHDI MOHD-Male28 Years-230366manalNo ratings yet
- Khames Ali Nasser-Female60 Years-232287Document1 pageKhames Ali Nasser-Female60 Years-232287manalNo ratings yet
- Specialist Vs Generalist 2012Document10 pagesSpecialist Vs Generalist 2012Juanito FCalocaNo ratings yet
- Annelida 1Document36 pagesAnnelida 1Hescel An ButacNo ratings yet
- Biology Questions and Answers - Biomolecules - Primary and Secondary Metabolites - 1Document8 pagesBiology Questions and Answers - Biomolecules - Primary and Secondary Metabolites - 1Neharkar RaniNo ratings yet
- 1.1 Introduction To CellsDocument55 pages1.1 Introduction To Cellsralph nmeirNo ratings yet
- Summative Mednelian and NonmendelianDocument2 pagesSummative Mednelian and NonmendelianMae Uayan Prisco-TagaraoNo ratings yet
- Artigos Científicos - NeCDocument905 pagesArtigos Científicos - NeCBryan JulioNo ratings yet
- 25 Page Research PaperDocument4 pages25 Page Research Papergzrvpcvnd100% (1)
- Emotional Intelligence: What Does It Mean To Be EmotionallyDocument4 pagesEmotional Intelligence: What Does It Mean To Be EmotionallyAshley NicoleNo ratings yet
- Shivaramu Ph.D. ThesisDocument108 pagesShivaramu Ph.D. Thesisdaniel cretuNo ratings yet
- Law of The Limiting FactorsDocument4 pagesLaw of The Limiting FactorsBiswajit DarbarNo ratings yet
- Evolution ReviewDocument8 pagesEvolution Reviewn.misovicNo ratings yet
- Grade 7 Biology R01Document2 pagesGrade 7 Biology R01He NiNo ratings yet
- Shonkoff. Building A New Biodevelopment FrameworkDocument11 pagesShonkoff. Building A New Biodevelopment FrameworkRodrigo Miguel Rojas AndradeNo ratings yet
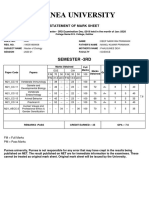
- Purnea University: Semester - 3RdDocument1 pagePurnea University: Semester - 3Rdpiyush raghavNo ratings yet
- Gramsstaining 170127105133 PDFDocument15 pagesGramsstaining 170127105133 PDFManish SoniNo ratings yet
- The Origin of Species: The Beak of The FinchDocument12 pagesThe Origin of Species: The Beak of The FinchBenedicto IluminNo ratings yet
- Unicellular and Multicellular OrganismsDocument30 pagesUnicellular and Multicellular OrganismsMishaliniNo ratings yet
- Evidence of Evolution 21-22Document13 pagesEvidence of Evolution 21-22JAMES DUDCZYKNo ratings yet
- Introduccion A La HPLC Quattrocchi PDFDocument406 pagesIntroduccion A La HPLC Quattrocchi PDFSara hidalgo marulandaNo ratings yet
- 03 Chapter 2Document37 pages03 Chapter 2Amen EyobedNo ratings yet
- SUSTAINABILITYDocument55 pagesSUSTAINABILITYAlfredo Romero100% (1)
- Biology Master Test: DT: 7 September 2014Document2 pagesBiology Master Test: DT: 7 September 2014TY OrganicNo ratings yet
- Living World Test 1Document2 pagesLiving World Test 1MRIDULANo ratings yet
- Biol 1122 Discussion Unit 4Document2 pagesBiol 1122 Discussion Unit 4Tosin JeremiahNo ratings yet
- Red Dragon Fruit As Natural DyeDocument7 pagesRed Dragon Fruit As Natural DyeKiersten GabatoNo ratings yet
- Eikon Issue5 WebDocument85 pagesEikon Issue5 WebTiffany AlexandriaNo ratings yet
- LUTHFIDocument1 pageLUTHFIbudy raharjaNo ratings yet
- Humacount 5D: - Quick GuideDocument2 pagesHumacount 5D: - Quick GuideMohamed ZinaNo ratings yet