You might also like
- Textbook of Urgent Care Management: Chapter 35, Urgent Care Imaging and InterpretationFrom EverandTextbook of Urgent Care Management: Chapter 35, Urgent Care Imaging and InterpretationNo ratings yet
- Paper 358Document8 pagesPaper 358PRATEEK SARKARNo ratings yet
- LED-Based Photoacoustic Imaging: From Bench to BedsideFrom EverandLED-Based Photoacoustic Imaging: From Bench to BedsideMithun Kuniyil Ajith SinghNo ratings yet
- RESPIRE: A Spectral Kurtosis-Based Method To Extract Respiration Rate From Wearable PPG SignalsDocument6 pagesRESPIRE: A Spectral Kurtosis-Based Method To Extract Respiration Rate From Wearable PPG SignalsMariana Córdoba HolguínNo ratings yet
- Robust Design of Pulse Oximeter Using Dynamic Control and Motion Artifact Detection AlgorithmsDocument8 pagesRobust Design of Pulse Oximeter Using Dynamic Control and Motion Artifact Detection AlgorithmsGil Won YoonNo ratings yet
- The Physics and Technology of Diagnostic Ultrasound: Study Guide (Second Edition)From EverandThe Physics and Technology of Diagnostic Ultrasound: Study Guide (Second Edition)No ratings yet
- 2616-Article Text-4940-1-10-20210416Document5 pages2616-Article Text-4940-1-10-20210416maxor4242No ratings yet
- Electronics 03 00282 - MdpiDocument21 pagesElectronics 03 00282 - MdpiKarthigaMurugesanNo ratings yet
- Preprints201810 0578 v1Document18 pagesPreprints201810 0578 v1mahsa sherbafiNo ratings yet
- A Clip-Free Eyeglasses-Based Wearable Monitoring Device For Measuring Photoplethysmograhic SignalsDocument4 pagesA Clip-Free Eyeglasses-Based Wearable Monitoring Device For Measuring Photoplethysmograhic SignalsDzuzu LicezNo ratings yet
- 1 PBDocument11 pages1 PBmarcos78arNo ratings yet
- Toward A Smartphone Application For Estimation of Pulse Transit TimeDocument19 pagesToward A Smartphone Application For Estimation of Pulse Transit TimePK PKNo ratings yet
- Wearable Photoplethysmographic Sensors - Seminar Report, PPT, PDF For ECE StudentsDocument6 pagesWearable Photoplethysmographic Sensors - Seminar Report, PPT, PDF For ECE StudentsvvkrkzNo ratings yet
- Irjet V4i5119 PDFDocument7 pagesIrjet V4i5119 PDFAnonymous plQ7aHUNo ratings yet
- Original PaperDocument6 pagesOriginal PaperDavid Ramirez AlanocaNo ratings yet
- Oximetro de PulsoDocument9 pagesOximetro de PulsoMartín NuñezNo ratings yet
- 10 Classification of Biomedical Signal On Iot Platform Using Support Vector MachineDocument4 pages10 Classification of Biomedical Signal On Iot Platform Using Support Vector MachineESP32 CAMNo ratings yet
- Heartbeat Monitoring Alert Via SMSDocument5 pagesHeartbeat Monitoring Alert Via SMSgualutalewNo ratings yet
- Non-Invasive Total Hemoglobin Measurement by Forehead OximetryDocument3 pagesNon-Invasive Total Hemoglobin Measurement by Forehead OximetryJayanthi ThiruvengadamNo ratings yet
- HeartrateDocument5 pagesHeartrateaishwaryaNo ratings yet
- Determination of Spo2 and Heart Beat Using ArduinoDocument20 pagesDetermination of Spo2 and Heart Beat Using Arduinodulipala alekya gupthaNo ratings yet
- Multiparameter Respiratory Rate Estimation From The PhotoplethysmogramDocument9 pagesMultiparameter Respiratory Rate Estimation From The PhotoplethysmogramCalm YourselfNo ratings yet
- Low-Cost Phonocardiogram Board With Graphic LCD, Solar Panel and Embedded Heart Sound AnalyserDocument7 pagesLow-Cost Phonocardiogram Board With Graphic LCD, Solar Panel and Embedded Heart Sound AnalyserLionel LapinouNo ratings yet
- Non Invasive Blood Glucose Monitoring Using Near Infrared SpectrosDocument10 pagesNon Invasive Blood Glucose Monitoring Using Near Infrared SpectrosErmias MulusewNo ratings yet
- Biomedical Signal Processing and Control: Sourav Kumar Mukhopadhyay, M. Omair Ahmad, M.N.S. SwamyDocument13 pagesBiomedical Signal Processing and Control: Sourav Kumar Mukhopadhyay, M. Omair Ahmad, M.N.S. SwamyfatimaNo ratings yet
- Biomedical Instrumentation Project Report: Submitted byDocument7 pagesBiomedical Instrumentation Project Report: Submitted bymahsa sherbafiNo ratings yet
- Design and Implementation of An OCC-Based Real-Time Heart Rate and Pulse-Oxygen Saturation Monitoring SystemDocument8 pagesDesign and Implementation of An OCC-Based Real-Time Heart Rate and Pulse-Oxygen Saturation Monitoring SystemFaisal AhmedNo ratings yet
- Pulse Oximetry Based On Photoplethysmography Imaging With Red and Green LightDocument11 pagesPulse Oximetry Based On Photoplethysmography Imaging With Red and Green Lightmahsa sherbafiNo ratings yet
- Boe 11 10 5458 BCGDocument12 pagesBoe 11 10 5458 BCGpuma flyerNo ratings yet
- Paper - 6747 MAX30102Document8 pagesPaper - 6747 MAX30102caveda1234No ratings yet
- Bim PresentationDocument23 pagesBim PresentationHoorain SajjadNo ratings yet
- 1011 88120 2 10 20221111 PDFDocument14 pages1011 88120 2 10 20221111 PDFNiteshNo ratings yet
- 65 PDFDocument7 pages65 PDFShajan SNo ratings yet
- Sensors 13 06552Document26 pagesSensors 13 06552Eemaan AzizNo ratings yet
- Poximeter 2.0Document34 pagesPoximeter 2.0Srinivasa Reddy Devireddy100% (1)
- Combined 1 6Document6 pagesCombined 1 6srrameshonline8854No ratings yet
- Fibre-Grating Sensors For The Measurement of PhysiDocument5 pagesFibre-Grating Sensors For The Measurement of PhysiagushattaNo ratings yet
- Estimation of Arterial Stiffness by Using PPG Signal: A ReviewDocument4 pagesEstimation of Arterial Stiffness by Using PPG Signal: A ReviewseventhsensegroupNo ratings yet
- Motion Artifact Red PPG AS-LMS Adaptive Filter Ashoka ReddyDocument13 pagesMotion Artifact Red PPG AS-LMS Adaptive Filter Ashoka ReddyAlex WongNo ratings yet
- Smartphone-Based Photoplethysmogram Measurement: January 2012Document31 pagesSmartphone-Based Photoplethysmogram Measurement: January 2012Boogie WritesNo ratings yet
- 134-Article Text-557-1-10-20211011Document8 pages134-Article Text-557-1-10-20211011dita rahmawatiNo ratings yet
- Design of An Electromyograph Equipped With Digital Neck Angle Elevation GaugeDocument8 pagesDesign of An Electromyograph Equipped With Digital Neck Angle Elevation Gaugedita rahmawatiNo ratings yet
- Combining Parallel Adaptive Filtering and Wavelet ThresholdDocument9 pagesCombining Parallel Adaptive Filtering and Wavelet ThresholdAkilesh MDNo ratings yet
- Heart Disease Prediction SystemDocument8 pagesHeart Disease Prediction SystemAnjanaNo ratings yet
- Conference RRDocument7 pagesConference RRJeaneffil VimalrajNo ratings yet
- Animal Tracking and GPS SystemDocument13 pagesAnimal Tracking and GPS Systemm niru50% (2)
- A NoveEOG L Topology For Design and Development of Wireless Electro Oculogram Biopotential AmpliferDocument6 pagesA NoveEOG L Topology For Design and Development of Wireless Electro Oculogram Biopotential AmpliferAbhinav GuptaNo ratings yet
- 967 978-1-4673-6997-8/15/$31.00 ©2015 Ieee Icassp 2015Document5 pages967 978-1-4673-6997-8/15/$31.00 ©2015 Ieee Icassp 2015Abdallah ToolmakerNo ratings yet
- Yellow Light The Next Technology For Smart WatchesDocument8 pagesYellow Light The Next Technology For Smart WatchesIJAR JOURNALNo ratings yet
- Wireless Monitoring of Physiological Data Using Nexus-10 & BiotraceDocument64 pagesWireless Monitoring of Physiological Data Using Nexus-10 & BiotraceInternational Journal of Application or Innovation in Engineering & ManagementNo ratings yet
- Oe 30 8 13121 DNN ShuyangDocument13 pagesOe 30 8 13121 DNN Shuyangpuma flyerNo ratings yet
- A Multi-Channel Electromyography, Electrocardiography and Inertial Wireless Sensor Module Using Bluetooth Low-EnergyDocument27 pagesA Multi-Channel Electromyography, Electrocardiography and Inertial Wireless Sensor Module Using Bluetooth Low-EnergyAbhishekNo ratings yet
- ICTTSE 2022 ETC FINAL PAPER REVIEV 1 Harsh DaharwalDocument3 pagesICTTSE 2022 ETC FINAL PAPER REVIEV 1 Harsh DaharwalHarsh DaharwalNo ratings yet
- Non-Constrained Blood Pressure Monitoring Using ECG and PPG For Personal HealthcareDocument6 pagesNon-Constrained Blood Pressure Monitoring Using ECG and PPG For Personal Healthcaremaxor4242No ratings yet
- Photoplethesmography (PPG) : A Novel Tool in Physiological MeasurementDocument11 pagesPhotoplethesmography (PPG) : A Novel Tool in Physiological MeasurementReddyvari VenugopalNo ratings yet
- ECG2Document21 pagesECG2spNo ratings yet
- D1.2 - Specification Report On Optical SensorsDocument20 pagesD1.2 - Specification Report On Optical SensorsSaqib HashmiNo ratings yet
- A Multi-Channel Electromyography ElectrocardiograpDocument27 pagesA Multi-Channel Electromyography ElectrocardiograpVizaNo ratings yet
- Monitoring Respiratory Rate Via AndroidDocument7 pagesMonitoring Respiratory Rate Via Androidmochamad aldi bahij farobyNo ratings yet
- PP - Week 5 - Premature Newborn - Concept MapDocument2 pagesPP - Week 5 - Premature Newborn - Concept MapSarah CollinsNo ratings yet
- KS3 Human Organ SystemDocument2 pagesKS3 Human Organ Systemejljn1No ratings yet
- Congenital Diaphragmatic HerniaDocument40 pagesCongenital Diaphragmatic HerniaPothina Sree HariNo ratings yet
- Cardiac Case StudyDocument44 pagesCardiac Case StudyNatalia Bernard100% (1)
- NCP Decreased Cardiac OutputDocument2 pagesNCP Decreased Cardiac OutputYamete KudasaiNo ratings yet
- Osmosis Case Study PDFDocument4 pagesOsmosis Case Study PDFRenata ZavalzaNo ratings yet
- S4 Biology 2018 T2 WK05 LPDocument3 pagesS4 Biology 2018 T2 WK05 LPLoire Aviles CollamatNo ratings yet
- Traumatic ShockDocument22 pagesTraumatic ShockOlga GoryachevaNo ratings yet
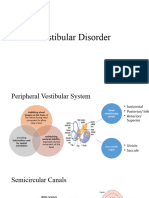
- Vestibular DisorderDocument22 pagesVestibular DisorderSumbal SalikNo ratings yet
- Open Heart Surgery JournalDocument3 pagesOpen Heart Surgery Journalapi-546517574No ratings yet
- BIO - F5 - KSSM - CHAPTER - 1 - 1.1 and 1.2 ORGANISATION OF PLANT TISSUES AND GROWTHDocument59 pagesBIO - F5 - KSSM - CHAPTER - 1 - 1.1 and 1.2 ORGANISATION OF PLANT TISSUES AND GROWTHwienna1987100% (2)
- PhysioEx Nuzla Emira Potensial AksiDocument7 pagesPhysioEx Nuzla Emira Potensial AksiPine's FauNo ratings yet
- Regional Circulation: Prof. K. SivapalanDocument23 pagesRegional Circulation: Prof. K. SivapalanjikookNo ratings yet
- Introduction To Transfusion MedicineDocument12 pagesIntroduction To Transfusion MedicineSamantha BuiNo ratings yet
- CMC Maritime Academy - Chennai MFA-Exit Exam Questions: (Revision JUNE 2021) - 1Document4 pagesCMC Maritime Academy - Chennai MFA-Exit Exam Questions: (Revision JUNE 2021) - 1Meghanath AdkonkarNo ratings yet
- Indications For Weaning: Kilips Classification of Ami With Expected Hospital Mortality RateDocument8 pagesIndications For Weaning: Kilips Classification of Ami With Expected Hospital Mortality RateSerious LeoNo ratings yet
- Homeostasis and The Excretory SystemDocument21 pagesHomeostasis and The Excretory Systemmark smithNo ratings yet
- Walter Cannon, Homeostasis and The Physiological Response To StressDocument12 pagesWalter Cannon, Homeostasis and The Physiological Response To StressMarc Imhotep Cray, M.D.No ratings yet
- Diabetes Mellitus Nursing Care PlanDocument7 pagesDiabetes Mellitus Nursing Care PlanjamieboyRN91% (32)
- ASN 11 Handout Case Study PDFDocument4 pagesASN 11 Handout Case Study PDFania ojedaNo ratings yet
- Pig Heart Dissection Lab Write UpDocument5 pagesPig Heart Dissection Lab Write Upapi-94693850No ratings yet
- Plant ExcretionDocument25 pagesPlant ExcretionPatrick Tew100% (1)
- ElectrolytesDocument2 pagesElectrolytestentenNo ratings yet
- Immediate Physiological Changes in New BornDocument7 pagesImmediate Physiological Changes in New BornLahunWanniangNo ratings yet
- SSI Freediving Level 1Document2 pagesSSI Freediving Level 1StephanieNo ratings yet
- Chapter 5Document9 pagesChapter 5CH2V2RR12No ratings yet
- Anatomy of The KidneyDocument7 pagesAnatomy of The KidneyArgie Arguson IINo ratings yet
- Assessment Nursing Diagnosis Scientific Explanation Planning Nursing Intervention RationaleDocument3 pagesAssessment Nursing Diagnosis Scientific Explanation Planning Nursing Intervention Rationalekimglaidyl bontuyanNo ratings yet
- Drug StudyDocument4 pagesDrug Studygrandville cabildoNo ratings yet
- Laporan Pendahuluan DM RsumDocument17 pagesLaporan Pendahuluan DM RsumMelinia AnggitaNo ratings yet
- Organic Chemistry for Schools: Advanced Level and Senior High SchoolFrom EverandOrganic Chemistry for Schools: Advanced Level and Senior High SchoolNo ratings yet
- Periodic Tales: A Cultural History of the Elements, from Arsenic to ZincFrom EverandPeriodic Tales: A Cultural History of the Elements, from Arsenic to ZincRating: 3.5 out of 5 stars3.5/5 (137)
- The Disappearing Spoon: And Other True Tales of Madness, Love, and the History of the World from the Periodic Table of the ElementsFrom EverandThe Disappearing Spoon: And Other True Tales of Madness, Love, and the History of the World from the Periodic Table of the ElementsRating: 4 out of 5 stars4/5 (146)
- Is That a Fact?: Frauds, Quacks, and the Real Science of Everyday LifeFrom EverandIs That a Fact?: Frauds, Quacks, and the Real Science of Everyday LifeRating: 5 out of 5 stars5/5 (4)
- Monkeys, Myths, and Molecules: Separating Fact from Fiction, and the Science of Everyday LifeFrom EverandMonkeys, Myths, and Molecules: Separating Fact from Fiction, and the Science of Everyday LifeRating: 4 out of 5 stars4/5 (1)
- The Regenerative Grower's Guide to Garden Amendments: Using Locally Sourced Materials to Make Mineral and Biological Extracts and FermentsFrom EverandThe Regenerative Grower's Guide to Garden Amendments: Using Locally Sourced Materials to Make Mineral and Biological Extracts and FermentsRating: 5 out of 5 stars5/5 (3)
- The Elements We Live By: How Iron Helps Us Breathe, Potassium Lets Us See, and Other Surprising Superpowers of the Periodic TableFrom EverandThe Elements We Live By: How Iron Helps Us Breathe, Potassium Lets Us See, and Other Surprising Superpowers of the Periodic TableRating: 3.5 out of 5 stars3.5/5 (22)
- The Periodic Table: A Very Short IntroductionFrom EverandThe Periodic Table: A Very Short IntroductionRating: 4.5 out of 5 stars4.5/5 (3)
- The Nature of Drugs Vol. 1: History, Pharmacology, and Social ImpactFrom EverandThe Nature of Drugs Vol. 1: History, Pharmacology, and Social ImpactRating: 5 out of 5 stars5/5 (5)
- Chemistry for Breakfast: The Amazing Science of Everyday LifeFrom EverandChemistry for Breakfast: The Amazing Science of Everyday LifeRating: 4.5 out of 5 stars4.5/5 (90)
- Handbook of Formulating Dermal Applications: A Definitive Practical GuideFrom EverandHandbook of Formulating Dermal Applications: A Definitive Practical GuideNo ratings yet
- A Perfect Red: Empire, Espionage, and the Quest for the Color of DesireFrom EverandA Perfect Red: Empire, Espionage, and the Quest for the Color of DesireRating: 4 out of 5 stars4/5 (129)
- Water-Based Paint Formulations, Vol. 3From EverandWater-Based Paint Formulations, Vol. 3Rating: 4.5 out of 5 stars4.5/5 (6)
- Essential Oil Chemistry Formulating Essential Oil Blends that Heal - Aldehyde - Ketone - Lactone: Healing with Essential OilFrom EverandEssential Oil Chemistry Formulating Essential Oil Blends that Heal - Aldehyde - Ketone - Lactone: Healing with Essential OilRating: 5 out of 5 stars5/5 (1)
- Bioplastics: A Home Inventors HandbookFrom EverandBioplastics: A Home Inventors HandbookRating: 4 out of 5 stars4/5 (2)
- Chemistry: a QuickStudy Laminated Reference GuideFrom EverandChemistry: a QuickStudy Laminated Reference GuideRating: 5 out of 5 stars5/5 (1)
- Formulating, Packaging, and Marketing of Natural Cosmetic ProductsFrom EverandFormulating, Packaging, and Marketing of Natural Cosmetic ProductsNo ratings yet
- Guidelines for Integrating Process Safety into Engineering ProjectsFrom EverandGuidelines for Integrating Process Safety into Engineering ProjectsNo ratings yet
- The Periodic Table of Elements - Alkali Metals, Alkaline Earth Metals and Transition Metals | Children's Chemistry BookFrom EverandThe Periodic Table of Elements - Alkali Metals, Alkaline Earth Metals and Transition Metals | Children's Chemistry BookNo ratings yet
- The Periodic Table of Elements - Post-Transition Metals, Metalloids and Nonmetals | Children's Chemistry BookFrom EverandThe Periodic Table of Elements - Post-Transition Metals, Metalloids and Nonmetals | Children's Chemistry BookNo ratings yet