Professional Documents
Culture Documents
Critical Decisions in Airway Management
Uploaded by
Pablo RamirezOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Critical Decisions in Airway Management
Uploaded by
Pablo RamirezCopyright:
Available Formats
Just Breathe
Rapid-Sequence
Intubation
LESSON 24
By Joshua T. McClain, MD; Benjamin J. Lawner, DO, EMT-P;
and Kenneth H. Butler, DO, FACEP
Dr. McClain is an emergency medicine physician at Meritus Health in Hagerstown,
Maryland. Dr. Lawner is an adjunct assistant professor and Dr. Butler is an associate
professor in the Department of Emergency Medicine at the University of Maryland
School of Medicine in Baltimore.
Reviewed by John C. Greenwood, MD
OBJECTIVES
On completion of this lesson, you should be able to: CRITICAL DECISIONS
1. Explain how to properly position and oxygenate patients n How should patients be positioned for RSI?
undergoing RSI.
2. Discuss the ideal pharmacologic agents for n How should patients be oxygenated during RSI?
pretreatment, induction, and paralysis. n Which pretreatment agents should be considered?
3. Describe the evidence surrounding the use of cricoid
pressure. n Is there an ideal induction agent?
4. Demonstrate techniques and strategies for maximizing n What paralytic agents are most effective, and when
the clinician’s view during RSI. should they be used?
FROM THE EM MODEL n Should cricoid pressure be applied during RSI?
19.0 Procedures and Skills Integral to the Practice
n What techniques can be used to maximize the view
of Emergency Medicine
during RSI?
19.1 Airway Techniques
19.1.1 Intubation
The ability to perform rapid-sequence intubation (RSI) is an essential skill for the practice of emergency
medicine. The decision to intubate must often be made at a moment’s notice and with only limited knowledge of the
patient’s history. Unfortunately, failure to intubate a patient on the first attempt more than doubles the risk of adverse
events.1-3 Because these choices can mean the difference between life and death, clinicians must possess an in-depth
understanding of ideal oxygenation conditions, medication strategies, and patient positioning.
December 2019 n Volume 33 Number 12 19
CASE PRESENTATIONS
■ CASE ONE hypertonic saline and vitamin K, and saturation 81% on NIPPV. The
requests fresh frozen plasma from clinician prepares to intubate the
A 59-year-old man with a history
of hypertension and atrial fibrillation the blood bank. The clinical team patient.
arrives via ambulance after being prepares to intubate the patient in
order to obtain a CT scan. ■ CASE THREE
found with an altered level of
A 73-year-old man presents with
consciousness. He is breathing
■ CASE TWO altered mental status. His daughter
spontaneously but has a Glasgow
Coma Scale (GCS) score of 5. The An obese 44-year-old woman states that the patient has become
patient’s wife mentions that he takes with a history of COPD presents in progressively incoherent over the past
a prescription for warfarin. His respiratory distress on noninvasive few days. His medical history includes
physical examination reveals a blown positive-pressure ventilation (NIPPV). Alzheimer disease and diabetes mellitus.
left pupil. His vital signs are blood EMS administered a nebulizer His GCS score is 7. The examination
pressure 186/101, heart rate 66, treatment and steroids en route. A reveals dry mucous membranes.
respiratory rate 9, rectal temperature brief history reveals that the patient His vital signs are blood pressure
36.9°C (98.4°F), and oxygen has been intubated twice in the past 68/42, heart rate 128, respiratory rate
saturation 97% on a nonrebreather for respiratory distress. 24, temperature 39.3°C (102.7°F), and
mask. She has severely decreased air oxygen saturation 94% on room air.
Suspecting an intracranial bleed entry bilaterally and diffuse, faint His finger-stick blood glucose level is
with elevated intracranial pressure, wheezing. Her vital signs are blood 185 mg/dL. The physician considers
the emergency physician elevates the pressure 143/79, heart rate 114, intubating the patient for airway
head of the patient’s bed, administers respiratory rate 22, and oxygen protection.
CRITICAL DECISION CRITICAL DECISION mask (BVM) with a positive end-
expiratory pressure (PEEP) valve, or
How should patients be How should patients be
continuous positive airway pressure
positioned for RSI? oxygenated during RSI?
(CPAP). High-risk patients (those with
Proper patient positioning during During the preoxygenation and apneic a preintubation oxygen saturation of
RSI is essential. A completely flat oxygenation periods, oxygen should be ≤90% on a nonrebreather mask) should
position should be avoided. Alignment administered via nasal cannula at a rate be preoxygenated using a BVM with a
of the clivus with the external auditory of 15 L/min. Apneic oxygenation creates PEEP valve or CPAP.6
meatus, correlating with the ear and the a diffusion gradient from the pharynx to If available, high-flow nasal cannula
sternal notch respectively, may produce the lungs, providing oxygenation even in oxygen therapy can also be used for the
superior laryngoscopic and intubating the absence of ventilation. In one study of
preoxygenation and apneic oxygenation
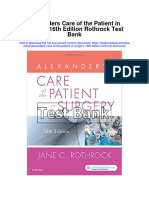
views.4 In obese patients, a ramped obese men undergoing general anesthesia,
of medium- and high-risk patients.11
patients receiving apneic oxygenation
position is often required to align High-flow nasal cannula oxygen
took 1 minute and 40 seconds longer to
the ear and sternal notch; this can be therapy increases patient comfort,
desaturate than patients not receiving
achieved by placing several blankets or induces a small amount of CPAP, and
apneic oxygenation.8 Although research
pillows under the patient’s head, neck, creates a higher fraction of inspired
has been mixed, the rate of first-pass
and upper back (Figure 1).5 oxygen (FiO2).12
success may be higher (and the risk of
Along with ear-to-sternal-notch Clinicians should fully understand
hypoxemia may be lower) in emergency
positioning, the head of the bed should how their institution’s oxygen delivery
department patients who receive apneic
be elevated to at least 20 degrees oxygenation.9,10 devices work. When using a BVM, a
for preoxygenation and during the In addition to a nasal cannula, low- tight seal should be achieved. The bag
intubation attempt. Patients in a risk patients (those with preintubation does not need to be squeezed if the
flat position have increased work of oxygen saturation levels of 96%-100% patient is breathing spontaneously,
breathing during the preoxygenation on a nonrebreather mask) can be can tolerate the tight seal, and is able
period and increased rates of preoxygenated with a nonrebreather to generate enough force to open the
atelectasis.6 When the head of the bed mask. Medium-risk patients (those one-way valve. To avoid a problematic
is elevated 20 degrees, patients appear with a preintubation oxygen saturation drop in FiO2, this method should only
to take about 1 minute and 30 seconds level of 91%-95% on a nonrebreather be used with bags that possess a one-
longer to desaturate than when the bed mask) can be preoxygenated with way exhalation port.13 Hovering the
is flat.7 a nonrebreather mask, a bag valve bag above the patient’s face — another
20 Critical Decisions in Emergency Medicine
common mistake — provides no bagging during the apneic period should patients prior to induction. This may be
advantage over room air.6 be mandatory to prevent hypercapnia necessary for several reasons, including
When it comes to oxygen delivery via (eg, salicylate overdose, severe metabolic increased intracranial pressure, a
a nonrebreather mask, an ideal mask can acidosis, increased intracranial pressure). history of cardiovascular disease, and
deliver upward of 90% FiO2; however, Ultimately, the decision to bag or not shock states.
many emergency departments are not to bag during RSI is a balance of risks In the past, lidocaine was routinely
equipped with true nonrebreather masks. (aspiration) and benefits (preventing used to blunt the sympathetic response
The masks found in most acute settings desaturation).6,18 to laryngoscopy in patients for whom the
typically deliver only 60% to 70% FiO2.
concomitant rise in intracranial pressure
Rates higher than this can be achieved CRITICAL DECISION
would be particularly detrimental.
by increasing the flow rate past the Which pretreatment agents However, subsequent research has
15 L/min mark, which can achieve rates should be considered? shown no evidence to support the use of
as high as 30 to 60 L/min.6
The recommended duration for Pretreatment involves the lidocaine in clinical practice.19
preoxygenation has generally been administration of medications to at-risk Fentanyl, which appears to blunt
3 minutes of tidal volume breathing,
or 8 maximal breaths.14 When there is a FIGURE 1. Ramped Patient Position
mask leak, which occurs often with the A.
use of standard emergency department
nonrebreather masks, 3 minutes of
tidal volume breathing may provide
better oxygenation.15 In such cases, the
addition of a nasal cannula can also
increase the FiO2.
To Bag or Not To Bag?
Another controversy in airway
management is whether or not patients
should be “bagged” after a sedative and
paralytic have been administered. Any
patient who is desaturating should be
bagged. But what about a patient who
is not desaturating? In a 1961 study,
pressures kept below 15 cm H2O did
not cause gastric insufflation.16 Another B.
study published in 2013 randomized
patients undergoing elective surgery into
groups with pressures of 10, 15, 20, and
25 cm H2O after an induction agent was
administered.
The investigators in the 2013 study
listened and looked for gastric insufflation
and observed the antrum size while
bagging. As pressures increased, so did
the levels of insufflation. In the pressure-
of-10 group, there was no increase in the
gastric antrum size; however, this pressure
would be inadequate for long-term
ventilation. In the pressure-of-15 group,
ventilation was optimal, but the antrum
size did increase by a small degree.17
Current recommendations regarding
bagging during the apneic period are
mixed. Based on current evidence,
practitioners should limit pressures to
10 to 15 cm H2O if they are going to bag. A. Flat; no attempt is made to achieve the best airway position.
Excluding a few subgroups for whom B. Ramping improves upper-airway patency and decreases work of breathing.
December 2019 n Volume 33 Number 12 21
TABLE 1. IV Induction and Neuromuscular-Blocking Agents for RSI
Dose if
Hemodynamically
Agent Standard Dose Compromised Comments
Etomidate 0.2-0.3 mg/kg Full dose may be Rapid onset, short duration. Few hemodynamic effects.
required, but lower Preferred for hypotensive patients with head injuries or
doses are safer. coronary artery disease.
Ketamine 1.0-2.0 mg/kg Lower end of dose Longer duration. Sympathetic stimulation, bronchodilation,
dreams, salivation. Preferred for patients with asthma.
Propofol 2.0-2.5 mg/kg given at Total dose may be Slow injection preferred over rapid bolus administration.
40 mg every 10 seconds as low as 10%. Rapid bolus may result in cardiorespiratory depression.
Titrate dose to response. Maintenance doses by infusion are
preferred: 0.3-3.0 mg/kg/hr for prolonged sedation. Avoid in
patients with hypovolemia.
Fentanyl and Fentanyl 1.0-4.0 mcg/kg Reduce by 50%. Can cause respiratory depression during initial
midazolam for pain; midazolam administration. Excellent for prolonged sedation and pain
5.0-10.0 mg for sedation control, but monitor vital signs often.
Succinylcholine 0.6-1.5 mg/kg Consider increasing Short-acting. Many contraindications and adverse effects.
total dose. Clinical duration 4-6 minutes.
Rocuronium 0.6-1.5 mg/kg Consider increasing Onset time is equal to that of succinylcholine. Clinical
total dose. duration 30-60 minutes.
Vecuronium 0.08-0.10 mg/kg Consider increasing Onset time 2-3 minutes. Clinical duration 25-40 minutes.
total dose.
increases in blood pressure and appears to be no difference between dose of etomidate increased mortality
heart rate, should be considered for the two drugs in mortality rate and secondary to adrenal insufficiency in
patients with potential intracranial hemodynamic effects.25,26 septic patients. Given the conflicting
hypertension.20 The medication should Ketamine causes dissociative literature and the fact that ketamine is a
also be considered for patients with a amnesia and provides analgesia through viable alternative, etomidate should be
history of ischemic heart disease and for the NMDA receptor. An induction avoided in septic patients.31,32
those at risk of an aortic aneurysm or dose of 1 to 2 mg/kg has traditionally
Traumatic Brain Injuries
dissection.21 Pretreatment with esmolol been recommended; however,
at a dose of 1.5 mg/kg can be used if patients in shock should receive no Historically, ketamine has been
heart rate elevation is a major peri- more than 1.5 mg/kg (or even less avoided in patients who may have
intubation concern.22 if the patient may be catecholamine suffered intracranial injuries based
Patients in shock present a serious depleted). Etomidate stimulates the on studies and case reports published
challenge for emergency physicians. gamma-aminobutyric acid receptor to in the 1970s, which demonstrated an
Patients with preintubation hypotension produce a sedative amnestic state.21 association between ketamine and
have a much greater risk of cardiac The traditional dose is 0.3 mg/kg; increased intracranial pressure.33 In
arrest and death than those who are unlike with propofol and ketamine, recent years, this cause-and-effect
normotensive.23 If time and clinical which require dose reductions in cases relationship has been challenged.21
status permit, isotonic fluids, blood of shock, the etomidate dose should Current literature even suggests that
products, and vasopressors should be remain unchanged or only be increased ketamine is appropriate for patients
provided as clinically indicated, with minimally.27 with traumatic brain injuries because of
a goal of increasing the mean arterial its ability to increase cerebral perfusion
Sepsis pressure and reduce the release of
pressure prior to intubation. It is
Ketamine should usually be the first- glutamate, which can be neurotoxic.33
important to remember that RSI and
line induction agent for patients with
NIPPV can cause dramatic decreases in
sepsis. Although several small studies CRITICAL DECISION
blood pressure.
have found a relationship between What paralytic agents are
CRITICAL DECISION etomidate and adrenal suppression,
most effective, and when
subsequent research has questioned
Is there an ideal induction should they be used?
the clinical significance of this
agent? association.28-30 Paralytic agents should be used
Because of their favorable One study showed that a single dose during all RSI attempts. In a study that
hemodynamic profiles, ketamine and of etomidate for intubation did not compared how laryngoscopy performed
etomidate have emerged as the induction increase the rate of in-hospital deaths with etomidate plus a paralytic versus
agents of choice in many emergency and other adverse outcomes. However, etomidate alone, acceptable intubating
departments (Table 1).24 There another study found that a single conditions were reported in 79% of the
22 Critical Decisions in Emergency Medicine
patients who received the paralytic but serum potassium levels. In healthy is that patients who receive it take
only in 13% of those who did not.34 patients who receive the drug, serum longer to desaturate than those who
Airway trauma occurred in 28% of potassium concentrations rise an receive succinylcholine. Patients given
nonparalyzed patients, aspiration in 15%, average of 0.5 to 1 mEq/L. In patients succinylcholine also desaturate to lower
and death in 3%. The researchers did not with comorbidities or acute medical oxygen levels and take longer to achieve
observe any of these complications in the conditions, receptor upregulation can resaturation compared with patients
group receiving a paralytic.35 lead to much larger increases. The who receive rocuronium.41,42
risk is greatest in patients with severe A common misconception is that
Rocuronium vs Succinylcholine infections, in those with upper- and succinylcholine is safer because of its
Because of the undifferentiated lower-motor neuropathies (including short duration of action. However, using
nature of emergency department diabetic peripheral neuropathy and a paralytic in the emergency department
cases and the extensive risks and side severe peripheral vascular disease), should be an all-or-nothing scenario. As
effects associated with succinylcholine, after exposure to certain toxins and noted by emergency medicine researcher
rocuronium should be the emergency medications, in patients who require Reuben Strayer, “Emergency clinicians
physician’s first-line paralytic. immobilization, and in those with burns who believe they are protected against a
Rocuronium has few side effects, and or trauma.38 ‘can’t intubate, can’t ventilate’ scenario
its only absolute contraindication In addition to receptor upregulation, by the short duration of succinylcholine
is in patients with an allergy to life-threatening hyperkalemia are usually wrong and make dangerous
nondepolarizing paralytics.36 At a dose secondary to succinylcholine-induced decisions as a result.”43 Furthermore,
of 1.2 mg/kg, rocuronium produces rhabdomyolysis has been documented in the use of a short-acting drug leaves
intubating conditions equivalent to several case reports.39 Other side effects physicians where they were in the first
1.5 mg/kg of succinylcholine when both of the drug include masseter muscle place: needing to intubate the patient.
are compared at 45 seconds.37 spasms, malignant hyperthermia, and In the rare circumstance that
The main concern with increased intracranial pressure.24,40 the physician would like to reverse
succinylcholine is the effect it has on Another benefit of rocuronium rocuronium paralysis, sugammadex can
be used. Sugammadex was approved by
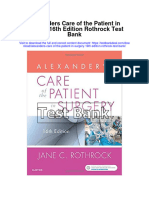
FIGURE 2. Surface Anatomy of the Hyoid Bone, Thyroid, and Cricoid the FDA in 2015 as a reversal agent for
Cartilage rocuronium bromide and vecuronium
bromide.44 However, it is important
to be aware that up to 1% of patients
who are given the emergent reversal
dose of 16 mg/kg have hypersensitivity
reactions.45
CRITICAL DECISION
Hyoid bone Should cricoid pressure be
applied during RSI?
Thyroid cartilage
Major controversy surrounds the use
of cricoid pressure, sometimes called the
Cricoid cartilage Sellick maneuver. The technique was first
described by Scottish physician Alexander
Monro, who used it to revive drowning
victims. The maneuver was popularized
in 1960s when British anesthesiologist
Brian Sellick promoted its efficacy for
controlling gastric regurgitation during
the induction of anesthesia.46 Sellick
hypothesized that, by applying backward
pressure to the cricoid cartilage (Figure
2) against the cervical vertebrae, he
could occlude the upper esophagus. His
original study involved 26 patients, who
experienced no aspiration events when
cricoid pressure was applied; however,
3 of the subjects experienced aspiration
COURTESY OF THE NEW YORK SCHOOL OF REGIONAL ANESTHESIA
when the pressure was released.47
December 2019 n Volume 33 Number 12 23
Several more recent studies have the American Heart Association Other refining factors can be
questioned whether the application removed the technique from its CPR applied to blade selection when several
of cricoid pressure occludes the and emergency cardiovascular care options are available. In general, English
esophagus, which lies lateral to the guidelines. In addition, the Eastern Macintosh blades outperform standard
airway in an estimated 60% of patients. Association for the Surgery of Trauma Macintosh models.62 It is important
When pressure is applied, the trachea no longer endorses the maneuver as a to select the shortest handle available,
can be displaced laterally instead of level 1 recommendation.54 especially when intubating obese
being compressed against the cervical patients; adipose tissue in the chest and
vertebrae.48,49 Nonetheless, the positioning CRITICAL DECISION neck can hinder blade insertion when
of the esophagus may actually be What techniques can be using a longer handle.63 Finally, the
irrelevant, as the cricoid ring is attached Macintosh 3 and Macintosh 4 blades
used to maximize the view
to the hypopharynx, not the esophagus, provide different benefits. A Macintosh 4
and the two structures move together as during RSI? can be used as a Miller in most patients
a unit. Cricoid pressure appears to reduce Blades with a grade 3 or 4 airway; however,
the diameter of the hypopharynx by an the device places the clinician at a
Although video laryngoscopy
average of only 35%.50 mechanical disadvantage during most
generally outperforms direct
The application of cricoid pressure intubations because of its longer blade
laryngoscopy, emergency physicians
is not without risks, including airway length.
should master the direct technique
compression and compromised glottic
so that it can be used when video Tubes
views.49,51 The other concern is that
equipment is unavailable or in situations Traditional arcuate stylets are slowly
the technique may actually cause the
where video imaging cannot provide being phased out in favor of straight-
problems it sets out to prevent. In one
study, when 20 newtons of force were an adequate view.55,56 Inexperienced to-cuff models, which provide greater
applied to the cricoid cartilage, the lower clinicians may find more success with maneuverability without the midportion
esophageal sphincter pressure decreased curved Macintosh blades over straight of the tube obscuring the laryngeal inlet
from 24 to 15 mm Hg. A force of Miller blades, which may provide poorer — a drawback of arcuate devices. The
40 newtons caused the pressure to drop intubating views (Figure 3).57,58 However, ideal angle at the cuff is 25 degrees, but
to 13 mm Hg.52 One of the largest studies research suggests that Miller blades may there appears to be a dramatic drop-off
on the use of cricoid pressure found the outperform Macintosh models when in the ability to intubate with angles
procedure to be ineffective for preventing using a paraglossal approach.59 Although above 35 degrees.64
regurgitation or death in patients Miller blades have traditionally Epiglottis-Only View
undergoing caesarian deliveries.53 been preferred for pediatric patients, If the laryngoscopic view remains
Major medical organizations Macintosh blades can provide similar limited to the epiglottis, several
have also noted the lack of evidence views with comparable success and alternative approaches exist. First, the
supporting cricoid pressure. In 2010, failure rates.60,61 clinician should advance the blade
further into the vallecula to ensure
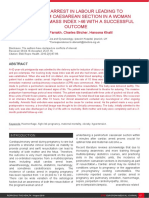
FIGURE 3. Miller and Macintosh Blades adequate engagement of the hyoepiglottic
ligament. If this fails to fix the problem,
external laryngeal manipulation can
be attempted. In such cases, a modified
approach (in which the physician
attempting the intubation adjusts an
assistant’s hand) appears to perform
better than the classic approach.65 Finally,
using a head-lift position may help bring
the airway into view.66
If the laryngeal view remains
elusive after employing these options,
a difficult-airway algorithm should be
followed (Figure 4). Although these
techniques are beyond the scope of
this article, other options may entail
changing blades, switching to or
from video laryngoscopy, inserting a
supraglottic airway device (SAD), using
Miller blades Macintosh blades a fiberoptic scope, seeking assistance, or
creating a surgical airway.
24 Critical Decisions in Emergency Medicine
FIGURE 4. Management of Unanticipated, Difficult Tracheal Intubation in Adults
PLAN A: Facemask ventilation and tracheal intubation If in difficulty call for help!
• Optimize the patient’s head and neck position.
• Preoxygenate.
• Provide adequate neuromuscular blockade. Succeed
• Attempt direct or video laryngoscopy (max 3+1 attempts). Confirm tracheal intubation with capnography.
• Provide external laryngeal manipulation.
• Use a bougie.
• Remove cricoid pressure.
• Maintain oxygenation and anaesthesia.
Declare failed intubation
PLAN B: Maintaining oxygenation via SAD insertion STOP AND THINK
Options (consider risks and benefits):
• A 2nd-generation device is recommended.
Succeed 1. Wake the patient up.
• Change the device or size (maximum 3 attempts).
• Oxygenate and ventilate. 2. Intubate the trachea via SAD.
3. Proceed without intubating the trachea.
Declare failed supraglottic ventilation 4. Perform a tracheostomy or cricothyroidotomy.
PLAN C: Facemask ventilation
Succeed
• If face-mask ventilation is impossible, administer Wake the patient up.
paralytic agents.
• For the final attempt at face-mask ventilation, use a Postoperative and follow-up care
two-person technique and adjuncts. • Formulate an immediate airway-management plan.
Declare “can’t intubate, can’t oxygenate” scenario • Monitor for complications.
• Complete an airway alert form.
PLAN D: Emergency front of neck access • Explain the process to the patient, both in
person and in writing.
Perform a scalpel cricothyroidotomy.
• Submit a written report to the patient’s primary
Adapted from Difficult Airway Society 2015 guidelines. care physician and the local database.
Passage difficult airway is anticipated, consider Once the tube has been passed, it
If an acceptable view of the vocal going straight to a bougie approach to should be secured, and postintubation
cords has been achieved but the tube increase the likelihood of success.68 sedation and ventilator management
remains difficult to pass, the clinician Clinicians should not assume that should ensue.
bougie “stoppage” or the ability to
can attempt a bougie intubation, try Summary
feel tracheal rings are signs of being
downsizing the tube, or try rotating
in the trachea; these “indications” RSI is a necessary skill in the
the tube counterclockwise so that the practice of emergency medicine. A
can be unreliable.70 Success can be
bevel faces posteriorly.67,68 A bougie can confirmed by visualizing the tube pass thorough understanding of proper
be used in several ways; clinicians are through the vocal cords, using end-tidal patient positioning, ideal oxygenation
encouraged to find the technique that capnography, and noting the presence of conditions, and optimal medication
works best for them, as no approach bilateral lung sounds and the absence of strategies provide the foundation for
has been shown to be superior.69 If a sounds in the stomach upon ventilation. a successful intubation. Practices that
are unsupported by the literature, such
as the application of cricoid pressure,
should be avoided.
Having a firm grasp of the
different tools available during
RSI, and understanding how that
n Placing patients in the ear-to-sternal-notch position provides the best
equipment works, allows emergency
chance for laryngoscopic success.
n All patients should be oxygenated via nasal cannula during the physicians to optimize their intubation
preoxygenation and apneic periods. attempts. Finally, having confidence in
n Ketamine is the preferred induction agent for patients in septic shock, as approaching the epiglottis-only view,
etomidate poses a potential risk of significant adrenal suppression. and having an algorithm at hand in the
n Rocuronium should be the paralytic of choice. Succinylcholine has many event that complications arise, affords
contraindications that can be problematic in the emergent setting, where a
the highest chance of success while
patient’s full history is not always known.
decreasing the risk of adverse outcomes.
December 2019 n Volume 33 Number 12 25
CASE RESOLUTIONS
■ CASE ONE ■ CASE TWO ■ CASE THREE
To stabilize the man with the The obese woman with a COPD Suspecting that the elderly man
suspected intracranial bleed, the exacerbation underwent RSI. She was was suffering from septic shock, the
physician proceeded with RSI. The kept on NIPPV for preoxygenation clinician delayed intubation until the
head of the bed was kept elevated, and patient’s hemodynamics could be
and was placed in a ramped position
the patient was placed in a position maximized. Three large-bore IV lines
to maximize the view of her
where his ears aligned with his were established. Despite being given
larynx. Etomidate and rocuronium
sternal notch. A nasal cannula was a 1-L bolus of normal saline, his blood
placed under the nonrebreather mask. were chosen as induction and
pressure failed to improve. He was
Fentanyl was used as a pretreatment paralytic agents, respectively. Video
started on vasopressors through an IV
agent to prevent a sympathetic laryngoscopy and a straight-to-cuff
line, and he was oxygenated via nasal
response to the intubation. stylet bent at 25 degrees were used to
cannula and a nonrebreather mask.
The clinician chose rocuronium maximize success.
In light of the mixed evidence
as a paralytic agent in order to During the initial attempt, an
regarding the use of etomidate in cases
avoid the potential increase in epiglottis-only view was encountered.
intracranial pressure associated of sepsis, the clinician used ketamine
The physician attempted to insert as an induction agent; rocuronium
with succinylcholine. After the
the laryngoscope blade further into was administered to avoid the life-
induction agent and paralytic were
the vallecula without success. With threatening risk of hyperkalemia
administered, the patient was bagged
for 45 seconds to prevent hypercapnia the help of an assistant, external associated with succinylcholine.
while the paralytic took effect. He laryngeal manipulation enabled The patient was intubated without
was successfully intubated on the first visualization of the cords and led to a difficulty, started on broad-spectrum
attempt. successful intubation. antibiotics, and admitted to the ICU.
REFERENCES
1. Sakles JC, Chiu S, Mosier J, Walker C, Stolz U. The 6. Weingart SD, Levitan RM. Preoxygenation and 11. Vourc’h M, Asfar P, Volteau C, et al. High-flow nasal
importance of first pass success when performing prevention of desaturation during emergency airway cannula oxygen during endotracheal intubation in
orotracheal intubation in the emergency department. management. Ann Emerg Med. 2012 Mar;59(3):165-175. hypoxemic patients: a randomized controlled clinical
Acad Emerg Med. 2013 Jan;20(1):71-78. 7. Lane S, Saunders D, Schofield A, Padmanabhan trial. Intensive Care Med. 2015 Sep;41(9):1538-1548.
2. Mort TC. Emergency tracheal intubation: R, Hildreth A, Laws D. A prospective, randomised 12. Ward JJ. High-flow oxygen administration by nasal
complications associated with repeated laryngoscopic controlled trial comparing the efficacy of cannula for adult and perinatal patients. Respir Care.
attempts. Anesth Analg. 2004 Aug;99(2):607-613. preoxygenation in the 20 degrees head-up vs. supine 2013 Jan;58(1):98-122.
3. Hasegawa K, Shigemitsu K, Hagiwara Y, et al; Japanese position. Anaesthesia. 2005 Nov;60(11):1064-1067. 13. Nimmagadda U, Salem MR, Joseph NJ, et al. Efficacy
Emergency Medicine Research Alliance Investigators. 8. Ramachandran SK, Cosnowski A, Shanks A, Turner CR. of preoxygenation with tidal volume breathing.
Association between repeated intubation attempts Apneic oxygenation during prolonged laryngoscopy Comparison of breathing systems. Anesthesiology.
and adverse events in emergency departments: an in obese patients: a randomized, controlled trial of 2000 Sep;93(3):693-698.
analysis of a multicenter prospective observational nasal oxygen administration. J Clin Anesth. 2010 14. Baraka AS, Taha SK, Aouad MT, El-Khatib MF,
study. Ann Emerg Med. 2012 Dec;60(6):749-754. May;22(3):164-168. Kawkabani NI. Preoxygenation: comparison of maximal
4. Greenland KB, Edwards MJ, Hutton NJ. External 9. Semler MW, Janz DR, Lentz RJ, et al. Randomized trial breathing and tidal volume breathing techniques.
auditory meatus-sternal notch relationship in adults in of apneic oxygenation during endotracheal intubation Anesthesiology. 1999 Sep;91(3):612-616.
the sniffing position: a magnetic resonance imaging of the critically ill. Am J Respir Crit Care Med. 2016 15. Russell T, Ng L, Nathan E, Debenham E.
study. Br J Anaesth. 2010 Feb;104(2):268-269. Feb;193(3):273-280. Supplementation of standard preoxygenation
5. Collins JS, Lemmens HJ, Brodsky JB, Brock-Utne JG, 10. Sakles JC, Mosier JM, Patanwala AE, Arcaris B, Dicken with nasal prong oxygen or machine oxygen flush
Levitan RM. Laryngoscopy and morbid obesity: a JM. First pass success without hypoxemia is increased during a simulated leak scenario. Anaesthesia. 2014
comparison of the “sniff” and “ramped” positions. with the use of apneic oxygenation during rapid Oct;69(10):1133-1137.
Obes Surg. 2004 Oct;14(9):1171-1175. sequence intubation in the emergency department. 16. Ruben H, Knudsen EJ, Carugati G. Gastric inflation
Acad Emerg Med. 2016 Jun;23(6):703-710. in relation to airway pressure. Acta Anaesthesiol
Scand.1961 Oct;5:107-114.
17. Bouvet L, Albert ML, Augris C, et al. Real-
time detection of gastric insufflation related to
facemask pressure-controlled ventilation using
ultrasonography of the antrum and epigastric
auscultation in nonparalyzed patients: a prospective,
randomized, double-blind study. Anesthesiology. 2014
Feb;120(2):326-334.
18. Brown, JP. Werrett G. Bag-mask ventilation in rapid
n Assuming that hovering a BVM above a patient’s face increases oxygen sequence induction. Anaesthesia. 2009 Jul;64(7):
delivery over room air; a tight seal is necessary. 784-785.
19. Robinson N, Clancy M. In patients with head injury
n Applying cricoid pressure to your patient. Studies show that this approach undergoing rapid sequence intubation, does
does not prevent aspiration and can actually worsen views during intubation. pretreatment with intravenous lignocaine/lidocaine
lead to an improved neurological outcome? A review of
n Failing to have an algorithm for the epiglottis-only view. The blade should first the literature. Emerg Med J. 2001 Nov;18(6):453-457.
be inserted further into the vallecula. If this doesn’t work, external laryngeal 20. Harris CE, Murray AM, Anderson JM, Grounds RM,
Morgan M. Effects of thiopentone, etomidate and
manipulation should be attempted, followed by a head lift. propofol on the haemodynamic response to tracheal
intubation. Anaesthesia. 1988 Mar;43:32-36.
26 Critical Decisions in Emergency Medicine
21. Stollings JL, Diedrich DA, Oyen LJ, Brown DR. 44. Drug Trial Snapshot: Bridion (sugammadex). https:// 65. Hwang J, Park S, Huh J, et al. Optimal external
Rapid-sequence intubation: a review of the process and www.fda.gov/drugs/drug-approvals-and-databases/ laryngeal manipulation: modified bimanual
considerations when choosing medications. drug-trial-snapshot-bridion Updated February 16, 2016. laryngoscopy. Am J Emerg Med. 2013 Jan;31(1):32-36.
Ann Pharmacother. 2014 Jan;48(1):62-76. Accessed November 12, 2019. 66. Law JA, Broemling N, Cooper RM, et al; Canadian
22. Ugur B, Ogurlu M, Gezer E, Nuri Aydin O, Gürsoy 45. Jahr JS, Miller JE, Hiruma J, Emaus K, You M, Airway Focus Group. The difficult airway with
F. Effects of esmolol, lidocaine and fentanyl on Meistelman C. Sugammadex: a scientific review recommendations for management—part 1—difficult
haemodynamic responses to endotracheal intubation: including safety and efficacy, update on regulatory tracheal intubation encountered in an unconscious/
a comparative study. Clin Drug Investig. 2007;27(4): issues, and clinical use in Europe. Am J Ther. 2015 induced patient. Can J Anaesth. 2013 Nov;60(11):
269-277. Jul-Aug;22(4):288-297. 1089-1118.
23. Kim WY, Kwak MK, Ko BS, et al. Factors associated 46. Bhatia N, Bhagat H, Sen I. Cricoid pressure: where 67. Johnson DM, From AM, Smith RB, From RP, Maktabi
with the occurrence of cardiac arrest after emergency do we stand? J Anaesthesiol Clin Pharmacol. 2014 MA. Endoscopic study of mechanisms of failure of
tracheal intubation in the emergency department. Jan;30(1):3-6. endotracheal tube advancement into the trachea
PLoS One. 2014 Nov 17;9(11):e112779. during awake fiberoptic orotracheal intubation.
47. Sellick BA. Cricoid pressure to control regurgitation
Anesthesiology. 2005 May;102(5):910-914.
24. Brown III CA, Walls RW. Airway. In: Marx JA, Hockberger of stomach contents during induction of anaesthesia.
RS, Walls RM, et al, eds. Rosens’ Emergency Medicine Lancet. 1961 Aug 19;2(7199):404-406. 68. Messa MJ, Kupas DF, Dunham DL. Comparison
Concepts and Clinical Practice. 8th ed. Philadelphia PA: of bougie-assisted intubation with traditional
48. Tsung JW, Fenster D, Kessler DO, Novik J. Dynamic
endotracheal intubation in a simulated difficult airway.
Elsevier Saunders; 2014:03-19. anatomic relationship of the esophagus and trachea
Prehosp Emerg Care. 2011 Jan-Mar;15(1):30-33.
25. Jabre P, Combes X, Lapostolle F, et al; KETASED on sonography: implications for endotracheal tube
confirmation in children. J Ultrasound Med. 2012 69. Baker JB, Maskell KF, Matlock AG, Walsh RM, Skinner
Collaborative Study Group. Etomidate versus ketamine
Sep;31(9):1365-1370. CG. Comparison of preloaded bougie versus standard
for rapid sequence intubation in acutely ill patients: a
bougie technique for endotracheal intubation
multicentre randomised controlled trial. Lancet. 2009 49. Smith KJ, Dobranowski J, Yip G, Dauphin A, Choi
in a cadaveric model. West J Emerg Med. 2015
Jul 25;374(9686):293-300. PT. Cricoid pressure displaces the esophagus: an Jul;16(4):588-593.
26. Price B, Arthur AO, Brunko M, et al. Hemodynamic observational study using magnetic resonance imaging.
70. Shah KH, Kwong BM, Hazan A, Newman DH, Wiener
consequences of ketamine vs etomidate for Anesthesiology. 2003 Jul;99(1):60-64.
D. Success of the gum elastic bougie as a rescue airway
endotracheal intubation in the air medical setting. 50. Rice MJ, Mancuso AA, Gibbs C, Morey TE, Gravenstein in the emergency department. J Emerg Med. 2011
Am J Emerg Med. 2013 Jul;31(7):1124-1132. N, Deittle LA. Cricoid pressure results in compression of Jan;40(1):1-6.
27. Shafer SL. Shock values. Anesthesiology. 2004 the postcricoid hypopharynx: the esophageal position
Sep;101(3):567-568. is irrelevant. Anesth Analg. 2009 Nov;109(5):1546-1552.
28. Hildreth AN, Mejia VA, Maxwell RA, Smith PW, Dart 51. Oh J, Lim T, Chee Y, et al. Videographic analysis of
BW, Barker DE. Adrenal suppression following a single glottic view with increasing cricoid pressure force.
dose of etomidate for rapid sequence induction: Ann Emerg Med. 2013 Apr;61(4):407-413.
a prospective randomized study. J Trauma. 2008 52. Tournadre JP, Chassard D, Berrada KR, Boulétreau P.
Sep;65(3):573-579. Cricoid cartilage pressure decreases lower esophageal
29. Duthie DJ, Frasier R, Nimmo WS. Effect of induction of sphincter tone. Anesthesiology. 1997 Jan;86(1):7-9.
anaesthesia with etomidate on corticosteroid synthesis 53. Fenton PM, Reynolds F. Life-saving or ineffective? An
in man. Br J Anaesth. 1985 Feb;57(2):156-159. observational study of the use of cricoid pressure and
30. Lundy JB, Slane ML, Frizzi JD. Acute adrenal maternal outcome in an African setting. Int J Obstet
insufficiency after a single dose of etomidate. J Anesth. 2009 Apr;18(2):106-110.
Intensive Care Med. 2007 Mar-Apr;22(2):111-117. 54. Trikha A, Vasudevan B. Cricoid pressure: time to
31. McPhee LC, Badawi O, Fraser GL, et al. Single-dose release the pressure! “The Indian Anaesthetists’ Forum
etomidate is not associated with increased mortality in website.”. http://180.149.244.185:9898/iaforum/Article_
ICU patients with sepsis: analysis of a large electronic Folder/Cricoid-Pressure-Time-to-Release-the-Pressure.
ICU database. Crit Care Med. 2013 Mar;41(3):774-783. pdf Published February 2015. Accessed November 12,
2019.
32. Chan CM, Mitchell AL, Shorr AF. Etomidate is
associated with mortality and adrenal insufficiency 55. Mechlin MW, Hurford WE. Emergency tracheal
in sepsis: a meta-analysis*. Crit Care Med. 2012 intubation: techniques and outcomes. Respir Care.
Nov;40(11):2945-2953. 2014 Jun;59(6):881-892.
33. Filanovsky Y, Miller P, Kao J. Myth: ketamine should not 56. Sakles JC, Mosier J, Chiu S, Cosentino M, Kalin L.
be used as an induction agent for intubation in patients A comparison of the C-MAC video laryngoscope to
with head injury. CJEM. 2010 Mar;12(2):154-157. the Macintosh direct laryngoscope for intubation in
the emergency department. Ann Emerg Med. 2012
34. Bozeman WP, Kleiner DM, Huggett V. A comparison
Dec;60(6):739-748.
of rapid-sequence intubation and etomidate-only
intubation in the prehospital air medical setting. 57. Amornyotin S, Prakanrattana U, Vichitvejpaisal P, Vallisut
Prehosp Emerg Care. 2006 Jan-Mar;10(1):8-13. T, Kunanont N, Permpholprasert L. Comparison of the
clinical use of Macintosh and Miller laryngoscopes for
35. Li J, Murphy-Lavoie H, Bugas C, Martinez J, Preston
orotracheal intubation by second-month nurse students
C. Complications of emergency intubation with
in anesthesiology. Anesthesiol Res Pract. 2010.
and without paralysis. Am J Emerg Med. 1999
Mar;17(2):141-143. 58. Arino JJ, Velasco JM, Gasco C, Lopez-Timoneda F.
Straight blades improve visualization of the larynx
36. Highlights of prescribing information: Zemuron while curved blades increase ease of intubation: a
(rocuronium bromide). Access data FDA. https:// comparison of the Macintosh, Miller, McCoy, Belscope
www.accessdata.fda.gov/drugsatfda_docs/label/ and Lee-Fiberview blades. Can J Anaesth. 2003
2010/020214s034lbl.pdf. Accessed November 12, 2019. May;50(5):501-506.
37. Tran DT, Newton EK, Mount VA, Lee JS, Wells GA, 59. Achen B, Terblanche OC, Finucane BT. View of the
Perry JJ. Rocuronium versus succinylcholine for rapid larynx obtained using the Miller blade and paraglossal
sequence induction intubation. Cochrane Database approach, compared to that with the Macintosh blade.
Syst Rev. 2015 Oct 29;(10):CD002788. Anaesth Intensive Care. 2008 Sep;36(5):717-721.
38. Martyn JA, Richtsfeld M. Succinylcholine-induced 60. Varghese E, Kundu R. Does the Miller blade truly
hyperkalemia in acquired pathologic states: etiologic provide a better laryngoscopic view and intubating
factors and molecular mechanisms. Anesthesiology. conditions than the Macintosh blade in small children?
2006 Jan;104(1):158-169. Paediatr Anaesth. 2014 Apr 2;24(8):825-829.
39. Gronert GA. Cardiac arrest after succinylcholine: 61. Passi Y, Sathyamoorthy M, Lerman J, Heard C, Marino
mortality greater with rhabdomyolysis than receptor M. Comparison of the laryngoscopy views with the
upregulation. Anesthesiology. 2001 Mar;94(3):523-529. size 1 Miller and Macintosh laryngoscope blades
40. Minton MD, Grosslight K, Stirt JA, Bedford RF. lifting the epiglottis or the base of the tongue in
Increases in intracranial pressure from succinylcholine: infants and children <2 yr of age. Br J Anaesth. 2014
prevention by prior nondepolarizing blockade. Nov;113(5):869-874.
Anesthesiology. 1986 Aug;65(2):165-169. 62. Asai T, Matsumoto S, Fujise K, Johmura S, Shingu K.
41. Taha SK, El-Khatib MF, Baraka AS, et al. Effect of Comparison of two Macintosh laryngoscope blades in
suxamethonium vs rocuronium on onset of oxygen 300 patients. Br J Anaesth. 2003 Apr 1;90(4):457-460.
desaturation during apnoea following rapid sequence 63. Delaney JS, Al-Kashmiri A, Baylis PJ, Aljufaili M, Correa
induction. Anaesthesia. 2010 Apr;65(4):358-361. JA. The effect of laryngoscope handle size on possible
42. Tang L, Li S, Huang S, Ma H, Wang Z. Desaturation endotracheal intubation success in university football,
following rapid sequence induction using ice hockey, and soccer players. Clin J Sport Med. 2012
succinylcholine vs. rocuronium in overweight patients. Jul;22(4):341-348.
Acta Anaesthesiol Scand. 2011 Feb;55(2):203-208. 64. Levitan RM, Pisaturo JT, Kinkle WC, Butler K, Everett
43. Strayer RJ. Rocuronium versus succinylcholine: WW. Stylet bend angles and tracheal tube passage
Cochrane synopsis reconsidered. Ann Emerg Med. using a straight-to-cuff shape. Acad Emerg Med. 2006
2011 Aug;58(2):217-218. Dec;13(12):1255-1258.
December 2019 n Volume 33 Number 12 27
Primetime
Viewing
Video Laryngoscopy
LESSON 6
By Samuel Kim, MD, Calvin A. Brown III, MD
and Alexander Y. Sheng, MD
Dr. Kim is an emergency medicine resident at Boston University Medical Center
in Boston, Massachusetts. Dr. Brown is assistant professor of emergency medicine
at Harvard Medical School, director of faculty affairs at Brigham and Women’s
Hospital Urgent Care, and an attending physician in the Department of Emergency
Medicine at Brigham and Women’s Hospital in Boston, Massachusetts. Dr. Sheng is
the assistant residency program director and an assistant professor in the Depart-
ment of Emergency Medicine, also at Boston University Medical Center.
Reviewed by Frank LoVecchio, DO, MPH, FACEP
OBJECTIVES
On completion of this lesson, you should be
able to:
1. Describe the major limitations of conventional direct
CRITICAL DECISIONS
laryngoscopy.
n What clinical presentations warrant the use of
2. List the advantages of video laryngoscopy for difficult
video laryngoscopy over direct laryngoscopy?
intubations.
3. Describe the major video laryngoscopes available and n When and how should video laryngoscopy
the design differences between each device. be used as a first-line instrument for airway
4. Explain the strengths and weakness of each of the management?
major video laryngoscopes.
n What technical challenges are of greatest
5. Apply video laryngoscopy in a variety of difficult airway
scenarios. concern when using video laryngoscopy?
n Do all VL models have emergency
FROM THE EM MODEL
department applications, and what are the
19.0 Procedures and Skills Integral to the Practice benefits and limitations of each?
of Emergency Medicine
19.4 Diagnostic and Therapeutic Procedures
19.4.4 Head, Ear, Eye, Nose, and Throat
March 2016 n Volume 30 Number 3 13
CASE PRESENTATIONS
■ CASE ONE ■ CASE TWO ■ CASE THREE
An 84-year-old woman with EMS arrives with a 91-year- A 42-year-old woman with facial
severe shortness of breath arrives via old man who has been transferred swelling and a history of hereditary
ambulance. She reports sudden-onset from an outside hospital. He was angioedema is brought to the emergency
chest pain at rest with progressive a restrained passenger in a motor department of a small community
dyspnea. Vital signs are blood pressure vehicle that rear-ended a bus at a hospital by EMS. Thirty minutes
122/56, a heart rate 99, and oxygen high rate of speed. EMS reports that before her symptoms began, she ate an
saturation 93% on non-rebreather he had to be extricated and appears omelet seasoned with a “new” type of
facemask. The patient is tachypneic to have an unstable C2 fracture and pepper. She immediately experienced
and in respiratory distress, using weakness in both of his arms. a tingling sensation in her face, which
accessory muscles to breathe. Her Upon arrival, the patient is supine has progressed to worsening facial,
jugular vein pulsations are elevated, on a stretcher and is wearing a periorbital, and lingual edema within the
and diffuse crackles and a 2/6 cervical collar. Vital signs are stable last hour.
systolic murmur are noted at the apex and he is conversant, in no obvious On arrival, she is afebrile. Vital signs
radiating to the axilla. distress, and complaining of neck are blood pressure 115/74; heart rate 89;
The patient has 1+ bilateral lower- pain. A secondary survey reveals and oxygen saturation 94% on room air,
extremity edema. An ECG shows tenderness to palpation on the which improved to 97% with an oxygen
lateral-wall STEMI, and a portable posterior midline of the man’s neck. facemask (reservoir at 15 L/min flow).
chest radiograph shows diffuse An outside cervical spine CT shows a Edema is apparent in her face, lips, and
pulmonary edema. Furosemide and displaced pedicle fracture of C2, and the area around her eyes. The patient’s
nitroglycerin are administered, and significant soft-tissue swelling from tongue is swollen, filling the majority of
she is placed on bilevel positive airway C2 down to C5. her oral cavity, and her voice is hoarse;
pressure (BI-PAP); however, she Shortly thereafter, the patient expiratory wheezing and stridor are noted.
continues to struggle. suddenly begins having difficulty While awaiting fresh frozen plasma
The emergency physician suspects speaking and breathing, and from the blood bank, antihistamines,
ischemic mitral regurgitation from complains of feeling “strangled.” steroids, and epinephrine are administered
papillary muscle rupture. Cardiology Within minutes, he appears to be without effect. C1 esterase-inhibitor
at the bedside recommends in respiratory distress. Suspecting concentrates are not readily available in
immediately catheterization. a retropharyngeal hematoma, this emergency department. Meanwhile,
Preparations are made to secure the the clinician decides to intubate the patient develops worsening stridor,
airway for impending respiratory emergently to secure airway voice changes, and decreasing oxygen
failure prior to percutaneous coronary protection. saturation on a non-rebreather mask. The
intervention. decision is made to intubate.
There is a rapidly growing body of other aspect of medicine has undergone patients remain difficult — or even im-
evidence to support the use of video dramatic advances in recent decades, possible — to intubate under direct vision.
laryngoscopy for the management of both however, DL largely has remained Many of these patients will require mul-
routine and difficult airways. Emergency unchanged. tiple attempts and prolonged intubation
physicians, in particular, must understand Direct visualization, which requires a times, which can put them at risk for dire
the design and clinical applications of straight line of sight from the operator’s traumatic and hypoxic consequences.
these devices to achieve improved first- eye to the glottic inlet, can be difficult Through improved glottic visual
pass success. or even impossible to acquire in many ization and user-friendly designs, video
All resuscitative efforts ultimately will emergency department patients. Cervical laryngoscopy (VL) has transformed
fail if the patient cannot be adequately spine precautions, reduced mouth our current understanding of what
oxygenated and ventilated. For the openings, small mandibles, airway constitutes a difficult-to-manage airway,
majority of those who are critically ill obstruction, blood, vomit, secretions, and has provided a new process for
or injured, this requires the successful and large tongues all contribute to poor overcoming these clinical challenges.
placement of an endotracheal tube (ETT). direct visualization. Over the past decade, advances in video-
Since it first was introduced in the early Some of these challenges can be over- enhanced devices have launched an
1940s, direct laryngoscopy (DL) has come with optimal patient positioning, “airway management revolution.”
been a reliable and successful method meticulous DL technique, and external Fundamentally, all video laryngoscopes
for obtaining glottic visualization and laryngeal manipulation. However, even possess the same critical design elements
tracheal intubation. While nearly every in the hands of a skilled operator, many that improve glottic visualization. Each
14 Critical Decisions in Emergency Medicine
device features a curved blade structure
with a narrow profile that can curl FIGURE 2. GlideScope AVL Reusable
around the tongue to mirror an oral
airway. Embedded along the curve of
the blade are a microcamera and light
source that enable glottic illumination
and the acquisition of an image that
then is displayed on a video screen. This
configuration allows the provider to “see
around corners” and obviates the need
for a direct line of sight — a critically
important benefit for many emergency
department patients.
CRITICAL DECISION
What clinical presentations
warrant the use of video
laryngoscopy over direct
laryngoscopy?
Difficult airway attributes are
common in emergency department
presentations, and poor glottic
visualization is among the most frequent
a difficult DL is predicted based on a in this regard.9 In emergency department
reasons why intubation attempts fail.
pre-intubation bedside assessment, VL populations, GlideScope use actually
Even with optimal positioning and
should be used as an immediate backup, appears to improve first-pass success.10,11
technique, patients with suboptimal
or even employed as the initial method of Some portable video laryngoscopes,
glottic views are good candidates for
intubation.4,5 including the GlideScope Ranger
video laryngoscopy.
(Figure 1), were created for prehospital
While we know what constitutes a CRITICAL DECISION scenarios; their compact size and
difficult DL attempt, the factors that
When and how should video specially designed screens function well
contribute to a problematic VL are still
laryngoscopy be used as a in high-glare environments. Although
unclear, as typical predictors of poor
real-life field experience is limited, these
direct visualization (restricted mouth first-line instrument for airway
tools have been successfully integrated
opening, reduced neck mobility, anterior management? into both ground and air-transport
airways, etc.) do not necessarily portend
Although video laryngoscopes have prehospital settings.
poor video views.1-3
been successful in “rescuing” poor direct In the hands of ground personnel, the
There is a growing body of
views, there is little evidence about GlideScope Ranger shows improved rates
literature that supports the superiority
whether these devices should be used of success, fewer attempts, and a shorter
of glottic views with VL in both
for routine intubations, or reserved for time to intubation and ventilation
operative and emergency department
difficult or failed airways.6 While the compared to DL.12 Conversely, the
patients. Research suggests that when
focus has been on showing how VL Pentax Airway Scope (AWS) has
can “backup” DL, video laryngoscopy demonstrated inferior intubation success
FIGURE 1. GlideScope Ranger is gaining traction as a viable stand- rates when used in daylight environments
alone option that can be employed in because of screen glare.13
virtually any clinical situation. Recent
registry data suggests that VL is being CRITICAL DECISION
used nearly as often as DL for emergency What technical challenges are
department intubations.7 of greatest concern when using
Although VL improved visualization,
video laryngoscopy?
early experience with GlideScope
laryngoscopy suggested that it might not Most video laryngoscopes are user-
improve first-pass intubation success or friendly; however, transitioning from
time to tube placement.8 These results tube placement under direct visualization
may have been confounded by the to intubation by indirect vision may be
intubators’ inexperience. In adept, well- difficult for some operators. Devices
trained hands, VL is comparable to DL with integrated tube channels, including
March 2016 n Volume 30 Number 3 15
CRITICAL DECISION a rigid stylet, which should be used to
FIGURE 3. Storz C-MAC maintain ETT shape during intubation
Do all VL models have
by allowing the tube to follow the curved
emergency department trajectory of the blade without becoming
applications, and what are the deformed.
benefits and limitations of each? The GlideScope Cobalt AVL (Figure
2) is a disposable, single-use system that
GlideScope Video circumvents the cost and downtime
Laryngoscope associated with the maintenance and
Anatomy disinfection of the original model. Both
pediatric and standard-sized wands are
The GlideScope Video Laryngoscope
available.
(GVL), which has been on the market for
The GlideScope Ranger is a
more than a decade, is the prototypical
lightweight, portable version originally
VL model. The standard GVL system
designed for field use. The handle, cable,
consists of a curved Macintosh-like
and display are built into one self-
blade; its 80-degree hyperacute anterior
contained unit, and its 3.5-inch LCD
angulation curves around the tongue.
screen remains visible despite sun glare.
LED lights are positioned along the
underbelly of the blade with a video Devices in the GlideScope family
the Pentax Airway Scope, initially may also include a steel video blade with
camera that utilizes complementary
be easier to learn than the Macintosh metal-oxide semiconductor (CMOS) geometry similar to that of direct
blade.14 technology. A light source is placed in laryngoscopes. This “direct intubation
More practice may be required with close proximity to a rectangular glass trainer” is designed to allow the operator
devices that require the ETT to be placed window, enabling the LEDs to warm the to maintain skill with conventional DL
independently by hand (eg, GlideScope lens to prevent misting and fogging (a mechanics, while benefitting from video
or McGrath). The curved trajectory of common problem with such devices). enhancements that facilitate real-time
the ETT as it approaches the laryngeal A single video cable transmits instructor feedback. The most recent
processed images to a 7-inch LCD GlideScope iteration features a thin
inlet can make navigation of the cords
display, which can be placed on a titanium profile and disposable high-
challenging.15
flat surface or mounted to a mobile grade plastic blades.
VL offers superior glottic exposure
over DL in nearly every scenario. stand and brought to the bedside. The Technique
However, devices with distal image original GVL blade comes in a variety Limited by its shape and design, the
acquisition are susceptible to soiling of shapes and sizes (GVL-2 through GlideScope does not function and should
GVL-5) suitable for virtually any patient not be used as a direct laryngoscope.
by airway bleeding and secretions,
population — from small children to Like all such devices, the GlideScope is
which can make it difficult to maintain
adults with physical limitations such as a left-handed instrument. After opening
adequate visualization. To achieve
morbid obesity. the patient’s mouth, the blade should be
indirect visualization of the laryngeal
Most average-sized adults can be inserted directly in the midline with the
inlet and vocal cords, the ETT must intubated with a size 3 or 4 blade.
follow the same trajectory of the blade as top surface of the blade touching, but
Standard GVL blades are reusable; after not manipulating, the tongue. While the
it approaches the airway. each intubation, they must undergo patient can be placed in the “sniffing
Since this path follows a steep cleaning to remove gross debris, as well position,” this is not required.
arc and not a straight line, it can be as high-level disinfection. The handle, With an eye on the screen, the
difficult to navigate the vocal cords made of high-grade medical plastic, is intubator should guide the distal tip
with the tube tip; the stylet often must submersible. of the blade around the tongue while
be retracted to complete the intubation. Every GlideScope system includes watching for key midline structures,
This unique extra step can result in a including the uvula and the tip of the
slightly prolonged time to tracheal tube epiglottis. The blade tip should be
placement, although it does not affect TABLE 1. Upper Lip Bite Test
maneuvered into the vallecula and then
intubation success.13 According to a Class I: Lower incisors can bite the a gentle backward lift should be used to
recent study, predictors of difficult VL upper lip above the vermilion line. expose the laryngeal inlet.
include patients with poor upper lip Class II: Lower incisors can bite the A common mistake is to advance
bite tests (Table 1), although the study upper lip below the vermilion line. the blade too far into the hypopharynx,
only included subjects with grade I or Class III: Lower incisors cannot bite which results in an “up-close” image
II Cormack and Lehane (C-L) glottic the upper lip. of the vocal cords that appears highly
views.16 optimized; in reality, however, the
16 Critical Decisions in Emergency Medicine
blade may be too close and incorrectly of the ETT flexible, enabling it to pass In a recent study aimed at identifying
positioned in the laryngeal inlet. easily into the trachea. the clinical features associated with
Ultimately, the blade competes for The device is appropriate as a primary difficult GlideScope laryngoscopy,
the same space as the approaching ETT, intubation tool, although it traditionally patients with high upper lip bite
making tube delivery exceptionally has been reserved for cases that are test scores and short sternothyroid
difficult. The tip of the ETT should be difficult or impossible to complete distances required multiple attempts or
inserted in the corner of the right side under direct vision. The minimal force lengthier intubation times. Despite these
of the patient’s mouth, with the tube required to expose the glottis makes complications, a grade I or II view was
parallel to the ground. As the tube is the GlideScope useful for patients in obtained in every patient (all of whom
advanced behind or adjacent to the blade C-spine immobilization. Its sharp distal were undergoing general anesthesia).16
and its distal tip guided toward the tip angulation allows better visualization of In the hands of prehospital providers,
of the laryngoscope, the user should the anterior larynx. the GlideScope also has been associated
look at the screen while rotating the tube with improved intubation success (97%
counterclockwise 90 degrees. (The tip
Evidence
compared to 95% with DL), fewer
of the ETT should be held at 12 o’clock, Among inexperienced operators, the
attempts (1.2 versus 2.3), less time
positioned in front of the laryngeal inlet device is able to provide a C-L grade I or
without ventilation (37 seconds versus
curving into the trachea.) II view in nearly every patient in which
55 seconds), and shorter time to
Under real-time video supervision, its used, with glottic visualization equal
intubation (21 versus 42 seconds).12
the operator should advance the to or better than DL. Although rare,
ETT through the vocal cords while failures can occur due to the difficulty Storz C-MAC
simultaneously withdrawing the of passing the ETT, despite a sufficient Anatomy
stylet by about 5 cm to complete the glottic view.17
The Storz C-MAC (Figure 3) is
intubation. Withdrawal, which can be Success with this device is high (96%
a reincarnation of the older video
done by the operator’s thumb or by an to 98%), even in patients who exhibit
Macintosh laryngoscope (V-MAC).
assistant, should follow the arc of the hallmarks of difficult laryngoscopy
While the video Macintosh was a hybrid
instrument, eventually curving into the (eg, those with morbid obesity, cervical
scope that combined both fiberoptic and
patient’s chest. spine disease, or a cervical collar). The
video elements, the C-MAC utilizes a
Obtaining an optimal view of the device performs equally well compared
CMOS chip technology similar to that
glottis with the GlideScope is rarely to flexible bronchoscopes in morbidly
used in the GlideScope.
difficult. However, passage of the ETT obese patients.29 The GlideScope also
The device’s shape is that of
through the glottis while observing has shown promise as a rescue device,
a traditional direct Macintosh
the screen can be challenging for two succeeding in 94% of intubations where
laryngoscope. A newer hyperangulated
reasons. First, some familiarity with the DL failed. Evidence of altered upper-
blade (called the “D-blade” or difficult
instrument is required. Second, due to airway anatomy or head and neck
blade) recently has been designed to help
the hyperangulation of the GlideScope surgery appear to be the only predictors
visualize a more anterior and superior
blade, the tip of the ETT must follow the of GlideScope difficulty.18 The device’s
larynx. A micro camera and light source
same path with an anterior trajectory only limitation is that the patient’s
are blended into the blade; and a video
that can impinge on the trachea at mouth opening must be greater than
cartridge slips into the back of the
a sharp angle and fail to advance. 15 mm to accommodate the passage of
handle, attached by a single cord to a
Withdrawal of the stylet makes the end the widest portion of the blade.
high-resolution digital display that can
sit on a flat surface or mount to a mobile
FIGURE 4. McGrath Series 5 pole.
The blades intrinsically possess
anti-fog properties (the light source is
contained in the blade itself, warming
the lens), and the monitor system can
record both still images and video clips.
Technique
Since the standard C-MAC
blades feature Macintosh geometry,
the mechanics of laryngoscopy are
more akin to that of DL. Because of
this, the trajectory to the airway is
straighter, which can help facilitate
the manipulation of the ETT tip to
the laryngeal inlet. While it is possible
March 2016 n Volume 30 Number 3 17
curved video wand (called a “Camera
Stick”) houses the light source with a
single-use disposable hard plastic blade.
The McGrath’s main advantage is its
portability; it weighs only 325 grams,
and requires neither cables nor a separate
n Use a rigid stylet when intubating with the GlideScope; this can help the display unit. However, the device’s small
ETT navigate the sharper anterior angulation of the blade to reach the size can make it vulnerable to theft and
laryngeal inlet.
damage during transport. The video
n If maintaining DL skill is important in your practice, consider using a wand and blade cover are fully adjustable
C-MAC blade, which maintains standard Macintosh geometry and can be to three different lengths.
used when DL mechanics are desired. The newest version of the device
n Consider VL as the initial method for routine and difficult intubations, includes a slightly larger screen and an
and be familiar with the specific devices available in your emergency angled blade designed for both video and
department. direct viewing. However, when used as
n Devices with plastic covers that go over or envelop the video and light a direct laryngoscope, the device may
elements (eg, C-MAC, GlideScope Cobalt, McGrath Series 5) are prone to not provide adequate direct views of the
fogging. Either warm the device or apply a commercial anti-fog solution glottic inlet.24
prior to the intubation attempt.
Technique
Much like the GlideScope, the
“good” glottic views (C-L grade I or II) McGrath is designed to be inserted in
to intubate without one, a malleable
compared to DL. Of the patients with the midline and “hugged” around the
stylet should be used for the majority of
an initial grade IV direct view, a grade tongue, while being rotated backwards
emergency tracheal intubations; rigid
I or II video view was obtained nearly until the glottis can be visualized. The
stylets are unnecessary.19
80% of the time. This data also supports tip of the blade should be positioned in
When using the C-MAC, the operator
the argument that early recourse to the vallecula. A slight upward lift may
can either insert the blade as if using
VL should be considered when glottic be required to expose the glottis. A
a conventional direct laryngoscope,
visualization is suboptimal.20 malleable stylet with a curve that follows
or place the blade in the midline and
Video laryngoscopes also provide the arc of the blade should be used within
advance it using a GlideScope-like
gentler intubation attempts since less the tracheal tube to maintain its shape.
technique. With its anti-fog features,
wider field of view, ease of use, and effort is required to obtain an acceptable Evidence
mobility, the C-MAC has become view. The force exerted on the maxillary
Although not as extensively studied
particularly popular in emergency incisors by the V-MAC is less than that
as the GlideScope, the McGrath has
department settings. associated with a standard Macintosh
performed well in operative reports,
blade (2.1 N versus 15.3 N).21
Evidence obtaining a C-L grade I or II view in
As with the GlideScope, the V-MAC
99% of subjects.25 The model also may
Because the C-MAC is a newer allows trainees to view the procedure on
be a particularly valuable rescue tool
device, it has yet to collect the robust the screen in real time — a benefit that
after DL has failed. In one operative
body of evidence seen with the can improve the intubation process and
study of patients undergoing general
GlideScope; however, early studies are reduce the learning curve.22 Preliminary
anesthesia with unsuccessful DL, the
encouraging. In one dual-center study, experience with the C-MAC shows
McGrath successfully intubated patients
V-MAC laryngoscopy succeeded in it performs on par with other video
producing the best attainable direct 95% of the time (58/61).9 As with other
laryngoscopes in its class. The device
and video view and a higher number of also may provide better first-pass success video laryngoscopes, novice clinicians
(93% versus 84%) in predicted difficult may take longer to intubate when using
airways.23 the instrument than when using DL — a
FIGURE 5. Pentax Airway Scope caveat that reflects the additional skill
McGrath Series 5 required to indirectly navigate the ETT
Anatomy through the vocal cords.26
Compact and lightweight, the The Pentax Airway Scope
McGrath Series 5 video laryngoscope
features a 1.7-inch integrated LCD
(AWS-100)
screen mounted on the end of its handle Anatomy
(Figure 4). The monitor pivots and is The portable, self-contained Pentax
adjustable to maintain optimal viewing Airway Scope includes a video camera,
during different phases of insertion. A 2.4-inch LCD rectangular display,
18 Critical Decisions in Emergency Medicine
disposable blade, and tube holder (Figure for secretions and blood to contaminate to view in bright light, can result in
5). While the design is similar to that the device’s optics can compromise harder and longer intubation attempts in
of other video laryngoscopes, several visualization during intubation. outdoor daylight settings.13
unique features are worth noting. Green
“crosshairs” on the display allow the
Technique King Vision
Much like other video laryngoscopes, Anatomy
operator to properly position the device;
the AWS is advanced in the midline after The King Vision video laryngoscope
when the ETT is advanced, it is more
the vocal cords have been positioned in is among the newest devices on the
likely to traverse the laryngeal opening
the target site.
into the trachea. market. Introduced in late 2011, it
The device’s handle is attached to a Evidence incorporates a reusable monitor and
flexible video/light wand that fits inside In 100 elective surgery patients, stalk, which fit into a disposable plastic
a disposable plastic sheath and provides the Pentax AWS obtained a grade I handle containing both video and light
a 90-degree field of view. The blade, view in all cases, while the Mac blade elements. The tool features a 24-inch
made from fog- and contamination- achieved this only 65% of the time. diagonal monitor with a full-color,
resistant Lexan plastic, incorporates The integrated channel, as opposed OLED anti-glare display that provides a
a tracheal channel that holds the tube to freehanding, may result in faster 160-degree viewing angle (Figure 6).
during insertion and facilitates its times to intubation compared to the Its handle is ergonomically designed
passage during intubation. The channel GlideScope in patents with normal to reduce the impact on teeth and
can accommodate tubes with internal airway anatomy. 27 prevent the lift of soft tissue. The
diameters from 6.0 to 8.5 mm. The Pentax also shows encouraging device’s disposable blades feature
Durable and highly water-resistant, results in patients at risk for cervical coated, anti-fog lenses; CMOS chips;
the AWS-S100 model is particularly spine injury.28 Even in the hands of novice micro cameras; and white LED lights.
useful in outdoor prehospital operators, intubation with the Pentax Ultra-portable and water resistant, the
environments. However, the lack of a may be faster and more successful than device is highly adaptable to prehospital
robust anti-fog mechanism and tendency with DL.14 The screen, which is difficult environments.
CASE RESOLUTIONS
■ CASE ONE GlideScope, which provided a full- patient was intubated successfully with
grade I Cormack-Lehane glottic view, a 7-0 ETT on first attempt using the
Airway equipment was prepared
despite the patient’s rigid TMJ. video view.
at the bedside to intubate the elderly
A 7.5-mm ETT was passed through
woman with STEMI, including size-3
the cords under video visualization and
■ CASE THREE
Macintosh and Miller blades, and a When preparing equipment to
secured, and the patient was taken to
GlideScope video laryngoscope and intubate the 42-year-old woman with
the catheterization lab for definitive
bougie as backups. The patient was angioedema, the emergency physician
treatment of a ST-segment elevation
preoxygenated with BL-PAP with a discovered that the fiberoptic broncho-
myocardial infarction.
starting oxygen saturation of 97%. scope normally available had been sent
Etomidate (10 mg) and succinyl ■ CASE TWO for repairs. The clinician adjusted his
choline (100 mg) were administered The emergency physician anticipated plan to attempt an awake look with a
intravenously. Fasciculations appeared intubation difficulties in the elderly King Vision video laryngoscope, while
30 seconds later with flaccid paralysis car accident victim. Anesthesia was simultaneously preparing for an
at 50 seconds. The emergency notified, but could not spare any emergent bedside cricothyroidotomy.
physician’s first direct look with the personnel. The patient began to A benzocaine 20% metered spray
Mac 3 provided a C-L grade III view; deteriorate. with atomizer was used to desensitize
it became apparent that the patient A topical anesthesia with nebulized the posterior pharynx. The King
suffered from advanced degenerative and atomized lidocaine was applied, Vision was inserted with the patient
temporomandibular joint (TMJ), which and ketamine (0.5 mg/kg) was sitting upright. A C-L grade II view
limited the opening of her mouth. The administered intravenously. A backup was achieved; and, despite significant
view was not improved, even with use cricothyroidotomy kit was prepared. supraglottic swelling, a 7-0 ETT was
of the Miller blade and backwards, Intubation was attempted with a successfully placed. The patient was
upwards, rightwards pressure. C-MAC video laryngoscope. A direct immediately sedated with propofol.
The patient desaturated, but was look failed to visualize any glottis Fresh frozen plasma arrived minutes
successfully bagged and preoxygenated. structures; however, a grade IIa view later, and the patient was admitted to
A second attempt was made with the was achieved on the video screen. The the ICU.
March 2016 n Volume 30 Number 3 19
versus direct laryngoscopy intubation in the
emergency department. Acad Emerg Med.
2009;16(9):866-871.
9. Noppens RR, Möbus S, Heid F, et al. Evaluation of
the McGrath Series 5 videolaryngoscope after failed
direct laryngoscopy. Anaesthesia. 2010;65(7):716-720
10. Sakles JC, Mosier JM, Chiu S, Keim SM. Tracheal
intubation in the emergency department: a
comparison of GlideScope® video laryngoscopy to
direct laryngoscopy in 822 intubations. J Emerg Med.
n Failing to practice the techniques for tube delivery with video 2012;42(4):400-405.
laryngoscopy, which requires different hand-eye coordination, stereotactic 11. Mosier JM, Stolz U, Chiu S, Sakles JC. Difficult
airway management in the emergency department:
skills, and experience than with DL. GlideScope videolaryngoscopy compared to direct
laryngoscopy. J Emerg Med. 2012;42(6):629-634.
n Advancing a video laryngoscope too deeply. This can result in a 12. Wayne MA, McDonnell M. Comparison of traditional
disorienting view of the esophageal opening, which is created when the versus video laryngoscopy in out-of-hospital tracheal
intubation. Prehosp Emerg Care. 2010;14(2):278-282.
camera is directed posterior to the laryngeal inlet.
13. Ueshima H, Asai T. Tracheal intubation in daylight
n Intubating without a stylet or with the wrong stylet. and in the dark: a randomised comparison of the
Airway Scope, Airtraq, and Macintosh laryngoscope
n Attempting to intubate without maintaining a curve on the tracheal tube; in a manikin. Anaesthesia. 2010;65(7):684-687.
14. Liu L, Tanigawa K, Kusunoki S, et al. Tracheal
this mistake will make the procedure challenging or even impossible. intubation of a difficult airway using Airway Scope,
Airtraq, and Macintosh laryngoscope: a comparative
manikin study of inexperienced personnel. Anesth
Analg. 2010;110(4):1049-1055.
Technique we should relegate them to this role. 15. Walls RM, Samuels-Kalow M, Perkins A. A new
maneuver for endotracheal tube insertion during
The King Vision should be introduced Trauma, bleeding, and airway difficult GlideScope intubation. J Emerg Med.
into the patient’s mouth in much the swelling will occur with serial 2010;39(1):86-88.
16. Tremblay MH, Williams S, Robitaille A, Drolet P. Poor
same way it is with the GlideScope laryngoscopy attempts. Each device has visualization during direct laryngoscopy and high
upper lip bite test score are predictors of difficult
and Pentax AWS. Once fully inserted, its advantages and disadvantages, and intubation with the Glidescope videolaryngoscope.
slight upward force may be required the final choice will depend on practice Anesth Analg. 2005;106(5):1495-1500.
17. Cooper RM, Pacey JA, Bishop MJ, McCluskey
to optimize the glottic view. If using a setting, departmental budgets, provider SA. Early clinical experience with a new video
channeled blade, the tube simply can be preference, and the ability to reprocess laryngoscope (GlideScope) in 728 patients. Can J
Anaesth. 2005;52(2):191-198.
pushed forward while the glottic opening reusable equipment. However, one thing 18. Aziz MF, Healy D, Kheterpal S, et al. Routine clinical
is kept in the middle of the screen. is clear — when available, VL is quickly practice effectiveness of the Glidescope in difficult
airway management: an analysis of 2,004 Glidescope
becoming standard care. intubations, complications, and failures from two
Alternatively, a preformed stylet and institutions. Anesthesiology. 2011;114(1):34-41.
For the same reason we’ve moved
ETT can be “freehanded” to complete 19. van Zundert A, Maassen R, Lee R, et al. A Macintosh
away from ordering oral contrast laryngoscope blade for videolaryngoscopy reduces
the intubation. stylet use in patients with normal airways. Anesth
dye studies to diagnose appendicitis Analg. 2009;109(3):825-831.
Innovative, lightweight, compact, and
or performing diagnostic peritoneal 20. Brown CA 3rd, Bair AE, Pallin DJ, et al. Improved
affordable, the device includes the design glottic exposure with the video Macintosh
lavage for unstable trauma patients, we laryngoscope in adult emergency department
elements that have proved successful tracheal intubations. Ann Emerg Med. 2010;56(2):83-
should begin to migrate away from DL. 88.
in other VL models. Although formal
Although DL represents “the way we’ve 21. Lee RA, van Zundert AA, Maassen RL, et al. Forces
studies are lacking, promising research is applied to the maxillary incisors during video-assist-
always done it,” we must now perform ed intubation. Anesth Analg. 2009;108(1):187-191.
underway.
intubation “the way it should be done.” 22. Kaplan MB, Ward DS, Berci G. A new video
laryngoscope—an aid to intubation and teaching.
Summary J Clin Anesth. 2002;14(8):620-626.
VL is changing the landscape of REFERENCES 23. Aziz MF, Dillman D, Fu R, Brambrink AM.
Comparative effectiveness of the C-MAC video
emergency airway management. DL is 1. Walls RM. Identification of the Difficult and laryngoscope versus direct laryngoscopy in
Failed Airway. In: Manual of Emergency Airway the setting of the predicted difficult airway.
a time-tested technique that relies on Management, 3rd Ed. LW&W; 2008:81-93. Anesthesiology. 2012;116(3):629-636.
2. Reed MJ, Dunn MJ, McKeown DW. Can an airway 24. Wallace CD, Foulds LT, McLeod GA, et al. A
an outdated tool. Video laryngoscopes assessment score predict difficulty at intubation comparison of the ease of tracheal intubation
are highly successful, easy to use, in the emergency department? Emerg Med J. using a McGrath MAC® laryngoscope and a
2005;22(2):99-102. standard Macintosh laryngoscope. Anaesthesia.
and improve glottic visualization in 3. Hagiwara Y, Watase H, Okamoto H, et al. Prospective 2015;70(11):1281-1285.
validation of the modified LEMON criteria to predict 25. Shippey B, Ray D, McKeown D. Case series: the
almost every conceivable scenario. The difficult intubation in the ED. Am J Emerg Med. McGrath videolaryngoscope—an initial clinical
combination of improved visualization, 2015;33(10):1492-1496. evaluation. Can J Anaesth. 2007;54(4):307-313.
4. Kaplan MB, Hagberg CA, Ward DS, et al. 26. Walker L, Brampton W, Halai M, et al. Randomized
high first-pass success and gentler Comparison of direct and video-assisted views of controlled trial of intubation with the McGrath
the larynx during routine intubation. J Clin Anesth.
attempts undoubtedly will translate 2006;18(5):357-362.
Series 5 videolaryngoscope by inexperienced
anaesthethists. Br J Anaesth. 2009;103(3):440-445.
into a safer, more reliable intubation 5. Sakles JC, Mosier J, Chiu S, et al. A comparison of 27. Teoh WH, Shah MK, Sia AT. Randomised comparison
the C-MAC video laryngoscope to the Macintosh of Pentax AirwayScope and Glidescope for tracheal
experience for the patient and provider. direct laryngoscope for intubation in the emergency intubation in patients with normal airway anatomy.
In modern medicine, these devices department. Ann Emerg Med. 2012;60(6):739-748. Anaesthesia. 2009;64(10):1125-1129.
6. Piepho T, Fortmueller K, Heid FM, et al. Performance 28. Liu EH, Goy RW, Tan BH, Asai T. Tracheal intubation
help facilitate airway management of the C-MAC video laryngoscope in patients after with videolaryngoscopes in patients with cervical
a limited glottic view using Macintosh laryngoscopy.
education, quality assurance, and Anaesthesia. 2011;66(12):1101-1105
spine immobilization: a randomized trial of the
Airway Scope and the GlideScope. Br J Anaesth.
research through their ability to record 7. Brown CA 3rd, Blair AE, Pallin DJ, et al. Techniques, 2009; [e-pub ahead of print]. Available at: http://
success, and adverse events of emergency dx.doi.org/10.1093/bja/aep164.
still images and videos. While they department adult intubations. Ann Emerg Med, 29. Abdelmalak BB, Bernstein E, Egan C, et al.
2015;65(4):363-370.e1.
traditionally have been thought of as GlideScope® vs flexible fibreoptic scope for
8. Platts-Mills TF, Campagne D, Chinnock B, et al. A elective intubation in obese patients. Anaesthesia.
“rescue” tools, there is no evidence that comparison of GlideScope video laryngoscopy 2011;66(7):550-555.
20 Critical Decisions in Emergency Medicine
Down the Tube
Postintubation Care
of the Critically Ill
LESSON 12
By Matthew A. Roginski, MD, MPH; Christopher J. Hogan, MD,
FACEP, FCCM; and Michael G. Buscher, DO, FAAEM
Dr. Roginski is the assistant medical director of DHART and an assistant professor
of medicine in the Sections of Emergency and Critical Care Medicine at Dartmouth-
Hitchcock Medical Center in Lebanon, New Hampshire. Dr. Hogan is an associate
professor in the Departments of Emergency Medicine and Surgery at Virginia
Commonwealth University Medical Center in Richmond. Dr. Buscher is an attending
physician in the Departments of Emergency Medicine and Internal Medicine (Critical
Care) at Yale New Haven Health, Bridgeport Hospital in Bridgeport, Connecticut.
Reviewed by George Sternbach, MD, FACEP
OBJECTIVES
On completion of this lesson, you should be able to: CRITICAL DECISIONS
1. Discuss how to choose an initial ventilator setting, and n What factors should be considered when choosing
describe techniques for evaluating complications like a patient’s initial ventilator settings, and how
air trapping and high alveolar pressures.
should potential complications be avoided?
2. Summarize the ideal sedative and analgesic agents for
intubated patients. n What sedatives and analgesic agents are preferred
3. Identify hemodynamically unstable postintubation for intubated patients in the ED?
patients using invasive and noninvasive measures. n What is the best approach for assessing and
4. Recognize and manage deadly postintubation managing hemodynamic instability?
pathologies. n How should metabolic derangements be managed?
5. Identify acute interventions to limit the risk of ventilator-
n What causes of postintubation cardiac arrest
associated pneumonia.
should emergency physicians be prepared to
FROM THE EM MODEL address?
19.0 Procedures and Skills Integral to the Practice n What can be done to decrease the risk of
of Emergency Medicine ventilator-associated pneumonia?
19.1 Airway Techniques
Given the escalating number of high-acuity cases and frequency of prolonged boarding, intubated patients
must often be managed in the emergency department for extended periods. Although most emergency
physicians are highly skilled in emergent airway management, they must also be adept at performing various
mechanical ventilation techniques, following sedation and analgesia regimens, and treating the complex acid base
and hemodynamic derangements that many of these patients exhibit.
June 2020 n Volume 34 Number 6 17
CASE PRESENTATIONS
■ CASE ONE ■ CASE TWO ■ CASE THREE
A 31-year-old man presents A 38-year-old woman arrives A 74-year-old man with oxygen-
in respiratory distress; he is blue via ambulance after being found dependent emphysema presents from
unresponsive by her roommate, who a local nursing home in respiratory
and unresponsive. His vital signs
says the patient has a history of distress. His caregiver reports that he
are blood pressure 180/90, heart
depression and recently underwent a has been febrile and more confused
rate 125, and oxygen saturation
breakup. EMS reports that the patient recently with increased sputum
83% with minimal lung sounds on
was unresponsive, tachypneic (40 bpm), production. When EMS arrived,
examination. His wife frantically tachycardic (145 bpm), hypotensive he was sitting upright in bed, in a
explains that the patient is healthy (88/40 mm Hg) and febrile (38.4°C tripod position and in significant
at baseline with the exception of [101.1°F]) at the scene. distress. They promptly placed him on
sleep apnea and nasal polyps. He Upon arrival, the patient is continuous positive airway pressure
was diagnosed with an upper- unresponsive and tachypneic, localizing (CPAP), nebulized albuterol, and IV
respiratory infection earlier this to painful stimuli. Her oxygen methylprednisolone.
week, but his symptoms have saturation is 99% on room air, and her Upon arrival, the patient is in
worsened today. blood glucose level is 130 mg/dL. After respiratory distress and remains
being preoxygenated, she is sedated hypoxic on CPAP. His initial vital signs
The patient is intubated but is
and paralyzed with etomidate and are blood pressure 100/60, heart rate
difficult to ventilate with a bag-
rocuronium, respectively. The patient 110, respiratory rate 40, and oxygen
valve-mask. Once on a ventilator,
is intubated with a 7.5-endotracheal saturation 84%. After an additional
his peak pressures reach 78 cm tube (ETT); her vocal cords are albuterol nebulizer is administered
H 2 0. His arterial blood gas (ABG) visualized, and a positive color change through the CPAP, a chest x-ray shows
measurement includes a pH of 7.12 is noted on capnography. As the ETT is hyperinflated lungs with bilateral infil
and partial pressure of carbon being secured, she begins to seize and trates. The decision is made to perform
dioxide (pCO 2) of 81 mm Hg. becomes hypoxic. a rapid-sequence intubation (RSI).
CRITICAL DECISION Volume Control patient without active respiratory effort,
For patients without evidence of plateau pressure (Figure 1) should be
What factors should be
lung injury, a targeted tidal volume of measured at the end of inspiration.
considered when choosing When flow in the airways approach zero,
6 to 8 mL/kg of predicted body weight
a patient’s initial ventilator is safe place to start. Recent research the pressure equilibrates throughout
settings, and how should shows that low tidal volume ventilation the circuit, and the plateau pressure
potential complications be reduces the risk of lung injury and acute represents the pressure in the alveoli.
avoided? respiratory distress syndrome (ARDS) in The aim is to keep plateau pressure
patients with normal-appearing lungs.1-3 under 30 cm H2O to avoid barotrauma.
Managing the ventilator of a newly
If evidence of a lung injury is present at The etiology of elevated plateau
intubated emergency department patient
the time of intubation, it is important to pressures is multifactorial; it can result
is an active process, and every decision
reduce tidal volumes to 6 mL/kg of ideal from a combination of increased volume
has downstream effects on morbidity
body weight. This strategy can improve and alveolar overdistention, reduced
and mortality.1,2 The goal of ventilatory
outcomes in patients with ARDS.4 chest wall compliance, or abdominal
management is to provide support and
Shortly after intubation, it can be helpful distention that compresses the thoracic
avoid causing iatrogenic harm while
to evaluate the patient’s height with a cavity. A general approach is to reduce
the underlying process is being treated.
tape measure to accurately calculate the pressure to less than 30 cm H2O.
It can be particularly challenging to
their ideal body weight. A first step in reducing this pressure is
balance adequate ventilatory support
to decrease the patient’s tidal volume
and lung protection when managing Plateau Pressure
and ensure the absence of dynamic
critically ill patients, as no single Along with targeting low tidal
hyperinflation.
ventilator mode can accomplish volumes, it is also important to avoid
oxygenation and ventilation goals. All overdistending the alveoli and increasing Dynamic Hyperinflation
ventilator settings require clinicians to the transpulmonary pressure gradient.5 Dynamic hyperinflation, also
be mindful of tidal volumes, airway The plateau pressure is a commonly known as auto-PEEP or breath
pressures, and respiratory rates to avoid accepted surrogate when monitoring stacking, is a phenomenon in which
causing harm. for overdistention. When evaluating a the lungs fail to completely empty
18 Critical Decisions in Emergency Medicine
before the next ventilator-delivered While it is commonly taught to is zero. This concept can be easily
breath. This is commonly seen disconnect crashing patients with demonstrated by being mindful of
when patients with obstructive lung obstructive lung disease from the the pause after a normal spontaneous
disease (eg, emphysema, asthma) are ventilator to allow complete exhalation, exhalation. The process is shown on
intubated. Because these patients evidence of hyperinflation can be the ventilator when the flow returns to
do not completely exhale before the detected long before cardiovascular baseline. If the flow does not return to
next delivered breath, lung volumes collapse. This complication can be zero before the next breath, the patient
progressively increase over multiple checked at the bedside by observing the may be exhaling when the breath is
respiratory cycles. As the volume of air flow curve in a relaxed patient (Figure 2) being delivered — a problem that can
in the lungs rises, so does the pressure; and assessing the total positive end- lead to dynamic hyperinflation.
this dynamic increases the risk of expiratory pressure (PEEP) compared A similar thought experiment is
complications, including pneumothorax the set PEEP. to have the patient exhale only half
and cardiovascular collapse from During a normal respiratory cycle, the total lung volume before taking
decreased preload. the flow at the end of exhalation another breath, which can become very
uncomfortable after a small number of
respiratory cycles. The total PEEP (ie,
FIGURE 1. Pressure Waveform of a Mechanical Ventilator on Volume Control
Mode of a Relaxed Patient the total pressure in the thorax) can
be measured during an end-expiratory
Plateau hold in a relaxed patient. The difference
Pressure Total PEEP between the total PEEP and the
PEEP set on a ventilator is “auto-
PEEP,” which reflects the unintended
excess pressure caused by dynamic
hyperinflation. While there is no clear,
Pressure
Auto-PEEP harmful cutoff, monitoring a trend is
helpful when manipulating respiratory
rates and tidal volumes in patients
with obstructive lung disease. This
Inspiratory Expiratory
Hold Hold condition can be treated by increasing
the absolute exhalation time, a process
The inspiratory hold allows the measurement of plateau pressure. Flow stops during that is best accomplished by reducing
this pause; the alveolar pressure can be measured because pressure equilibrates along the respiratory rate.
the ventilator circuit when there is zero flow. Similarly, an expiratory hold inhibits the
Oxygen Toxicity
ventilator from delivering the next breath and allows the pressure to equilibrate. To
calculate “auto-PEEP” subtract the set PEEP from the total PEEP. The difference is the Hyperoxia has been increasingly
auto PEEP. To acutely measure these variables, the patient must be sedated without recognized as a harmful pathological
exerting spontaneous respiratory effort. entity in the critically ill. The goal
of oxygen management is to obtain
a therapeutic level of oxygenation
FIGURE 2. Square-Flow Waveform of a Mechanical Ventilator with the lowest fraction of inspired
oxygen (FiO2) and lowest PEEP. For a
majority of newly intubated patients, an
Inhalation oxygenation goal above 92% suffices,
(+)
and the clinician should attempt to
Zero Flow titrate the PEEP to reduce the FiO2 to
Flow
under 60%.6
Obstructive Lung Disease
(-)
Exhalation Hypercarbic respiratory failure is
the primary physiologic disturbance in
Complete Continued patients with obstructive lung disease
Exhalation Exhalation who require mechanical ventilation.
An elevated partial pressure of carbon
Positive flow represents ventilator-assisted inhalation, and negative flow represents
dioxide (pCO2) can commonly be
passive exhalation. The exhalation arm approaching zero between breaths indicates
complete exhalation. If the exhalation arm of the flow curve does not approach zero
seen in the ABG measurements of
before the next ventilator-delivered breath (noted by the star), incomplete exhalation is newly intubated patients. While the
indicated, and breath stacking will occur. reflexive response to an elevated pCO2
is to increase the minute ventilation
June 2020 n Volume 34 Number 6 19
tolerate permissive hypercarbia
TABLE 1. Tips for Managing Obstructive Lung Disease or hypoxia because of pulmonary
“Low and A low tidal-volume strategy with a low respiratory rate. Typically, vasoconstriction and increased right
slow” strategy 6-8 mL/kg of predicted body weight with a respiratory rate of ventricular afterload.11 Worsening
12-14 breaths/minute. afterload may precipitate further failure.
Tolerate It is important to tolerate hypercarbia because reflexive Key concepts for managing pulmonary
hyercarbia hyperventilation may significantly harm patients.
hypertension are normocarbia,
Check for To assess for adequate exhalation time, check the total PEEP with an
air trapping end-expiratory hold, and evaluate the expiratory limb of the flow curve
normoxia, low tidal volumes, and low
to ensure that it returns to zero before the patient’s next breath. PEEP and plateau pressures.
CRITICAL DECISION
by increasing the respiratory rate or Sepsis and ARDS
tidal volume, this is counterproductive Patients who develop impaired What sedatives and analgesic
and commonly leads to dynamic oxygen exchange with diffuse bilateral agents are preferred for
hyperinflation. infiltrates or altered respiratory intubated patients in the
“Low and slow” is a helpful mechanics without hydrostatic emergency department?
approach when determining a patient’s pulmonary edema are at high risk for
Analgesia and sedation are
initial ventilator settings (Table 1). ARDS.7 In these cases or when there
critical components in the care of any
As previously mentioned, a low is a concern for lung injury, special
intubated patient, but these elements
tidal volume (6-8 mL/kg of ideal attention must be paid to the lung
are often overlooked. It is vital for
body weight) is important for lung protective ventilation strategy.8 Lung
every emergency physician to have a
protection, but the degree of dynamic protection should be prioritized over the
rapidly accessible sedation package at
hyperinflation is ultimately related to normalization of blood gas.4,5,7
their disposal. Appropriate analgesia
respiratory rate and absolute exhalation While ARDS is a heterogenous
and sedation can be as important as the
time. The most effective way to achieve disease, it is important that the
intubation itself — too much, even early
prevalence of high inflation pressures
a longer absolute exhalation time is in the course, is predictive of delayed
and collapsed lung units adjacent to
through a low respiratory rate; 10 to extubation and increased mortality;
open lung units increase the risk of
14 breaths per minute is a safe start. too little can lead to increased energy
further lung damage.5,9 A low tidal
Decreasing the inspiratory time may expenditure, immunomodulation, and
volume ventilation strategy has been
also be beneficial. even post-traumatic stress disorder.12,13
shown to improve mortality.4 Key steps
An elevation in the patient’s pCO2 Pain, agitation, and delirium are
in the initial management of a patient
level is an expected consequence of the closely linked and should be targeted
with ARDS are:
“low and slow” strategy. While many with specific medications. Although
1. Provide a low tidal volume (6mL/kg
clinicians are uncomfortable with intubated patients have frequently been
predicted body weight).
respiratory acidosis, it is a necessary managed with benzodiazepines alone,
2. Increase PEEP to recruit atelectatic
aspect of ventilator management recent Society of Critical Care Medicine
lung segments and keep them
in patients with severe obstructive (SCCM) guidelines recommend a
expanded.
disease. Patients with pure respiratory “pain-first” approach.14 The old
3. Avoid barotrauma by initially
practice of administering a bolus of
acidosis can tolerate acidemia to a attempting to reduce the plateau
benzodiazepines followed by a paralytic
pH of 7.2.6 Hypercarbia generally pressure below 30 cm H2O.
agent is no longer an acceptable method
improves as the adjunctive therapies 4. Avoid oxygen toxicity by decreasing
of managing intubated patients.
(eg, steroids, bronchodilators) improve the FiO2 to under 60%.
Sedatives should be used once the
the underlying disease. 5. Tolerate permissive hypercarbia.
patient’s pain has been addressed,
When prescribing permissive
Pulmonary Hypertension except when the immediate initiation of
hypercapnia, it is important to
The fragile hemodynamic balance deep sedation is indicated, as in cases
remember that most patients tolerate of intracranial hypertension, severe
inherent in pulmonary hypertension
respiratory acidosis and acidemia makes this pathophysiology difficult to respiratory failure, status epilepticus,
without much consequence. However, manage on a ventilator. These patients and the prevention of awareness
clinicians must be mindful of the are exquisitely sensitive to changes during chemical paralysis. The latter
populations that do not tolerate in preload and afterload.10 After is an extremely important point to
permissive hypercapnia, including intubation, the goals are centered around remember, especially when using long-
pregnant patients and those with maintaining a low tidal volume and low acting paralytics like rocuronium.
severe left or right ventricular failure, plateau pressures to limit the effects on There is ample evidence to show
pulmonary hypertension, intracranial vascular preload. that patients who undergo RSI in the
hemorrhage, elevated ICP, and salicylate Unlike patients with ARDS or emergency department frequently
or sodium channel-blocker overdose.6 emphysema, these patients cannot receive inadequate analgesia and
20 Critical Decisions in Emergency Medicine
sedation — sometimes none at all — Benzodiazepines Special Populations
so it is vital to have these medications Although benzodiazepines are In the same way that certain
available.15,16 inexpensive and readily available, recent conditions warrant a nuanced ventilation
Once the paralytics wear off, the evidence points to a number of untoward strategy, there are certain patient
primary goal should be to optimize effects, including a longer duration populations for which a specific sedative
analgesia. Pain is the most common of mechanical ventilation, longer ICU or analgesic are preferred.
memory patients have of their critical and hospital lengths of stay, increased A combination of propofol
illness. Because sedatives can mask delirium, and long-term cognitive and fentanyl is reasonable for
pain, clinicians should ensure adequate dysfunction.14 Furthermore, parenteral analgosedation in neuro-critically
analgesia before initiating a sedation infusions of lorazepam include propylene ill patients. Continuous infusions of
regimen.12 Common sources of pain glycol, which can lead to metabolic sedatives and opioids are generally
include the ETT itself, manipulation of acidosis and acute kidney injury.39 To considered protective for the injured
post-traumatic injuries, wound care, this end, the 2013 SCCM guidelines brain in the acute phase.19 Both
invasive procedures, nursing care, in- recommend sedation strategies using non- agents are rapidly effective and have
line ETT suctioning, and prolonged benzodiazepine agents to improve clinical a short duration of action when
immobility. outcomes.14 stopped, allowing easier monitoring of
Opioids are most frequently used neurologic function when needed.
Dexmedetomidine
for managing pain in the critically ill. Most patients with an injured
It is important to remember that
While the optimal drug and dose for or ill brain manifest hypertension,
analgesics are poor sedatives — and
each individual patient depends on many and propofol decreases intracranial
vice versa — so the ideal “agent” is
factors, fentanyl and remifentanil are pressure and the cerebral metabolic
either a drug with both properties or,
generally regarded as first-line treatments rate of oxygen while preserving
more likely, a combination of two
because of their quick onset, benign cerebral autoregulation. It should be
medications (eg, propofol and fentanyl).
hemodynamic profile, and unlikely noted, however, that propofol can
Dexmedetomidine is a newer, centrally
accumulation in those with renal cause hypotension. Because even one
acting, highly selective, alpha-2 adrenergic
dysfunction. episode of hypotension can increase
agonist that possesses sedative, anxiolytic,
If not initiated while the patient mortality in those with brain injuries, the
and analgesic properties. It is currently
is paralyzed, sedatives should be medication should be started at a low
approved in the US and Canada for the
administered once pain has been dose and carefully titrated while closely
short-term sedation (<24 hours) of patients
addressed. The most common sedative monitoring for complications.
receiving mechanical ventilation.17
agents, which act via the GABAA Propofol decreases cerebral electrical
The drug is not associated with
receptor, include propofol, etomidate, activity and can also be used to achieve
respiratory depression, which is helpful
benzodiazepines, and barbiturates. A burst suppression in patients with
when liberating patients from mechanical
newer agent, dexmedetomidine, works seizures. Ketamine and dexmedetomidine
ventilation; however, it is associated
as an agonist of the alpha-2 adrenergic can also be considered; however, given
with bradycardia and hypotension.
receptor. Finally, ketamine is a NMDA the lack of good evidence to support
Dexmedetomidine is of particular interest
receptor antagonist that inhibits the their use in this population, this decision
in the critical care community because
influx of calcium into the cells. should be made in consultation with a
studies suggest it may reduce the duration
neurologist or neurosurgeon.
Propofol of mechanical ventilation and incidence of
Propofol is also considered the
The most commonly used sedative is delirium.18
first-line treatment for patients who are
propofol, which has powerful anxiolytic Ketamine withdrawing from alcohol and require
and amnestic properties but no Ketamine, another agent with both intubation. Because most of these
analgesic effect. Propofol is a complex neuroleptic and analgesic properties, patients have already received a large
drug with three half-lives, ranging is a rapidly acting drug that produces quantity of benzodiazepines, the GABA
from minutes to days, but its duration dissociative anesthesia. Patients breathe receptor-agonist properties of propofol
of action is much shorter because it spontaneously, and because the drug can help treat their severe withdrawal.
rapidly crosses the blood-brain barrier activates the sympathetic nervous system, These patients also require analgesia
and distributes to the peripheral tissue. mean arterial pressure (MAP) and heart while intubated.
Adverse reactions to the drug include rate often increase. The widespread use Some smaller studies have examined
pain at the injection site, an increased of ketamine is limited by adverse drug dexmedetomidine for the treatment of
risk of bacterial infections, and reactions, including hallucinations, alcohol withdrawal syndrome. While
cardiovascular effects (eg, hypotension). delirium, tachycardia, and increased the drug can prevent intubation in
Propofol can also cause hyperlipidemia myocardial oxygen demand; however, some patients and blunt the tachycardia
and propofol infusion syndrome, but short-term use in the emergency and hypertension seen with severe
these complications are most often department is generally safe and well withdrawal, it is not recommended as
encountered in the ICU setting. tolerated.17 a single agent and does not obviate the
June 2020 n Volume 34 Number 6 21
need for benzodiazepines.20 As such, possibly because it does not trigger fluctuations associated with ventilator-
propofol is more commonly used to histamine release.21 Ketamine is also an delivered respirations. This modality can
manage withdrawal in patients who have excellent choice because of its minimal help evaluate the fluid responsiveness of
already been intubated. impact on the cardiovascular system and apneic patients on controlled mechanical
Initial treatment with fentanyl and rapid onset of action. Lastly, propofol ventilation.
a benzodiazepine is a valid option for has been associated with hypotension, LTTE is less reliable in patients
hypotensive medical patients. Fentanyl particularly in hypovolemic patients; who are breathing spontaneously
does not precipitate histamine release, however, a half-dose may mitigate this because the degree of IVC fluctuation
and neither agent has significant potential outcome. is a function of both respiratory effort
hemodynamic effects. Ketamine may also After ensuring that there is a secure and the pressure applied to assist
have a role in this patient population airway and adequate ventilation, it ventilation. Without standardized
owing to its positive hemodynamic and is paramount to assess the patient’s ventilator settings, this approach
dissociative effects. Once the patient circulation. Physiologically speaking, has not been proven to be a reliable
can be started on vasopressors, it is airway, breathing, and circulation are indicator of fluid responsiveness.25 In
acceptable to consider transitioning to a intertwined, so altering one parameter the recently paralyzed and intubated
propofol drip if needed for sedation. may impact the others. For example, patient, these measures are ideal for
the negative pressure generated by a assessing hemodynamic instability in
CRITICAL DECISION spontaneously breathing tachypneic the postintubation period. An IVC
What is the best approach patient can bolster cardiac output by diameter less than 1.5 cm is suggestive
for assessing and managing augmenting preload. Transitioning of low intravascular volumes.26 More
hemodynamic instability? from negative-pressure ventilation importantly, this measurement can be
may decrease venous return to the reassessed after blood or crystalloid are
Peri-intubation instability can be heart, causing hypotension or arrest. provided, allowing the clinician to trend
mitigated prior to intubation with some Intubation independently increases the the patient’s response.
preparation and forethought, time risk of death.22
permitting. Hypotension is an ominous Mitigating Complications
In most cases, the first sign of trouble
finding and should heighten awareness Some patients with heightened
is the blood pressure measurement
that complications may occur. Although vagal tone can develop bradycardia as
taken immediately after the ETT
an elevated diastolic blood pressure the laryngoscope or GlideScope presses
tube is secured. Overall, noninvasive
reflects increased vascular tone that may the back of the pharynx or as the ETT
blood pressure cuffs are accurate in
be maintaining perfusion pressures, this is advanced. Preintubation atropine
determining normal MAP, but individual
may resolve once a patient is induced should be considered when intubating
diastolic and systolic blood pressures can
and intubated. pediatric patients, who are infamous for
vary widely when compared to arterial
Hypovolemia can be addressed manifesting this phenomenon; however,
line measurements.23 Additionally,
prophylactically in high-risk patients, some research suggests that the drug may
different monitors may provide differing
including those with sepsis and large, not prevent reflex bradycardia entirely.27
values depending on the manufacturer’s
insensible volume losses caused by fever, The administration of atropine can help
proprietary algorithm.
vomiting, or diarrhea. This is especially clinicians quickly determine if vagal
Overall, noninvasive blood
true with trauma patients, for whom stimulation is the cause of the patient’s
pressure measurements are unreliable
blood transfusions should be considered bradycardia and hypotension.
in critically ill patients; an arterial
if tachycardia, a labile blood pressure Hypotension, far and away the
line should be considered early before
(ie, any low reading), tachypnea, or most frequent complication in the
patients lose their radial pulses from
altered mental status are present before postintubation period, is associated
worsening decompensation. Leg and
the decision to intubate is made. An with increased hospital mortality.22 Both
thigh blood pressures correlate with
infusion of crystalloid solution (250 mL- pre- and postintubation hypotension
upper-arm cuff MAPs, but these values
500 mL) is not detrimental, even for are also associated with peri-intubation
may be unreliable when evaluating a
fluid-overloaded patients. cardiac arrest. Other factors that have
hypotensive or tachycardic patient.24
The choice of induction medications been associated with postintubation
also impacts postintubation Transthoracic Echocardiography hypotension are advanced age, the use
hemodynamics. If a patient is in cardiac Bedside ultrasound, specifically a of neuromuscular blockers, preexisting
arrest or is about to arrest, no sedation limited transthoracic echocardiogram COPD, sepsis, and extremes in body
or paralytic is needed. In such cases, (LTTE), can be helpful for assessing weight.28
the administration of these agents perfusion and intravascular volume. Complications that arise during
wastes time and exposes the patient to a Ultrasound imaging is a safe, intubation (eg, hypoxemia, esophageal
multitude of risks. Classically, etomidate noninvasive method for measuring intubation, vomiting/aspiration, arrest,
is the agent of choice because it causes the diameter of the inferior vena cava and suspected sepsis) also predispose
less hypotension than other agents, (IVC) and the degree of collapse and patients to postprocedure hypotension.29
22 Critical Decisions in Emergency Medicine
Importantly, a preintubation blood hypoxia) may still be in play and can be anesthesiologists and has been used in
pressure under 140 mm Hg is a accompanied by hypertension. However, the emergency department with good
significant indicator of postintubation if hypotension or tachycardia persist, effect.33 In a proper concentration (40
hypotension and its associated other etiologies should be pursued, μg/mL), phenylephrine can also be
complications; as such, hypotension including an occult ischemia/infarct, given through a peripheral IV for a
before induction is an ominous sign and poorly controlled infectious source, short period of time, enabling further
should be addressed if time permits. ongoing hemorrhage, or septic shock. treatment of any instabilities.34
The usual first-line response Some research suggests that older
to a decompensating patient in
Norepinephrine
and/or sicker patients may already
nonhemorrhagic shock is a 20-mL/kg For most cases of shock,
have a heightened adrenergic tone
fluid bolus given rapidly, but only half to norepinephrine is a good initial agent to
that prevents the expected response
two-thirds of patients with septic shock use once the decision to use vasopressors
to norepinephrine. In such cases,
respond to this intervention.25 Although has been made. However, in the peri-
agents that do not use an adrenergic-
the utility of early goal-directed therapy intubation period, the drug has been
stimulation pathway may be more
has recently been dispelled in emergency associated with in-hospital and 90-
beneficial. Although vasopressin has
department patients, hypotension must day mortality, even after controlling
been advocated, it does not appear to be
be corrected promptly.30 for the patients’ original illness.31,32
superior to norepinephrine.35
Whenever possible, patients Its mechanism of increased systemic
with trauma or GI bleeding should vascular resistance (alpha-1 agonist), CRITICAL DECISION
receive blood products before coupled with its significant effect upon
How should metabolic
crystalloid solutions are administered. arterial and venous capacitance vessels,
Postintubation instability can generally enhances venous return to the heart. derangements be managed?
be corrected by allowing time for the A patient’s lack of response to Metabolic acidosis arises when
induction agents to wear off while norepinephrine should cause alarm. fixed acids in the blood increase. This
adding intravascular volume. Patients For instance, does the patient have a can occur when a patient gains a strong
may develop tachycardia as they become spinal injury that might require a pure acid (eg, in cases of ketoacidosis or
more alert after intubation; furthermore, alpha agonist, such as phenylephrine? lactic acidosis) or loses their base (eg,
their underlying pathology (eg, trauma, This agent is a favorite pressor of in cases of diarrhea or renal failure). To
TABLE 2. Common Metabolic Derangements
Initial Blood Blood Gas
Primary Compensatory Gas Results Blood Gas Results After Results After Full
Disburbance Common Causes Mechanism (uncompensated) Partial Compensation Compensation
Respiratory Hypoventilation Increase bicarbonate pH decreased pH decreased but pH normal
acidosis due to: (kidney and red PaCO2 increased closer to normal PaCO2 increased
(ie, primary • Pneumonia blood cells) PaCO2 increased
Bicarbonate normal Bicarbonate increased
increase in PaCO2) • Asthma Compensation slow Bicarbonate increased
• COPD (several days, maybe
• Depression of weeks)
respiratory center
Respiratory Hypoventilation Decrease pH increased pH decreased but pH normal
acidosis due to: bicarbonate (kidney PaCO2 decreased closer to normal PaCO2 decreased
(ie, primary • Pain and red blood cells)
Bicarbonate normal PaCO2 decreased Bicarbonate decreased
decrease in PaCO2) • Anxiety attack Compensation slow Bicarbonate decreased
• Stimulation of (several days, maybe
respiratory center weeks)
Metabolic acidosis • Renal failure Decrease PaCO2 pH decreased pH decreased but pH normal
(ie, primary • Diabetic (ie, increase PaCO2 normal closer to normal PaCO2 decreased
decrease in ketoacidosis respiratory ventilation) PaCO2 increased
Bicarbonate Bicarbonate decreased
bicarbonate) • Circulatory
Compensation rapid decreased Bicarbonate decreased
failure/shock
(minutes/hours)
Metabolic acidosis • Excessive Increase PaCO2 pH increased pH increased but closer Full compensation
(ie, primary bicarbonate (ie, increase PaCO2 normal to normal is rare in metabolic
increase in ingestion respiratory ventilation) PaCO2 decreased alkalosis beause the
Bicarbonate
bicarbonate) • Potassium decreased ventilation
Compensation rapid increased Bicarbonate increased
depletion required would threaten
(minutes/hours)
• Vomiting of blood oxygenation.
gastric acid Full compensation
is prevented by
“hypoxaemic drive.”
June 2020 n Volume 34 Number 6 23
compensate for these abnormalities, the true respiratory failure, a sodium usual suspects (eg, underlying cardiac
body hyperventilates to decrease arterial bicarbonate infusion should be initiated ischemia/infarct, overwhelming sepsis)
PCO2. prior to intubation. It is important must be carefully considered.
If a patient with metabolic acidosis to avoid long-acting sedatives and
Tension Pneumothorax
requires RSI, hyperventilation is paralytic agents and consider pressure-
Tension pneumothorax is the
necessary to prevent acidosis from controlled ventilation to allow increased
most worrisome complication of
worsening. The retained CO2 from tidal-volume breaths.
intubation. Regardless of how well
apnea or a “normal” respiratory rate
CRITICAL DECISION chest compressions are done and how
can worsen pH and lead to depressed
closely the ACLS protocol is followed,
myocardial activity, increased What causes of postintubation there will be no resolution of arrest until
arrhythmias, elevated intracranial cardiac arrest should the tension pneumothorax is treated.
pressure, and possibly death.
emergency physicians be Although this phenomenon can occur for
As such, a modified RSI approach
should be used when intubating
prepared to address? many reasons, trauma and underlying
illness are the most frequent causes.
any patient with metabolic acidosis. Although cardiac arrest occurs in
Bilateral chest tubes should be placed
This approach has been termed 2% to 4% of intubated patients, it
first in patients who present in cardiac
“resuscitation-sequence intubation” occurs twice as frequently in emergent
arrest with associated recent or distant
with a focus on resuscitation measures intubations than in elective ones.22,37,38
trauma.
(eg, fluid resuscitation, vasopressors, Peri-intubation cardiac arrest is
Bedside ultrasound should also
optimizing oxygenation) before usually a bradycardic or pulseless
be used to evaluate for the absence
intubation, if possible.36 It is also electrical activity event. Risk factors
of lung sliding and the presence of
prudent to consider alternatives to associated with these complications
the lung point sign, findings that are
typical RSI medications, such as include increased patient age, a high
specific for pneumothorax. However,
ketamine or dexmedetomidine, which BMI, and procedural complications
it is important to recognize that other
can facilitate intubation without (eg, multiple intubation attempts,
pulmonary etiologies can cause these
altering the patient’s minute ventilation. hypoxia, hypotension); furthermore,
findings as well.39,40 Patients with
Another population at risk of preprocedural hypotension is frequently
known COPD or bullous lung disease
intubation-associated decline are those present.
and those who appear Marfanoid may
with salicylate overdose. This toxidrome, Hypotension may represent a
also be candidates for early chest tube
which classically causes metabolic hypovolemic state, underlying cardiac
placement in the postintubation period.
acidosis and respiratory alkalosis, can ischemia, or advanced septic shock,
Of note, chest x-rays should not delay
be diagnosed clinically by the presence any of which can overwhelm the
placement of a chest tube when a tension
of tachypnea (Table 2). Decreasing patient’s compensation mechanisms. As
physiology is being considered.
respiratory alkalosis in these patients intubation and mechanical ventilation
increases the passage of salicylate into change the chest physiology from Pericardial Tamponade
the central nervous system. negative to positive pressure, these While pericardial tamponade is
Because intubation and mechanical underlying problems can lead to cardiac not caused by intubation, the change
ventilation can rapidly worsen arrest or profound hypotension. from negative-pressure to positive-
outcomes, intubation should be avoided Below is a short list of postintubation pressure ventilation can often diminish
whenever possible. If the procedure cardiac arrest etiologies that must either preload past a point at which cardiac
is necessary for the management of be treated or ruled out. In addition, the arrest ensues. Pericardial tamponade is
addressed in ACLS and ATLS protocols,
and an evaluation of the pathology is
best addressed by bedside ultrasound. In
such cases, physical examination findings
and chest radiographs are nonspecific.
Overwhelming Acidosis
n Provide analgesia to every intubated patient, and then quickly move to Metabolic, respiratory, and
sedation if agitation persists. mixed acidosis are other causes of
n Be prepared for cardiac arrest or further hypotension and instability when postintubation cardiac arrest that are
managing patients who are hypotensive before induction for intubation. A
not directly caused by intubation;
bolus of crystalloid solution or pressors should be considered.
however, the brief period in which a
n Measure the patient’s height to accurately prescribe a lung-protective
patient cannot offload carbon dioxide
ventilation strategy of 6 to 8 mL/kg of predicted body weight.
can be enough to overwhelm their
n Perform an inspiratory hold to evaluate the patient’s plateau pressure and
an expiratory hold to check for auto-PEEP. metabolic balance. Typically, these
patients present with metabolic acidosis
24 Critical Decisions in Emergency Medicine
(eg, aspirin overdose, ethylene glycol, CRITICAL DECISION in a semirecumbent position unless
diabetic ketoacidosis) for which they contraindications (eg, unstable spine
What can be done to
appropriately develop an increased fractures) exist.
decrease the risk of ventilator- Subglottic secretion removal is
respiratory drive to offload carbon
dioxide.
associated pneumonia? also recommended to reduce the risk
Patients with acidosis often present Ventilator-associated pneumonia of VAP. Commercially available ETTs
on the verge of respiratory failure (VAP), a known complication of with subglottic suction ports allow
because their work of breathing is mechanical ventilation, is defined as continuous or intermittent suction.
unsustainable; furthermore, when pneumonia that did not appear to be While these tubes are more expensive
they are sedated and paralyzed, they incubating at the time of admission but than traditional ETTs, a 2005 meta-
completely lose this compensation develops more than 48 to 72 hours after analysis of nearly 900 patients showed
endotracheal intubation. The disease that subglottic suction reduced the
mechanism. Shortly after induction
is thought to result from a leakage of risk of VAP by 49%.43 However, these
and intubation (a period during which
oropharyngeal secretions around the devices do not appear to reduce the
the patient is not breathing and CO2
ETT cuff and into the lungs.41 Ventilator- length of mechanical ventilation, ICU
accumulates) these patients either seize
associated pneumonias are particularly stays, or mortality.
or arrest.
important because they increase the Endotracheal cuff pressure
Acidosis will continue if this risk
length of mechanical ventilation and management is also extremely
is not considered because, per ACLS
the length of stay, elevate the risk of important. Although the movement of
protocols, patients in cardiac arrest morbidity and mortality, and increase secretions from the oropharynx into
are only intermittently ventilated. health care costs. the lungs increases the risk of VAP,
Capnography is instrumental for While these cases are often an effective cuff seal may reduce the
monitoring such cases. Although an diagnosed in the ICU, a number passage of secretions. The recommended
ABG measurement can ultimately of simple emergency department range for cuff pressure is 20 to 30 cm
confirm metabolic derangements, these interventions can reduce this risk. H2O. Pressures under 20 cm H2O
test results take a relatively long time in First, there is moderate evidence to are associated with a greater risk of
most institutions. recommend ventilating patients without pneumonia.
benzodiazepine sedation. If analgesics Finally, there is moderate
Esophageal Intubation
alone can make the patient comfortable, evidence to support oral care with
Cardiac arrest in the postintubation
sedation should be avoided.42 chlorhexidine solution for all intubated
period should be attributed to a Several studies also suggest that patients. Success with this approach
misplaced ETT until proven otherwise. patients should be positioned with is primarily reported in the cardiac
In many cases, these events are preceded the head of bed elevated 30 to 45 surgery population; data to endorse
by hypoxia. Again, CO2 capnography degrees. While evidence to support this its use in a general population is more
or capnometry will also be abnormal approach is poor and often conflicting, equivocal. However, the cost and
and should be addressed long before a it remains a basic practice because of safety of chlorhexidine have made
chest x-ray is obtained. In such cases, its simplicity, lack of cost, and potential it a ubiquitous treatment. Research
a second look with traditional or video benefits. Supine positioning predisposes from the Netherlands points to
laryngoscopy should be part of the patients to the microaspiration of decreased mortality when selectively
patient’s workup. gastric contents, so most should remain decontaminating the oropharynx with
antibiotics, although this practice
has not been adopted in the US over
concerns regarding antibiotic-resistant
infections.
Summary
n Failing to provide immediate analgesia and sedation following intubation, Emergency departments are receiving
especially when using long-acting paralytic agents. an increasing number of critically ill
n Allowing a suspected acidotic patient to undergo a prolonged period of intubated patients, many of whom
not being ventilated while undergoing intubation. This mistake can lead to require substantial bedside care prior to
seizures or cardiac arrest. ICU admission. Emergency physicians
n Hyperventilating a patient with asthma or emphysema because of hypercarbia. cannot expect their job to end once a
This leads to breath stacking and eventual hemodynamic collapse if not patient’s airway is secure. It is important
recognized early.
to understand the detrimental effects
n Setting the ventilator immediately after intubation and not returning to assess
that accompany improper mechanical
the need for changes. It is important to remember that, once intubated,
critically ill patients have a dynamic physiology and changing ventilatory needs. ventilation and be prepared to prescribe
appropriate ventilator settings.
June 2020 n Volume 34 Number 6 25
CASE RESOLUTIONS
■ CASE ONE He was extubated to a nasal cannula obtained, the patient was started
with intermittent bronchodilators. The on high-flow oxygen, and volume
A postintubation chest x-ray
patient was quickly transferred out resuscitation was initiated. Given his
of the young man in respiratory
of the ICU and discharged home on profound hypotension, peripheral
distress showed clear lung fields.
hospital day two. norepinephrine was administered
An end-expiratory hold maneuver
while volume resuscitation was
was performed while the patient ■ CASE TWO continued.
was still paralyzed, which revealed Even without an ABG measurement, When the patient’s MAP rose above
a total PEEP of 40 cm H 2O with the astute emergency physician 60 mm Hg, the emergency physician
a set PEEP of 5 cm H 2O. His recognized that the woman with a focused on intubating him using
ETT was promptly removed from presumed overdose was profoundly etomidate and rocuronium, while using
the ventilator for approximately acidotic. She was immediately bag-valve-mask ventilation during
20 seconds, enabling complete hyperventilated to blow off any periods of apnea to prevent respiratory
exhalation. After the patient was accumulated CO2 , and a bolus of acidosis. Lung-protective ventilator
reattached to the ventilator, the rate crystalloid solution was administered. settings were used with a respiratory
was decreased to 12 breaths/minute. The patient quickly stopped seizing, and rate that was equivalent to the man’s
IV methylprednisolone and inhaled her MAP improved slightly. preintubation respiratory rate.
bronchodilators were initiated. Early laboratory tests revealed a A bolus dose of fentanyl was
Because significant patient- pH of 7.0 and high anion-gap acidosis. administered followed by a dose of
ventilator dyssynchrony and severe The patient continued to breathe over propofol to provide sedation while the
airflow obstruction persisted, a ventilator rate of 18 breaths/minute, patient remained chemically paralyzed.
analgesia and sedation were so pressure support was added while Aware that this approach might cause
increased, and the patient was taking measures to avoid auto-PEEP. hypotension, the clinician continued
chemically paralyzed again. The Further laboratory tests revealed renal volume resuscitation and provided
emergency physician was willing to failure and an elevated ethylene glycol a titrated dose of norepinephrine
tolerate the patient’s hypercarbia to level, consistent with poisoning, and the while working on a central line. A
prioritize adequate ventilation, while patient was transferred to a tertiary care fentanyl infusion was also started.
closely monitoring for end-expiratory facility for further management. After adequate time had passed for
flow and auto-PEEP. the rocuronium to metabolize, the
The patient was transferred ■ CASE THREE patient was weaned off the propofol
to the ICU, where his airflow The elderly man with emphysema but continued on the fentanyl drip. He
obstruction and bronchospasm was determined to be septic and likely was then taken to the ICU for further
significantly improved overnight. acidotic. Two large-bore IVs were management.
Intubated patients also require patients without acute respiratory distress syndrome: a 13. Shehabi Y, Bellomo R, Reade MC, et al. Early intensive
meta-analysis. JAMA. 2012 Oct;308(16):1651-1659. care sedation predicts long-term mortality in ventilated
the thoughtful administration of 4. Acute Respiratory Distress Syndrome Network, Brown critically ill patients. Am J Respir Crit Care Med. 2012
RG, Matthay MA, et al. Ventilation with lower tidal Oct;186(8):724-731.
analgesia and sedation, and it is vital volumes as compared with traditional tidal volumes 14. Barr J, Fraser GL, Puntillo K, et al. Clinical practice
for acute lung injury and the acute respiratory distress guidelines for the management of pain, agitation, and
to understand the different agents syndrome. N Engl J Med. 2000 May;342(18):1301-1308. delirium in adult patients in the intensive care unit.
that can fulfill this role. Finally, these 5. Tobin MJ. Principles and Practice of Mechanical Crit Care Med. 2013 Jan;41(1):263-306.
Ventilation. 3rd ed. Dallas, TX: McGraw-Hill Medical; 15. Bonomo JB, Butler AS, Lindsell CJ, Venkat A.
patients can manifest significant acid- 2013. Inadequate provision of postintubation anxiolysis
6. Mosier JM, Hypes C, Joshi R, Whitmore S, and analgesia in the ED. Am J Emerg Med. 2008
base and hemodynamic disturbances, Parthasarathy S, Cairns CB. Ventilator strategies and May;26(4):469-472.
including peri-intubation cardiac arrest. rescue therapies for management of acute respiratory
failure in the emergency department. Ann Emerg Med.
16. Kendrick DB, Monroe KW, Bernard DW, Tofil NM.
Sedation after intubation using etomidate and a long-
Recognizing the most likely causes of 2015 Nov; 66(5):529-541. acting neuromuscular blocker. Pediatr Emerg Care.
7. Malhotra A. Low-tidal-volume ventilation in the acute 2009 Jun;25(6):393-396.
these complications may help prevent respiratory distress syndrome. N Engl J Med. 2007 17. Roberts DJ, Haroon B, Hall RI. Sedation for critically
Sep;257(11):1113-1120. ill or injured adults in the intensive care unit: a shifting
them altogether. 8. ARDS Definition Task Force, Ranieri VM, Rubenfeld GD, paradigm. Drugs. 2012 Oct;72(14):1881-1916.
et al. Acute respiratory distress syndrome: the Berlin 18. Reade MC, Eastwood GM, Bellomo R, et al. Effect
REFERENCES 9.
definition. JAMA. 2012 Jun;307(23):2526-2533.
Amato MBD, Meade MO., SlutskyAS, et al. Driving
of dexmedetomidine added to standard care on
ventilator-free time in patients with agitated delirium:
1. Gajic O, Dara SI, Mendez JL, et al. Ventilator-associated pressure and survival in the acute respiratory distress a randomized clinical trial. JAMA. 2016 Apr;315(14):
lung injury in patients without acute lung injury at the syndrome. N Engl J Med. 2015Feb;372(8):747-755. 1460-1468.
onset of mechanical ventilation. Crit Care Med. 2004 10. Wilcox SR, Kabrhel C, Channick RN. Pulmonary 19. Oddo M, Crippa IA, Mehta S, et al. Optimizing
Sep;32(9):1817-1824. hypertension and right ventricular failure in emergency sedation in patients with acute brain injury. Crit Care.
2. Fuller BM, Mohr NM, Drewry AM, Carpenter CR. medicine. Ann Emerg Med. 2015 Dec;66(6):619-628. 2016 May;20(1):128.
Lower tidal volume at initiation of mechanical 11. Zamanian RT, Haddad F, Doyle RL, Weinacker AB. 20. Rayner SG, Weinert CR, Peng H, Jepsen S, Broccard
ventilation may reduce progression to acute respiratory Management strategies for patients with pulmonary AF, Study Institution. Dexmedetomidine as adjunct
distress syndrome: a systematic review. Crit Care. hypertension in the intensive care unit. Crit Care Med. treatment for severe alcohol withdrawal in the ICU.
2013;17(1):R11. 2007 Sep;35(9):2037-2050. Ann Intensive Care. 2012 May;2(1):12.
3. Serpa Neto A, Cardoso SO, Manetta JA, et al. 12. Reade MC, Finfer S. Sedation and delirium in the 21. Benson M, Junger A, Fuchs C, Quinzio L, Böttger S,
Association between use of lung-protective ventilation intensive care unit. N Engl J Med. 2014 Jan;370(5): Hempelmann G. Use of an anesthesia information
with lower tidal volumes and clinical outcomes among 444-454. management system (AIMS) to evaluate the physiologic
26 Critical Decisions in Emergency Medicine
effects of hypnotic agents used to induce anesthesia. Leatherman J. Mechanical Ventilation for Severe Asthma.
J Clin Monit Comput. 2000;16(3):183-190. Chest. 2015 Jun;147(6):1671-1680.
22. Heffner AC, Swords DS, Neale MN, Jones AE. Levitan, Richard. Timing Resuscitation Sequence Intubation
Incidence and factors associated with cardiac arrest for Critically Ill Patients. ACEPNow, ACEP/Wiley. August
complicating emergency airway management. 2015.
Resuscitation. 2013 Nov;84(11):1500-1504. Mosier JM, Hypes C, Joshi R, Whitmore S, Parthasarathy S,
23. Ribezzo S, Spina E, Di Bartolomeo S, Sanson Cairns CB. Ventilator strategies and rescue therapies
G. Noninvasive techniques for blood pressure for the management of acute respiratory failure in the
measurement are not a reliable alternative to direct emergency department. Ann Emerg Med. 2015 Nov;
measurement: a randomized crossover trial in ICU. 66(5):529-541
ScientificWorldJournal. 2014 Jan;2014:353628. Reade MC, Finfer S. Sedation and delirium in the intensive
24. Lakhal K, Ehrmann S, Benzekri-Lefèvre D, et al. care unit. N Engl J Med. 2014 Jan;370(5):444-454.
Brachial cuff measurements of blood pressure
during passive leg raising for fluid responsiveness
prediction. Ann Fr Anesth Reanim. 2012;31(5):e67-e72.
25. Boyd JH, Sirounis D, Maizel J, Slama M.
Echocardiography as a guide for fluid management.
Crit Care. 2016 Sep;20:274.
26. Lee CW, Kory PD, Arntfield RT. Development of a fluid
resuscitation protocol using inferior vena cava and lung
ultrasound. J Crit Care. 2016 Feb;31(1):96-100.
27. Fastle RK, Roback MG. Pediatric rapid sequence
intubation: incidence of reflex bradycardia and effects
of pretreatment with atropine. Pediatr Emerg Care.
2004 Oct;20(10):651-655.
28. Lin CC, Chen KF, Shih CP, Seak CJ, Hsu KH. The
prognostic factors of hypotension after rapid sequence
intubation. Am J Emerg Med. 2008 Oct;26(8):845-851.
29. Smischney NJ, Demirci O, Diedrich DA, et al. Incidence
of and risk factors for post-intubation hypotension in
the critically ill. Med Sci Monit. 2016;22:346-355.
30. Angus DC, Barnato AE, Bell D, et al. A systematic
review and meta-analysis of early goal-directed therapy
for septic shock: the ARISE, ProCESS and ProMISe
Investigators. Intensive Care Med. 2015 Sep;41(9):
1549-1560.
31. De Backer D, Biston P, Devriendt J, et al. Comparison
of dopamine and norepinephrine in the treatment of
shock. N Engl J Med. 2010 Mar;362(9):779-789.
32. Smischney NJ, Demirci O, Ricter BD, et al. Vasopressor
use as a surrogate for post-intubation hemodynamic
instability is associated with in-hospital and 90-day
mortality: a retrospective cohort study. BMC Res Notes.
2015;8:445.
33. Panchal AR, Satyanarayan A, Bahadir JD, Hays D,
Mosier J. Efficacy of bolus-dose phenylephrine for
peri-intubation hypotension. J Emerg Med. 2015
Oct;49(4):488-494.
34. Delgado T, Wolfe B, Davis G, Ansari S. Safety of
peripheral administration of phenylephrine in a
neurologic intensive care unit: a pilot study. J Crit Care.
2016 Aug;34:107-110.
35. Russell JA, Walley KR, Singer J, et al. Vasopressin versus
norepinephrine infusion in patients with septic shock.
N Engl J Med. 2008 Feb;358(9):877-887.
36. Levitan RM. Timing resuscitation sequence intubation
for critically ill patients. ACEPNow. https://www.
acepnow.com/article/timing-resuscitation-sequence-
intubation-for-critically-ill-patients. Published August
13, 2015.
37. Kim WY, Kwak MK, Ko BS, et al. Factors associated
with the occurrence of cardiac arrest after emergency
tracheal intubation in the emergency department.
PLoS One. 2014 Nov;9(11):e112779.
38. Leibowitz AB. Tracheal intubation in the intensive care
unit: extremely hazardous even in the best of hands.
Crit Care Med. 2006 Sep;34(9):2497-2498.
39. Aziz SG, Patel BB, Ie SR, Rubio ER. The lung point sign,
not pathognomonic of a pneumothorax. Ultrasound Q.
2016 Sep;32(3):277-279.
40. Sim SS, Lien WC, Chou HC, et al. Ultrasonographic
lung sliding sign in confirming proper endotracheal
intubation during emergency intubation. Resuscitation.
2012 Mar;83(3):307-312.
41. Grap MJ, Munro CL, Unoki T, Hamilton VA, Ward KR.
Ventilator-associated pneumonia: the potential critical
role of emergency medicine in prevention. J Emerg
Med. 2012 Mar;42(3):353-362.
42. Klompas M, Branson R, Eichenwald EC, et al. Strategies
to prevent ventilator-associated pneumonia in acute
care hospitals: 2014 update. Infect Control Hosp
Epidemiol. 2014 Aug;35(8):915-936.
43. Dezfulian C, Shojania K, Collard HR, Kim HM, Matthay
MA, Saint S. Subglottic secretion drainage for
preventing ventilator-associated pneumonia: a meta-
analysis. Am J Med. 2005 Jan;118(1):11-18.
ADDITIONAL READING
Angus DC, Barnato AE, Bell D, et al. A systematic review
and meta-analysis of early goal-directed therapy
for septic shock: the ARISE, ProCESS and ProMISe
Investigators. Intensive Care Med. 2015 Sep;41(9):
1549-1560.
Bonomo JB, Butler AS, Lindsell CJ, Venkat A. Inadequate
provision of postintubation anxiolysis and analgesia in
the ED. Am J Emerg Med. 2008 May;26(4):469-472.
June 2020 n Volume 34 Number 6 27
Mechanical
Engineering
Ventilator Management
LESSON 17
By Andrew T. Schaub, DO; Christopher Peluso, DO; and
Matthew J. Stull, MD
Dr. Schaub is an attending emergency physician and clinical instructor at
MetroHealth/Case Western Reserve University in Cleveland, Ohio. Dr. Peluso is
a wilderness medicine fellow and an attending physician in the Department of
Emergency Medicine at Wake Forest University School of Medicine in Winston-
Salem, North Carolina. Dr. Stull is the assistant emergency medicine residency
director and an assistant professor in the Departments of Emergency Medicine and
Anesthesiology at University Hospitals-Cleveland Medical Center and Case Western
Reserve University in Cleveland, Ohio.
Reviewed by George Sternbach, MD, FACEP
OBJECTIVES
On completion of this lesson, you should be able to: CRITICAL DECISIONS
1. Devise a strategy for ventilator settings based on the n What initial ventilator strategies are most
initial indication for intubation.
appropriate after emergent intubation?
2. Describe the complications of inappropriate ventilator
settings in the emergency department. n How should intubated patients be monitored in
3. Apply appropriate ventilator settings in response to the emergency department?
dynamic patient conditions.
n What strategies are available for patients who fail
4. Understand how initial emergency department ventilator
to adequately ventilate?
settings impact patient outcomes.
5. Recognize adjuncts to ventilator management to enhance n What strategies are available for patients who fail
ventilator care for critically ill patients. to adequately oxygenate?
FROM THE EM MODEL
19.0 Procedures and Skills Integral to the Practice
of Emergency Medicine
19.1 Airway Techniques
19.1.6 Ventilatory Monitoring
Emergency physicians have the opportunity to intervene early to prevent downstream mortality and morbidity in
patients who must be mechanically ventilated, approximately 20.6% of whom die before leaving the hospital.1,2 As
the prevalence of critical care admissions and prolonged boarding continues to rise across the United States, it becomes
increasingly important to design effective, dynamic ventilator strategies to meet the unique and often-changing requirements
of each patient.
September 2020 n Volume 34 Number 9 3
CASE PRESENTATIONS
■ CASE ONE with increasing inspiratory pressure Supplemental oxygen is continued;
support to 20/5 cm H 2 O. Despite these an IV is established; and a 30-mL/kg
A 66-year-old woman with
interventions, she does not improve — normal saline fluid bolus and broad-
COPD, morbid obesity, and tobacco
as evidenced by worsening hypercapnia spectrum antibiotics, including
use presents via ambulance in
with a PaCO 2 of 115 and increasing vancomycin and piperacillin-
severe respiratory distress. Prior
somnolence. Subsequently, she is tazobactam, are initiated.
to arrival, EMS established an IV
intubated via rapid-sequence intubation Laboratory tests were initiated,
and administered three rounds of
(RSI) and placed on mechanical including a CBC with differential,
nebulized albuterol and 125 mg IV
ventilation. The ICU is full, so the blood cultures, and lactate and ABG
methylprednisolone. On arrival,
patient will be boarded for multiple measurements. A portable chest
she is placed on bilevel positive-
hours prior to transfer. x-ray reveals bilateral diffuse patchy
airway pressure (BiPAP) with
infiltrates with air bronchograms
pressure support of 10/5 cm H 2 O. ■ CASE TWO
Her initial vital signs are blood that are worse at the bases. The
A 19-year-old man with no medical
pressure 134/88, heart rate 122, patient’s hypotension improves
history presents in respiratory distress.
respiratory rate 38, temperature over the next 5 minutes after the
He has had multiple sick contacts over
36.8°C (98.2°F), and SpO 2 94% on the last 5 days and flu-like symptoms administration of fluid, but he
2 L/min supplemental oxygen via that have progressed over the last remains hypoxic despite receiving
nasal cannula. 48 hours. On arrival, he appears supplemental oxygen.
Two grams of IV magnesium diaphoretic and is in obvious distress, He is intubated via RSI, and an
sulfate and three rounds of nebulized with audible expiratory wheezes, endotracheal tube is placed. Despite
ipratropium bromide and albuterol rhonchi midway up the thorax, and maximal FiO2 , the patient’s oxygen
sulfate are administered. Laboratory bilateral intercostal and subcostal saturation remains in the mid-80s.
tests, including a CBC and ABG retractions. His initial vital signs The decision is made to transfer him
measurement, are administered; are blood pressure 82/40, heart rate to the nearest ICU, but critical care
a chest x-ray is unremarkable 138, respiratory rate 51, temperature transport is approximately 90 minutes
aside from hyperinflated lungs. 39.1°C (102.4°F), and SpO2 84% on away due to suboptimal weather
The patient is continued on BiPAP a nonrebreather mask at 15 L/min. conditions.
CRITICAL DECISION as the goal of mechanical support is to set peak pressure, further reducing the
temporarily match physiologic conditions chances of VALI. However, VC keeps
What initial ventilator strategies
as closely as possible (Figure 1). pressure as the dependent variable in
are most appropriate after When selecting an ideal ventilator flux, which is historically considered
emergent intubation? mode for patients in acute respiratory a risk factor for injury if the airway
There are four indications for failure, both pressure-controlled (PC) pressure is elevated in a system with
emergent intubation based on varying and volume-controlled (VC) settings less compliance, increased resistance,
pathophysiologies: airway protection have been used. A recent meta-analysis or acute active expiration, such as
(eg, safety of procedures, depressed of 34 small studies comparing PC and excessive coughing.5
mental status, severe agitation, expected VC modes found no difference in the When intubating for the purpose
clinical course, transport), hypercapnia, work of breathing, oxygenation/gas of airway protection, VC ventilation
hypoxia, and excessive respiratory exchange, compliance, hemodynamic settings are frequently appropriate, as a
load (eg, excessive work of breathing, stability, ICU mortality, and length of predetermined volume is administered
uncompensated acidosis, or shock).3 stay.4 over a given time period based on
Ventilator strategies should be tailored VC settings are easier to use the patient’s respiratory rate and
to each of these indications to maximize when implementing lung-protective VT, regardless of fluctuating airway
supportive measures, return patients to a strategies, avoid the risk of ventilator- pressures. Although this strategy
physiologically neutral state, and provide associated lung injuries (VALIs), and is appropriate for patients without
expedited extubation if possible. give clinicians total control over tidal active pulmonary disease, emergency
volume (VT), minute ventilation, and physicians must be cognizant of
Airway Protection minute volume. Additionally, assist- fluctuating airway pressures and act
The approach to ventilator controlled (AC) settings with a volume- accordingly, as the plateau pressure can
management in the setting of airway regulated strategy improve the work of change without a simultaneous change
protection is relatively straightforward, breathing and terminate inspiration at a in static VT.
4 Critical Decisions in Emergency Medicine
The most suitable care for patients exchange. Expiratory flow limitations Using a technique known as
who require airway protection and are the principal physiologic alterations “permissive hypercapnia,” combined
have no pre-existing lung or cardiac in most obstructive lung processes, VT and respiratory-rate strategies
pathologies is an overall lung-protective including COPD. Airflow obstruction, for obstructive processes that cause
strategy involving a VT of 6 to 8 mL/ low elastic recoil, high ventilatory hypercapnia should aim to normalize
kg based on ideal body weight (IBW), demand, and short expiratory time pH levels greater than 7.2, not PaCO2,
a respiratory rate of 12 to 16 breaths/ all result in air trapping.9 Therefore, to avoid further lung injury.9
minute, PEEP of 5 cm H2O, and titration ventilator settings in patients with When attempting to normalize
of FiO2 to a goal SpO2 of 92% to 99%, obstructive processes are tailored PaCO2, excessive respiratory rates and
while avoiding excessive oxygenation to minimize hyperinflation, rest VTs can worsen existing lung damage.
(Table 1). compromised respiratory muscles, and Like any technique, there are caveats
Hyperventilation is one important allow adequate expiration. to permissive hypercapnia. Absolute
caveat regarding ventilator management Ventilation is measured, from a contraindications include pregnancy,
in patients with traumatic head injuries physiologic perspective, by calculating pulmonary hypertension, salicylate
and resultant mental status depression. the minute ventilation, which is defined and tricyclic antidepressant toxicities,
Lung-protective mechanical ventilation as the respiratory rate multiplied by the and increased intracranial pressure,
strategies with a VT of 6 to 8 mL/kg VT. Hypercapnia stems from disease in which case a PaCO2 level near 35
and goal normocapnia have been shown processes in which the respiratory rate has been shown to improve patient
to provide the best results, including a and VT are ineffective at adequately outcomes.12,13
reduction in direct injuries to the lung removing CO2. Therefore, when Oxygen titration in nonhypoxemic
and improved neurologic outcomes.6 considering initial ventilator strategies mechanically ventilated patients should
Limited antiquated evidence suggests for hypercapnia, VC ventilator modes be initiated early to avoid inadvertent
that hyperventilation may reduce are suitable.9,10 oxygen toxicity. Due to the theoretical
intracranial pressure.6 VT should be tailored based on the free radical damage that high levels of
However, current brain injury patient’s IBW in a manner similar to oxygen can produce, an initial FiO2 of
guidelines discourage the prophylactic airway-protective strategies, aiming for 100% is reasonable, with rapid titration
or prolonged use of hyperventilation 6 to 8 mL/kg. This approach allows of FiO2 to target an oxygen saturation
and endorse its temporary use only for adequate volume administration between 92% and 99% with a goal of
in the presence of acute neurologic
while avoiding high airway pressures, less than 60% FiO2.
deterioration, assuming an intervention
thereby decreasing the likelihood of If possible, positive end expiratory
to correct the underlying cause (eg,
lung injuries, alveoli rupture, or a pressure (PEEP) should be kept at or
mass lesion evacuation) is planned.
pneumothorax. below 5 cm H2O to avoid barotrauma,
Thus, most patients with traumatic
Respiratory rate should ideally be particularly in patients with COPD
brain injuries should be kept within the
initiated at 16 to 20 breaths/minute or other obstructive processes; in
normocapnic range using the ventilator
in order to approximate near-normal such cases, higher PEEP can worsen
settings previously described.7,8
physiologic conditions, allow time for outcomes and prolong ventilator-
Hypercapnia exhalation, and reduce breath stacking.11 dependence.11,14
Hypercapnia — which often results The inspiratory-to-expiratory time One potentially important caveat
from decreased central drive, reduced (I:E) ratio (ie, the relative time spent to consider regarding ventilator
strength, increased respiratory load in inspiration compared to expiration) management in those with obstructive
from poor compliance or narrow should be kept near 1:3, or even pathologies is noted in the difference
airways, or some combination extended to 1:4 or 1:5, to allow for between COPD and fixed-airway
thereof — causes CO2 retention and maximal expiratory time and further obstruction. Applying PEEP during the
a subsequent loss of effective gas help with CO2 elimination. ventilatory support of a patient with
TABLE 1. Indications and Initial Ventilator Settings for the Mechanically Ventilated Patient
Indication
Respiratory Rate PEEP
for Emergent Ventilator Mode VT FiO2
(breaths/min) (cm H2O)
Intubation
Airway protection Volume control 6-8 mL/kg 12-16 5 Titrate to goal SpO2 >92%
Hypercapnia Volume control 6-8 mL/kg 16-20 (with I:E ratio 1:3) ≤5 Titrate to goal SpO2 >92%
Hypoxemia Pressure control 6-8 mL/kg 12-16 8-10 Titrate as necessary
or volume control (in conjunction with PEEP) with a
goal SpO2 >92% and PaO2 >75
September 2020 n Volume 34 Number 9 5
TABLE 2. Titration Strategy for PEEP and FiO2 in Hypoxemia (ARDSnet)
Lower PEEP/Higher FiO2
FiO2 0.3 0.4 0.4 0.5 0.5 0.6 0.7 0.7 0.7 0.8 0.9 0.9 0.9 1.0
PEEP 5 5 8 8 10 10 10 12 14 14 14 16 18 18-24
Higher PEEP/Lower FiO2
FiO2 0.3 0.3 0.3 0.3 0.3 0.4 0.4 0.5 0.5 0.5-0.8 0.8 0.9 0.9 1.0
PEEP 5 8 10 12 14 14 16 16 18 20 22 22 22 24
fixed airflow obstruction, including the emergency department requires prolonged states of hyperoxia,
severe asthma and bronchospasm, may adequate sedation, proper monitoring, especially in cases of ARDS and other
produce potentially dangerous increases and specific attention to PEEP and space-occupying diagnoses.17,20
in lung volume, airway pressure, FiO2 titration, as these variables Starting at 100% FiO2 and
and intrathoracic pressure, causing are responsible for oxygenation in titrating to the most effective lower
circulatory compromise.11 hypoxemic respiratory failure. The dose is an acceptable initial treatment
This occurs because a larger drop goal should be to achieve an adequate strategy as long as the physician
in intrathoracic pressure is necessary increase in mean airway pressure intends to reduce FiO2 in a timely
to trigger subsequent breaths. Thus, to aid in alveoli recruitment while manner. Titration in cases of ARDS,
emergency physicians should be aware simultaneously avoiding excessive for instance, can be done using the
that the routine use of significant PEEP pressure increases that result in VALI. ARDSnet PEEP tables (Table 2). The
during ventilatory support of a patient Emergency physicians should use more effective strategy — which also
with acute fixed-airway obstruction caution when titrating FiO2 alone, as allows the FiO2 to be decreased in a
remains controversial and is not this will ultimately result in ineffective timelier manner — is to increasingly
recommended. increases in PaO2 and SpO2. This up-titrate the PEEP while reducing
Hypoxia problem is due to preferential shunting the FiO2 to target an SpO2 of more
after the prolonged use of FiO2 than 92%. An effective PEEP titration
Hypoxemic respiratory failure,
exceeding 50% to 60%. Moreover, strategy enables the patient to
defined as a PaO2 less than 60 mmHg
(8 kPa) or SpO2 less than 90%, is a free radical damage can occur during maintain alveolar patency, thereby
common reason for assisted mechanical
ventilation in the emergency setting.15,16 FIGURE 1. Stepwise Approach to Hypoxemic Ventilator Management
Initial ventilator management for
hypoxemic respiratory failure has VOLUME-CONTROLLED SETTING
evolved extensively in recent years. • VT 6-8 mL/kg IBW
The literature has generated a shift • PEEP 5-8 cm H2 O
• FiO2 100% with goal <60%
toward the use of early lung-protective
ventilator strategies for ARDS and is
considered safe and effective for nearly
all ventilated patients.14 Increase PEEP as needed while
maintaining plateau pressure
This approach has consequently <30 cm H2 O. Consider using
reduced mortality, decreased the ARDSnet tables if appropriate.
worsening of ARDS, and decreased
lung injuries from both pressure
and volume consequence during the Increase FiO2
duration of a patient’s ventilator Goal to maintain <60%
requirement.14,17-19
Given the advantages and
disadvantages for both VC and PC
Consider prone or Consider paralysis (rocuronium,
ventilator settings, either mode can
“good lung down” positioning vecuronium, cisatracurium)
be used when managing hypoxemic
patients, depending on the emergency
physician’s experience and comfort
level. • Consider a reversal of the I:E ratio
• Consider a consultation for ECMO
Achieving the best outcomes
in intubated hypoxemic patients in
6 Critical Decisions in Emergency Medicine
FIGURE 2. Ventilator Airway Pressure Graph
Plateau Pressure
Peak Inspiratory (Goal <30)
PRESSURE
Pressure (Goal <30)
AIRWAY
Driving
Pressure AutoPEEP
PEEP }
Inspiration Expiration Inspiration Inspiratory Expiration Expiratory Hold
Hold
TIME
preserving adequate gas exchange and physician’s job has arguably just To increase the specificity of
alveolar perfusion. Thus, PEEP should begun. Initial ventilator strategies colorimetric EtCO2, endotracheal
be factored in early when considering based on the indication for intubation intubation should only be confirmed
an increase in FiO2, especially those can often address the underlying after 5 to 6 breaths are given.
exceeding 50% to 60%. cause of respiratory failure. However, (Color changes may initially arise in
In cases of hypoxemic respiratory these situations can be highly dynamic esophageal intubations from the CO2
failure without an alveolar fluid- and require close monitoring. Without that can accumulate in the stomach.)
occupying state and otherwise normal instituting standard protocols for Although waveform capnography can
lung parenchyma (eg, intracardiac assessing every patient intubated in confirm successful tracheal intubation,
shunt), a physiologic respiratory rate is the emergency department, the risk of a postintubation chest x-ray is still
appropriate (ie, 12-16 breaths/min). morbidity and mortality is significant. warranted to verify that the tube is
PEEP settings targeting 8 to 10 mmHg Monitoring the intubated patient placed at an appropriate depth above the
in patients with normal lung function takes place in three parts: carina (ideally ~2 cm).
are appropriate. Protective lung 1. Confirmation of endotracheal An endotracheal tube that is too
volumes of 6 to 8 mL/kg of IBW positioning high (above the level of the clavicles)
remain, as this method has been shown 2. Assessment of initial ventilator risks accidental displacement, but tube
to reduce the progression to ARDS settings positioning that is too low will result in
and subsequent VALI.16 Theoretically, 3. Ongoing monitoring a mainstem intubation and collapse of
an FiO2 greater than 60% should be the opposite lung. Emergency physicians
Tube Placement
unnecessary in these instances. should also order medications to
The proper position of the
If higher FiO2 values are needed, promote adequate postintubation
endotracheal tube must always be
immediately evaluate for a new lung- analgesia and sedation. Once the tube
confirmed; in fact, many experts
occupying process, acutely worsening placement is confirmed, lifting the head
intra- or extracardiac shunt, or suggest that this confirmation is the
of the bed to 30 degrees can significantly
worsening ventilation/perfusion final procedural aspect of successful
decrease the risk of aspiration and
mismatch. endotracheal intubation. Waveform
further reduce morbidity.22
end-tidal carbon dioxide (EtCO2)
CRITICAL DECISION monitoring is the ideal way to confirm Ventilator Settings
that an endotracheal tube is in the Next, several simple maneuvers are
How should intubated patients
trachea.21 Although many emergency required to assess whether the initial
be monitored in the emergency
departments use colorimetric EtCO2, ventilator settings are appropriate for
department? care must be taken; there are multiple the patient. Ideally, a lung-protective
Once a patient has been placed on reports of false-positives when using VT of 6 to 8 mL/kg is set based on the
mechanical ventilation, the emergency this method. patient’s IBW. When specific volumes
September 2020 n Volume 34 Number 9 7
are set on the ventilator, the airway PC ventilation mode. To prevent lung If VBG will be used to monitor
pressures differ from breath-to- injury, the PIP (and plateau pressure, the impact of ventilator settings,
breath depending on many variables, as needed) should be assessed after any carefully titrate the settings to produce
including the compliance of the changes to the ventilator settings. an SpO2 of 92% to 99%.23 Evolving
lung and resistance of the airways. evidence demonstrates the negative
Continued Monitoring
Barotrauma, which results when impact of hyperoxia on a variety of
After the patient’s initial ventilator
airway pressures exceed 30 mmHg, disease states ranging from traumatic
settings are deemed appropriate, it
has been shown to increase mortality brain injuries to cardiac arrest, so
is vital to continue monitoring the
in the ARDSnet trial.17 it is important to avoid an SpO2 of
patient closely. Quantitative waveform
Assessing peak inspiratory 100% when treating any ventilated
capnography should be continued
pressures (PIP) on the initial ventilator patient.24-26
beyond the initial confirmation of
settings to ensure that they are less
than 30 mmHg may prevent significant
endotracheal tube placement because it CRITICAL DECISION
can be an excellent window into what is
downstream lung injuries. If the PIP is What strategies are available
happening to the patient.
above 30 mmHg, measure the plateau for patients who fail to
The flow of expired CO2 can
pressure by completing an inspiratory adequately ventilate?
be used to diagnose any number of
hold on the ventilator for roughly
pathologies, including altered cardiac Troubleshooting acute
1 second to allow the pressure to
output, increased airway resistance, hypercapnic respiratory failure is a
equilibrate between the small airways
and decreased lung compliance. task all emergency physicians must
and alveoli.
Thus, not only is EtCO2 effective for be comfortable performing. When a
Plateau pressure is the best
continually monitoring appropriate patient’s CO2 level remains elevated
approximation of the pressure that
placement of the endotracheal tube, despite the use of suitable ventilator
the alveoli are truly experiencing
but it can also be a dynamic tool for settings, the respiratory rate is the
on a breath-to-breath basis. If the
assessing hemodynamic and ventilatory first parameter to adjust, as it has
plateau pressure is above 30 mmHg,
variables when caring for critically ill the greatest impact on gas exchange
barotrauma is likely, which can
patients in respiratory failure. and results in less alveoli damage and
contribute to mortality and morbidity.
A mechanically ventilated barotrauma than initially modifying
Emergency physicians should note
patient’s response to the ventilator VT.
that plateau pressure values must
settings should be evaluated within Hypercapnic respiratory failure
be monitored regularly (every 30-60
approximately 30 minutes. This and obstructive lung disorders
minutes, or with any high-pressure
response is ideally assessed with an involve dynamic hyperinflation, a
ventilator alarms), especially in the
ABG measurement, which can provide process in which a new breath often
early phase of the AC/VC ventilation
a comprehensive snapshot of the begins before the lung has reached
mode (Figure 2).
patient’s oxygenation, ventilation, the static equilibrium volume.9 This
There are two broad categories
and basic metabolic parameters, such dynamic results in increasingly
that can cause high PIP. The first,
as the pH value. However, multiple larger lung volumes and subsequent
increased airway resistance, leads to
studies have demonstrated that venous intrathoracic pressures, which worsens
increased PIPs but normal plateau
blood gases (VBG) can approximate hemodynamic compromise and can
pressures during the inspiratory hold.
ABG values if oxygenation is not a cause difficulties when managing the
Airway-resistance issues can be caused
concern. initial hypercapnia.
by an obstructed endotracheal tube,
dyssynchrony with the ventilator,
mucous plugs, or bronchospasm.
These potential causes should be
assessed. Alternatively, if both the PIP
and plateau pressure are elevated, the
problem likely stems from decreased
compliance of the lung. n Titrate the FiO2 and PEEP using the ARDSnet PEEP table with a goal SpO2 of
92% to 99% to avoid both hypoxia and hyperoxia, as both negatively impact
Causes of decreased lung
critically ill patients.
compliance are plentiful and include
n Use quantitative waveform EtCO2 to confirm endotracheal intubation.
infiltrative processes like edema,
Consider this approach for multiple physiologic conditions that affect
ARDS, pneumothorax, and obesity. mechanically ventilated patients.
Plateau pressure can be reduced by n When dealing with refractory hypercapnia, hypoxia, or significant ventilator
decreasing the VT (to as low as 4 mL/ dyssynchrony, it is important to optimize analgesia and sedation. Consider the
kg), increasing sedation, considering use of neuromuscular blockade to achieve the goals of mechanical ventilation.
chemical paralysis, or switching to a
8 Critical Decisions in Emergency Medicine
particularly in situations associated
TABLE 3. The DOPES Mnemonic for Hypoxic Ventilator Troubleshooting with upper-airway obstruction.11
Heliox has been shown to reduce
D Displacement of the tube
dynamic hyperinflation by 15%,
O Obstruction of the tube (kinks and mucus plugs) placing the respiratory muscles at a
P Pneumothorax better mechanical advantage.27 The
drug has also been shown to decrease
E Equipment failure
intrathoracic pressures and may be an
S Stacked breaths (may require disconnecting with manual assist attractive option for COPD patients
exhalation) with dynamic hyperinflation who are
failing to appropriately ventilate.
Calibrating the respiratory rate is patient’s presenting complaints and The correction of electrolyte
the safest and most reliable option for identifying the underlying issue. deficiencies, including hypokalemia
improving CO2 retention. Emergency Additional strategies for and hypophosphatemia, can help
physicians should only consider raising maintaining adequate ventilation may improve neuromuscular strength.
a patient’s VT after the respiratory include pain control with fentanyl The resulting mechanism improves
rate has been optimized to avoid the (analgosedation); the administration ventilation through enhanced
significant risk of barotrauma and of dexmedetomidine for delirium, respiratory muscle recruitment.28
worsening the already-poor elastic when applicable; and increased Neuromuscular-blockade
recoil present in most obstructive sedation with medications such as agents — particularly long-acting
processes. Notably, the end goal of midazolam or propofol. formularies like rocuronium and
modifying a patient’s respiratory rate Ventilator dyssynchrony may also cisatracurium — have been shown
and VT is a pH greater than 7.2 (not result from air hunger, inappropriate to provide additional benefits when
normocapnia), as defining normal pH low-minute ventilation or PEEP, or establishing ventilator synchrony
has been shown to improve outcomes.9 “breath stacking.” Therefore, a solid and optimal minute ventilation.29
Multiple strategies aimed at understanding of ventilator mechanics Status asthmaticus can pose particular
treating hypercapnia involve VC is paramount for attaining an challenges because these patients
support with a fixed flow-rate pattern. effective solution. Interventions may are routinely difficult to ventilate
Asynchrony between mandatory include increasing the flow rate, the despite appropriate settings. Such
and spontaneous patient-initiated inspiratory time, or PEEP (assuming
cases routinely warrant deep sedation
breaths is a major disadvantage that it is a safe option based on the
immediately after RSI in addition to
can lead to inadequate ventilation. indications for intubation).
neuromuscular blockade with a long-
This asynchrony can originate from Helium-oxygen (Heliox) is
acting paralytic.29
agitation, otherwise known as another adjunctive therapy that has
Finally, the use of veno-
“bucking the vent,” and can indicate proven beneficial for the management
venous extracorporeal membrane
a primary pathologic state like pain, of inadequately ventilated patients.
oxygenation (VV-ECMO) for
anxiety, hypoglycemia, intracranial Because airway turbulence is
hemorrhage, or alcohol withdrawal, dependent on density, Heliox’s lower the management of refractory
among others. The management of density decreases airway resistance hypercapnic respiratory failure has
these situations should focus on the and improves the work of breathing, gained renewed interest.30 Indications
for VV-ECMO, which can be
found in the Extracorporeal Life
Support Organization guidelines,
include failure to oxygenate, severe
CO2 retention or the inability to
maintain acceptable CO2 levels
at safe airway pressures (plateau
n Neglecting to use lung-protective ventilation (6-8 mL/kg of IBW), a mistake
pressure <30 cm H2O), and severe
that can increase the morbidity and mortality of ventilated patients.
air-leak syndromes.31 Emergency
n Relying on FiO 2 alone to promote oxygenation for hypoxic, ventilated
physicians should consider an early
patients. Instead, titrate PEEP to help decrease the FiO 2 and prevent
further lung damage. surgical consultation regarding the
potential use of ECMO or a transfer
n Being unaware of high peak and plateau pressures (>30 mmHg) in
ventilated patients, an oversight that can lead to ongoing lung damage and to a facility that is well versed in
other significant complications. this potentially life-saving adjunctive
therapy.
September 2020 n Volume 34 Number 9 9
CRITICAL DECISION <300 mmHg) and represents part of the of perfusion when a person is lying
diagnostic criteria for ARDS. down. Consequently, ventilation of
What strategies are available for
the affected dorsal regions is also
patients who fail to adequately FiO2 and PEEP
diminished. Prone positioning is
oxygenate? In VC mode, increases in FiO2 and
believed to reverses these trends via the
PEEP are the only two factors affecting
Refractory or persistent hypoxemia gravitational effects of recruiting lung
adequate oxygenation and the eventual
is a common phenomenon following units and by enhancing ventilation and
resolution of refractory hypoxemia. perfusion matching.
intubation. Given that more than
Depending on the diagnosis, FiO2 and Although prone positioning
80% of ARDS patients will require
PEEP should be titrated together when is uncommon in the emergency
intubation, identifying and treating
managing patients with ARDS (using department, it may be an effective
refractory hypoxemia earlier is
the ARDSnet table) or independently option for persistently hypoxemic
more beneficial.18 The principles of
with otherwise normal or close-to- patients, particularly in light of
the early recognition and treatment
normal lung parenchyma. In ARDS, increasing wait times for ICU beds
of a persistently poor oxygenation
PEEP has the ability to improve the nationwide. If prone positioning
state should be balanced with well-
PaO2/FiO2 ratio by recruiting alveoli. remains too substantial of a physical
established data concerning hyperoxia
Its use has also been shown to prevent or logistical burden, a strategy that
in critically ill patients.
further refractory hypoxemia and positions the best-aerated lung down is
Detriments owed to hyperoxia
include but are not limited to fewer decrease the use of other rescue another viable option. The “good lung
ventilator-free days, increased episodes therapies. down” technique enables improvement
of shock, liver failure, bacteremia, In those with acute lung injuries or in the distal aeration and recruitment
and increased hospital mortality.24-26 unilateral disease, more judicious use is of the lung-occupying additional dead
As such, emergency physicians advised to avoid the overdistention of space (ie, the more injured lung).
should ensure that the corrections normal, functional lung parenchyma.
If no response to PEEP titration is seen Other Strategies
for a refractory hypoxic state are not
over the course of a 30-minute trial, Lung-recruitment maneuvers
overcorrections that actually permit
continued titration can be attempted; (eg, sighing and short-duration PEEP
persistent hyperoxia.
however, alternate avenues should trials) are subject to recruitment
When identifying a state of
be considered early in the patient’s variability and must be done under close
refractory hypoxia, the physician
course.18 observation, especially during the initial
should first ensure adequate settings
implementation phase.18,30 Alternative
and avoid obvious pulmonary- Neuromuscular Blockade ventilator strategies, including high-
circuit malfunctions, either via the Neuromuscular blockade is a frequency oscillator ventilation;
machinery or by changing the patient’s useful tool for mechanically supported pulmonary vasodilators; VV-ECMO;
physiology. The DOPES mnemonic is patients, especially those with refractory and inverse ratio ventilation, in which
one screening tool that can facilitate hypoxemia because it allows external inspiratory time is increased at the
an efficient bedside analysis (Table 3). control of the patient’s respiratory expense of a decrease in expiratory time,
Notably, extra care should be taken to cycling. The early use of neuromuscular can also be attempted.
choose ventilator settings that do not blockade may improve oxygenation, These methods are largely found
encourage breath stacking (ie, auto- 90-day mortality, and total days off of in ICU care and are not always easily
PEEP), a complication that can lead mechanical ventilation in hospitalized executed in the emergency setting;
to cardiovascular collapse, worsened patients with ARDS.32-33 Although a nevertheless, recognition of these
respiratory status, and eventual arrest more recent trial has called the overall adjuvant therapies remains an important
if not recognized quickly. If breath
benefit of paralysis into question, aspect to improved patient care.
stacking does occur, disconnect the
this approach can certainly enhance
endotracheal tube from the circuit, Summary
oxygenation in hypoxic patients.34
allow full exhalation, and down-titrate Few interventions in the emergency
the VT if needed until an adequate Patient Positioning setting have such an immediate and
plateau pressure (<30 cm H2O) is Prone positioning has shown dramatic impact on the mortality and
achieved. benefit for the treatment of early downstream morbidity of critically ill
Traditionally, hypoxemia on an ARDS, with decreased progression patients as endotracheal intubation
ABG measurement is defined as a PaO2 to ECMO, improved PaO2/FiO2, and and mechanical ventilation. The
less than 80 mmHg; a normal expected improved 28- and 90-day mortality indications for ventilatory support can
value is between 80 and 100 mmHg. rates.35 Supine positioning causes direct initially guide a patient’s ventilator
Noting that PaO2 rises with elevations compression of lung tissue in the most settings, but acute respiratory failure
in FiO2, the PaO2/FiO2 ratio can be posterior aspects of the lungs, which remains a dynamic disease process
calculated (with abnormal being also receive the highest proportion that requires the close monitoring
10 Critical Decisions in Emergency Medicine
CASE RESOLUTIONS
■ CASE ONE pressure of 35 cm H 2O, and the patient based on the ARDSnet table. A repeat
After undergoing endotracheal was suctioned without improvement. chest x-ray showed no signs of a
intubation, the elderly woman A chest x-ray showed no pneumo pneumothorax.
was connected to the mechanical thorax. The patient was disconnected Despite these interventions,
ventilator on VC mode with the from the ventilator for 5 seconds and the patient’s ABG level marginally
following settings based on her IBW reconnected; this improved her peak improved to show a PaO2 of 55 mmHg
of 65 kg: VT 455 mL, respiratory pressures, indicating critical breath and an SpO2 of 89%. His respiratory
rate 14, PEEP 5 mmHg, and FiO 2 stacking. Subsequently, the I:E ratio mechanics were monitored, and his
80%. The endotracheal tube was prolonged and no further alarm PIP was found to be greater than
placement was confirmed with an incidents were noted. She was admitted 30 mmHg with a plateau pressure
EtCO 2 of 35 mmHg after 5 to 6 to the ICU and successfully extubated of 41 mmHg, indicating severe
breaths on the ventilator, and a the following day. She was discharged ARDS based on his chest x-ray and
chest x-ray showed the distal tip to from the hospital 5 days later with severe hypoxemia. Consequently,
be 1.5 cm above the carina. Sedation normal work of breathing. neuromuscular blockade was
was initiated with propofol. introduced with a bolus dose of
Fifteen minutes after the initial ■ CASE TWO rocuronium.
ventilator settings were placed, an After successful intubation, the An ABG measurement showed
ABG measurement revealed a pH young man was connected to the some improvement in the patient's
of 7.14, PaCO2 of 90 mmHg, and a ventilator on VC mode with the oxygenation status, so the decision
PaO2 of 182 mmHg. The respiratory following settings based on his IBW was made to transfer him to an
rate on the ventilator was increased of 75 kg: VT 525 mL, respiratory rate ECMO-capable tertiary facility. He
to 20 breaths/minute, and the 14 breaths/minute, PEEP 8 mmHg, remained hypoxic upon admission
FiO2 was titrated to 40% to avoid and FiO2 100%. A propofol infusion and was put in the prone position to
hyperoxia. A repeat ABG test 30 was initiated for sedation. His SpO2 help with lung recruitment. He was
minutes after these changes revealed remained 87% after intubation, and ultimately placed on VV-ECMO and
a pH of 7.40, PaCO2 of 55 mmHg, a subsequent ABG measurement successfully decannulated 10 days
and PaO2 of 94 mmHg. Twenty 15 minutes later revealed a PaO2 later. He was later discharged from
minutes later, the ventilator alarm of 45 mmHg, indicating persistent the hospital to an acute rehabilitation
indicated high peak pressures. An hypoxemia. His PEEP was titrated up facility, where he required respiratory
inspiratory hold was performed, to 12 mmHg and gradually increased support with 2 L oxygen via nasal
which revealed an elevated plateau over the next 90 minutes to 24 mmHg cannula.
of multiple physiologic parameters respiratory support can help optimize and Critical Care. Guidelines for the management
of severe head injury. J Neurotrauma. 1996 Nov;13:
to ensure appropriate oxygenation the ventilator management provided in 641-734.
9. Ward NS, Dushay KM. Clinical concise review:
and ventilation. The careful even the most tenuous of situations. mechanical ventilation of patients with chronic
obstructive pulmonary disease. Crit Care Med. 2008
monitoring of abnormalities in patient May;36(5):1614-1619.
hemodynamics, ventilator waveforms, REFERENCES 10. Rose L. Clinical application of ventilator modes:
1. Stefan MS, Shieh MS, Pekow PS, et al. Epidemiology ventilatory strategies for lung protection. Aust Crit
and blood gas values improves the and outcomes of acute respiratory failure in the Care. 2010 May;23(2):71-80.
United States, 2001 – 2009: a national survey. J Hosp 11. Ahmed SM, Athar M. Mechanical ventilation in
quality of care and facilitates the early Med. 2013 Feb;8(2):76-82. patients with chronic obstructive pulmonary
initiation of adjunctive therapy when 2. Cardoso LTQ, Grion CMC, Matsuo T, et al. Impact disease and bronchial asthma. Indian J Anaesthesia.
of delayed admission to intensive care units on 2015 Sep;59(9):589-598.
other oxygenation and ventilation mortality of critically ill patients: a cohort study. 12. Flomenbaum NE. Salicylates. In: Nelson LS, Lewin
Crit Care. 2011;15(1):R28. NA, Howland MA, Hoffman RS, Goldfrank LR,
strategies fail. 3. Graham CA. Emergency department airway Flomenbaum NE, eds. Goldfrank’s Toxicologic
management in the UK. J R Soc Med. 2005 Emergencies. 9th ed. McGraw-Hill; 2011:508-520.
A stepwise approach to ensuring Mar;98(3):107-110. 13. Chonghaile NM, Higgins B, Laffey JG. Permissive
ideal ventilator settings, including 4. Rittayami N, Katsios DM, Beloncle F, Friedrich JO, hypercapnia: role in protective lung ventilatory
Mancebo J, Brochard L. Pressure controlled vs volume strategies. Curr Opin Crit Care. 2005 Feb;11(1):
confirmation of the endotracheal tube controlled ventilation in acute respiratory failure. 56-62.
A physiology based narrative and systemic review. 14. Neto AS, Cardoso SO, Manetta JA, et al.
position, enables the early identification CHEST. 2015 Aug;148(2):340-355. Association between use of lung protective
5. Campbell RS, Davis BR. Pressure-controlled versus
of persistently hypercapnic or hypoxic volume-controlled ventilation: does it matter? Respir
ventilation with lower tidal volumes and clinical
outcomes among patients without acute respiratory
patients, thereby allowing clinicians Care. 2002 Apr;47(4):416-424. distress syndrome: a meta-analysis. JAMA. 2012
6. Marion DW, Firlik A, McLaughlin MR. Hyperventilation Oct 24;308(16):1651-1659.
to effectively implement changes to therapy for severe traumatic brain injury. New Horiz. 15. Nee PA, Al-Jubouri MA, Gray AJ, O’Donnell
1995 Aug;3(3):439-447. C, Strong D. Critical care in the emergency
the clinical course. Understanding the 7. Maung AA, Kaplan LJ. Mechanical ventilation after department: acute respiratory failure. Emerg Med J.
basics of respiratory mechanics and injury. J Intensive Care Med. 2014;29:128-137. 2011 Feb;28:94-97.
8. Brain Trauma Foundation, American Association of 16. Sutherasan Y, Vargas M, Pelosi P. Protective
having a keen eye for fluctuations in Neurological Surgeons, Joint Section on Neurotrauma mechanical ventilation in the non-injured lung:
September 2020 n Volume 34 Number 9 11
review and meta-analysis. Crit Care. 2014 Mar
18;18(2):211.
17. Acute Respiratory Distress Syndrome Network;
Brower RG, Matthay MA, Morris A, Schoenfeld
D, Thompson BT, Wheeler A. Ventilation with
lower tidal volumes as compared with traditional
tidal volumes for acute lung injury and the acute
respiratory distress syndrome. ARDS Net. N Engl J
Med. 2000 May 4;342(18):1301-1308.
18. Esan A, Hess DR, Raoof S, George L, Sessler CN.
Severe hypoxemic respiratory failure: part 1 --
ventilatory strategies. CHEST. 2010 May;137(5):
1203-1216.
19. Needham DM, Colantuoni E, Mendez-Tellez PA, et al.
Lung protective mechanical ventilation and two year
survival in patients with acute lung injury: prospective
cohort study. BMJ. 2012 Feb 27;344:e2124.
20. West JB, Luks AM, eds. West’s Respiratory
Physiology: The Essentials. 10th ed. Wolters Kluwer;
2016.
21. Silvestri S, Ladde JG, Brown JF, et al. Endotracheal
tube placement confirmation: 100% sensitivity and
specificity with sustained four-phase capnographic
waveforms in a cadaveric experimental model.
Resuscitation. 2017 Jun;115:192-198.
22. Muscadere J, Dodek P, Keenan S, Fowler R, Cook
D, Heyland D; VAP Guidelines Committee and the
Canadian Critical Care Trials Group. Comprehensive
evidence-based clinical practice guidelines for
ventilator-associated pneumonia: prevention. J Crit
Care. 2008 Mar;23(1):126-137.
23. Zeserson E, Goodgame B, Hess JD, et al.
Correlation of venous blood gas and pulse oximetry
with arterial blood gas in the undifferentiated
critically ill patient. J Intensive Care Med. 2018
Mar;33(3):176-181.
24. de Jonge E, Peelen L, Keijzers PJ, et al. Association
between administered oxygen, arterial partial
oxygen pressure and mortality in mechanically
ventilated intensive care unit patients. Critical Care.
2008 Dec 10;12(6):R156.
25. Helmerhorst HJF, Arts DL, Schultz MJ, et al. Metrics
of arterial hyperoxia and associated outcomes in
critical care. Crit Care Med. 2017 Feb;45(2):187-195.
26. Vincent JL, Taccone FS, He X. Harmful effects
of hyperoxia in postcardiac arrest, sepsis,
traumatic brain injury, or stroke: the importance of
individualized oxygen therapy in critically ill patients.
Can Respir J. 2017 Jan 26;2017:2834956.
27. Swidwa DM, Montenegro HD, Goldman MD, Lutchen
KR, Saidel GM. Helium-oxygen breathing in severe
chronic obstructive pulmonary disease. CHEST. 1985
Jul;87(6):790-795.
28. Ackerman GL, Arruda, JL. Acid-base and electrolyte
imbalance in respiratory failure. Med Clin North Am.
1983 May;67(3):645-656.
29. Wright BJ. Lung-protective ventilation strategies and
adjunctive treatments for the emergency medicine
patient with acute respiratory failure. Emerg Med Clin
North Am. 2014 Nov;32(4):871-887.
30. Peek GJ, Mugford M, Tiruvoipati R, et al; CESAR trial
collaboration. Efficacy and economic assessment of
conventional ventilatory support versus extracorporeal
membrane oxygenation for severe adult respiratory
failure (CESAR): a multicentre randomised controlled
trial. Lancet. 2009 Oct 17;374(9698):1351-1363.
31. Extracorporeal Life Support Organization (ELSO).
General Guidelines for all ECLS Cases. ELSO.
Published August 2017. https://www.elso.org/
Portals/0/ELSO%20Guidelines%20General%20All%20
ECLS%20Version%201_4.pdf
32. Papazian L, Forel JM, Gacouin A, et al; ACURASYS
Study Investigators. Neuromuscular blockers in
early acute respiratory distress syndrome. N Engl J
Med. 2010 Sep;363(12):1107-1116.
33. Mosier JM, Hypes C, Joshi R, Whitmore,
Parthasarathy S, Cairns CB. Ventilator strategies
and rescue therapies for management of acute
respiratory failure in the emergency department.
Ann Emerg Med. 2015 Nov;66(5):529-541.
34. The National Heart, Lung, and Blood Institute PETAL
Clinical Trial Network. Early neuromuscular blockade
in the acute respiratory distress syndrome. N Engl J
Med. 2019 May 23;380(21):1997-2008.
35. Guérin C, Reignier J, Richard JC, et al; for the
PROSEVA Study Group. Prone positioning in severe
acute respiratory distress syndrome. N Engl J Med.
2013 Jun 6;368(23):2159-2168.
12 Critical Decisions in Emergency Medicine
Clearing
the Air
Avoiding Postintubation
Complications
LESSON 13
By Matthew R. Dettmer, MD
Dr. Dettmer is an emergency and critical care physician at the Cleveland Clinic in
Cleveland, OH.
Reviewed by Sharon E. Mace, MD, FACEP
OBJECTIVES
On completion of this lesson, you should be able to: CRITICAL DECISIONS
1. Explain the physiological changes triggered by induction
n Which patients are at risk for postintubation
and intubation.
2. Name the main factors that raise a patient’s risk of hypotension?
postintubation complications. n How can the risk of postintubation hypotension be
3. Discuss the pros and cons of various induction agents and reduced?
preoxygenation techniques.
n How can postintubation hypoxemia be limited?
4. Describe the best tactics for intubating patients with COPD
and metabolic acidosis. n When and how should patients with metabolic
5. Recognize and respond appropriately to lung pressure acidosis be intubated?
buildup in a ventilated patient. n How should patients with obstructive lung disease
be intubated and monitored?
FROM THE EM MODEL
19.0 Procedures and Skills Integral to the Practice
of Emergency Medicine
19.1 Airway Techniques
19.1.1 Intubation
Endotracheal intubation is a common procedure both inside and outside the emergency department; however, many
patients who require emergency intubation are already critically ill, placing them at heightened risk for life-threatening
complications. Although postintubation complications can never be prevented completely, identifying the highest-risk
patients and understanding the most appropriate tactics for intubation can reduce the likelihood of deleterious effects.
July 2021 n Volume 35 Number 7 3
CASE PRESENTATIONS
■ CASE ONE with a respiratory rate of 30 and of 130. A second lactate test shows
SpO 2 of 93% on FiO 2 of 0.6, and he is no change since the initial exam. The
A 62-year-old man presents
via ambulance with shortness of beginning to appear fatigued and less patient becomes increasingly drowsy
breath. He is in significant distress responsive. and seems to be struggling harder to
and unable to answer questions, but breathe.
■ CASE TWO
his medical records reveal a history
A 38-year-old woman with no ■ CASE THREE
of hypertension, diabetes mellitus,
significant medical history presents A 52-year-old man with a history
and congestive heart failure with
with fever and lethargy. The patient’s of COPD, multiple hospitalizations,
reduced systolic function. His most
wife explains that the patient has and three previous intubations presents
recent ejection fraction was 45%.
experienced 2 days of worsening nausea in severe respiratory distress. He is
The patient’s wife says that he ran
and vomiting that did not improve with diaphoretic and breathing 30 times
out of his medications several weeks
ago and has had increasing difficulty antiemetics prescribed by her primary per minute. His vital signs are blood
breathing since then. His vital care doctor. The patient’s vital signs are pressure 162/92, heart rate 124, and
signs are blood pressure 180/110, blood pressure 92/50, heart rate 132, temperature 37.8ºC (100ºF). A lung
heart rate 122, respiratory rate 32, respiratory rate 44, temperature 39.1ºC exam reveals diffuse wheezing with
temperature 37.6ºC (99.7ºF), and (102.4ºF), and SpO2 90% on 2 L nasal a prolonged expiratory phase. A
SpO 2 82% on 6 L nasal cannula. cannula. On physical examination, she venous blood gas obtained on arrival
The patient is diaphoretic appears fatigued and demonstrates high shows a pH of 7.15 and PCO2 of 80,
and in severe respiratory distress, work of breathing. She is tachycardic indicating acute respiratory acidosis.
but his neurological function with a regular rhythm and has clear The patient is placed on noninvasive
appears normal. A physical exam lungs on auscultation. Her abdomen positive pressure ventilation with an
reveals tachycardia with a regular is soft but tender to the touch in the inspiratory pressure of 12 cm H 2 O and
rhythm, diffuse crackles on lung suprapubic area. A point-of-care expiratory pressure of 5 cm H 2 O. He is
auscultation, and pitting edema in lactate is 4.7 mmol/L, and urinalysis given intravenous methylprednisolone
both lower extremities. The patient is negative for pregnancy but shows and placed on continuous inhaled
is placed on noninvasive positive evidence of UTI. bronchodilators. After 30 minutes,
pressure ventilation, started on a The patient is given intravenous a repeat blood gas shows worsening
nitroglycerine infusion, and given antibiotics and 3 L of crystalloid fluids, respiratory acidosis, with a pH of 7.12
intravenous diuretics. Despite these but she remains tachycardic with a and PCO2 of 85. On reassessment, the
interventions, he remains tachypneic blood pressure of 103/57 and heart rate patient appears increasingly lethargic.
Introduction CRITICAL DECISION retrospective cohort study found that
Airway management is a fundamental in hemodynamically stable patients
Which patients are at risk for
skill for emergency physicians. who underwent emergency intubation,
postintubation hypotension? patients with a shock index of >0.8
Intubations are typically successful when
they occur in controlled settings, such Life-threatening hypotension is before the procedure were at the greatest
as in preparation for a planned surgery, relatively common after emergent risk for postintubation hypotension.6
intubation, complicating between Shock index is calculated by dividing
but emergency endotracheal intubation
15% and 28% of procedures.2,3 heart rate by systolic blood pressure
carries a higher risk of poor outcomes
Unsurprisingly, preintubation (Figure 1). Additional risk factors
in the period immediately following
hypotension is a strong predictor of include baseline hemodynamic
the procedure. Patients who require
postintubation hypotension; however, compromise and right ventricular
emergency airway management are often
certain patients with normal blood dysfunction.
already in severe physiological distress,
pressure are also at high risk of
heightening the risk of postintubation CRITICAL DECISION
postintubation hypotension and may
complications such as hypotension,
therefore benefit from additional How can the risk of
hypoxemia, and cardiac arrest.1 To treat resuscitation.3-5 A single-center
these patients, emergency physicians must
postintubation hypotension
understand the potentially deleterious be reduced?
physiological effects of endotracheal FIGURE 1. Calculate Shock Index To understand potential
intubation and master the techniques that Heart Rate interventions to prevent hypotension,
can help mitigate these effects in patients Systolic Blood Pressure it is important to first understand the
who are critically ill. physiological changes that occur with
4 Critical Decisions in Emergency Medicine
preoxygenation in patients who require
FIGURE 2. Preoxygenation with NIPPV intubation (Figure 2).10 In a study of 53
consecutive ICU patients who underwent
preoxygenation with either NRBs or
NIPPV before intubation, only 1 patient
in the NIPPV cohort experienced
postintubation oxygen desaturation to
below 92% compared to 8 patients in the
NRB cohort.11 There were no differences
in episodes of regurgitation or aspiration
between the two groups. It is unclear
why NIPPV led to better outcomes than
NRBs, but it may be because NIPPV
is more effective at aerating atelectatic
alveoli. Preoxygenation with NIPPV may
especially benefit patients with morbid
obesity, for whom diaphragmatic pressure
on lung units can contribute to alveolar
collapse.
For patients with high oxygen
requirements but minimal deficits
in ventilation, humidified high-flow
PHOTO COURTESY OF JAMES HEILMAN, MD – CC BY-SA 4.0
nasal cannulas are another option
for respiratory support.12 In a before-
mechanical ventilation. Any anesthetic CRITICAL DECISION and-after study of ICU patients who
agent used for rapid-sequence induction
How can postintubation underwent intubation, high-flow nasal
will decrease overall sympathetic
tone, which may cause rapid arterial
hypoxemia be limited? cannulas were associated with fewer
instances of severe hypoxemia than
vasodilation. Positive-pressure According to a retrospective
NRBs.13 A high-flow nasal cannula
ventilation also decreases venous return analysis of more than 3,000 patients
can also be kept in position during
and cardiac output, lowering blood who underwent emergent intubation,
laryngoscopy, allowing oxygenation to
pressure further. hypoxemia was a factor in 90% of cases
continue during apneic periods. This
Of all the anesthetics typically used of cardiac arrest immediately following
offers another advantage over traditional
for rapid-sequence induction, propofol the procedure.9 Apnea during rapid-
preoxygenation techniques.14
may be the most likely to worsen sequence induction places a patient at
hypotension, especially for patients high risk for hypoxemia, especially if CRITICAL DECISION
who are already in shock.7 As long the airway is anatomically challenging
When and how should
as there is no cardiogenic pulmonary and requires multiple attempts to
edema, using empiric fluid loading intubate. The traditional approach for patients with metabolic
and administering vasopressors early limiting hypoxemia during intubation is acidosis be intubated?
to patients with a high shock index preoxygenation. This process provides Acidosis, especially lactic acidosis, is
may also help mitigate postintubation the patient with a high FiO2 in an effort a marker of poor prognosis for patients
hypotension. to dilute the nitrogen content of gas in shock states and can complicate the
A recent survey asked physicians in the alveoli and provide a reservoir physiology of emergency intubation.15,16
how they would manage patients of oxygen-rich gas that can continue The body often compensates for severe
who need intubation for a variety of to participate in gas exchange during metabolic acidosis by maintaining a
reasons, including trauma, pneumonia, apneic periods. Preoxygenation has high minute ventilation, which manifests
and congestive heart failure.8 The historically been administered with a clinically as a high respiratory rate and
vast majority said they would provide nasal cannula or nonrebreather mask high work of breathing. In these cases,
intravenous crystalloid resuscitation (NRB); however, alternative approaches initial resuscitation attempts are focused
before intubating the patient. By contrast, using newer modes of preoxygenation on reversing early organ hypoperfusion
only 4.9% of providers surveyed may benefit the critically ill patient. and mitigating acidosis in order to
would routinely use vasopressors in Noninvasive positive pressure decrease the work of breathing; however,
these scenarios. In light of the data ventilation (NIPPV) is known to be useful this is not always successful within the
reviewed above, using vasopressors for a variety of disease processes, and a first few hours of a patient’s course, and
more consistently may be a way to make growing body of evidence suggests that the risk of cardiac arrest from acidemia
emergency intubations safer. it is also a safe and beneficial method for grows higher as the patient’s ventilatory
July 2021 n Volume 35 Number 7 5
flow is impaired more than inspiratory flow,
FIGURE 3. Recognizing Intrinsic PEEP and as a result, air from the previous breath
Flow Time may remain in the alveoli when a new
Inspiration
breath is inspired. With each respiratory
Normal
cycle, the volume of air trapped in the
Patient
alveoli grows, creating increasing pressure
in the lungs at the end of expiration.
This buildup of pressure is referred to
Flow (L/min)
Time (sec)
as intrinsic PEEP, auto-PEEP, or breath
stacking, and it can have several harmful
effects on the patient.19,20 The inability to
Trapping
intrinsic adequately ventilate can contribute to and
PEEP exacerbate respiratory acidosis. If intrinsic
Expiration PEEP continues to climb, it puts the patient
at risk of barotrauma and pneumothorax.
At the bedside, intrinsic PEEP can be
detected by looking at the flow-vs-time
abilities begin to wane. The savvy This principle has been demonstrated waveform displayed on the ventilator
emergency physician will recognize that in autopsy studies of rats following (Figure 3). If the expiratory flow rate
acidosis that persists despite adequate bicarbonate administration.17 does not return to zero (or the level
resuscitation is a reason to intubate. of applied PEEP set on the ventilator)
For patients with severe metabolic CRITICAL DECISION
before rising again with a new breath,
acidosis, the aim during intubation How should patients with this suggests some degree of air trapping
should be to minimize the amount of obstructive lung disease be that contributes to intrinsic PEEP. To
time ventilation is interrupted. Foregoing
intubated and monitored? quantify the degree of intrinsic PEEP, it is
neuromuscular blocking agents to
useful to perform an end-expiratory pause
avoid paralysis may allow the patient Patients with severe obstructive lung
maneuver on the ventilator and note the
to maintain some degree of respiratory disease lose their ability to ventilate as
airway pressure reading during the pause.
compensation during the procedure, a result of obstructed outflow through
This measurement minus any applied
but the added challenge of intubating small airways. Traditional therapies
PEEP represents intrinsic PEEP.
a nonparalyzed patient may outweigh include β2 agonists, anticholinergic agents,
If significant air-trapping and carbon
this benefit. To minimize apnea, an and corticosteroids, which are aimed
dioxide retention are detected, the best
experienced physician should be the at reversing bronchoconstriction and
way to improve ventilation may be to
one to attempt the intubation. After inflammation. When these therapies fail,
decrease the respiratory rate on the
intubation, the ventilator should be set to however, patients may need mechanical
ventilator. Lowering the respiratory rate
a respiratory rate that approximates the ventilation. In these cases, using ketamine
while keeping the inspiratory time fixed
patient’s preintubation respiratory rate in as an induction agent not only anesthetizes
provides more expiratory time in each
order to compensate for the acidosis. patients for intubation but also provides
breath cycle, allowing for the complete
The use of sodium bicarbonate to β agonism and bronchodilation that may
exhalation of each volume of air before
treat acidemia has been suggested in improve their ability to ventilate.18
the initiation of the next breath.
the past, but it is a practice that begs Following intubation, the physician
reassessment. Theoretically, bicarbonate must remain aware of positive end- Summary
treats acidemia when bicarbonate anions expiratory pressure (PEEP). When the Intubation and initial ventilator
bind with hydrogen ions and form small airways are obstructed, expiratory management in the emergency department
carbon dioxide and water. In order for
this strategy to effectively increase pH,
the patient must be able to adequately
ventilate and load this additional carbon
dioxide. As patients undergo induction
and reduced ventilation, this ability to
appropriately breathe off the excess n In hemodynamically stable patients, a shock index (heart rate ÷ systolic
carbon dioxide is compromised, limiting blood pressure) of >0.8 before intubation is an excellent predictor of
any theoretical improvement in pH postintubation hypotension.
from the bicarbonate. Furthermore, the n For patients with severe hypoxemia and morbid obesity, consider preoxygen
additional carbon dioxide can easily ating with noninvasive positive pressure ventilation before intubating.
n A high-flow nasal cannula is useful for preoxygenation and can remain in
cross cell membranes and decrease
place to provide oxygen during apneic periods of induction and intubation.
intracellular pH, causing cellular injury.
6 Critical Decisions in Emergency Medicine
CASE RESOLUTIONS
■ CASE ONE ■ CASE TWO ■ CASE THREE
Physicians decided to intubate this The woman’s high lactate, work Despite noninvasive ventilation and
patient when less-invasive techniques of breathing, and progressive fatigue other appropriate therapies for acute
failed to reverse his hypoxemic all pointed toward lactic acidosis and exacerbation of COPD, this patient’s
respiratory failure. Because hypoxemia impending respiratory failure. Her condition was deteriorating. Physicians
put him at high risk for further low blood pressure and shock index decided to intubate the patient and
desaturation during intubation, FiO2 of 1.3 indicated a high probability of opted to anesthetize him with ketamine
through noninvasive positive pressure postintubation hypotension, so she was for the best chance of improving his
ventilation was increased to 1.0 to started on norepinephrine 5 mcg/min ventilation before the procedure. The
maximize preoxygenation. The patient IV, which improved her blood pressure
patient’s ventilator was initially set to
was also placed on high-flow oxygen to 123/85. After rapid-sequence
a respiratory rate of 20 breaths/min
through a nasal cannula at 40 L/min induction, she was intubated quickly
with a tidal volume of 500 mL and an
and FiO2 of 1.0. These interventions by an attending physician, who focused
applied PEEP of 5 cm H 2O. After 30
raised the patient’s SpO2 to 98%. The on minimizing apnea time to avoid
minutes, the peak pressure and plateau
nasal cannula was left in place to take worsening the patient’s acidosis. The
pressure measured by the ventilator had
advantage of passive oxygenation ventilator was set to a respiratory
while the patient underwent rapid- rate of 30 breaths/min to maintain both increased markedly. By inspecting
sequence induction using etomidate appropriate compensation for the the flow-vs-time waveform on the
for anesthesia and rocuronium for acidosis. Intubation dropped the patient’s ventilator, physicians determined that
neuromuscular blocking. The patient’s blood pressure to 90/52, but after an the patient’s expiratory flow was being
SpO2 decreased to 93% as the tube hour of additional fluid resuscitation, interrupted each new breath, resulting in
was placed, but the intubation was she was weaned off vasopressors and a buildup of intrinsic PEEP. Decreasing
successful, and mechanical ventilation remained hemodynamically stable. A the ventilator respiratory rate to 12
slowly brought his oxygen level back postintubation blood gas showed a pH breaths/min improved both the intrinsic
to normal. of 7.37 and a PCO2 of 24. PEEP and the plateau pressure.
are often complicated by the fact that Med. 1994 Jul;12(4):425-428 arrest during emergency tracheal intubation: a
3. Lin CC, Chen KF, Shih CP, Seak CJ, Hsu KH. The justification for incorporating the ASA Guidelines in the
patients are already critically ill, placing prognostic factors of hypotension after rapid sequence remote location. J Clin Anesth. 2004 Nov;16(7):508-516.
intubation. Am J Emerg Med. 2008 Oct;26(8):845-851. 10. Nava S, Hill N. Non-invasive ventilation in acute
them at high risk for postintubation 4. Heffner AC, Swords DS, Neale MN, Jones AE. Incidence respiratory failure. Lancet. 2009 Jul 18;374(9685):250-259.
11. Baillard C, Fosse JP, Sebbane M, et al. Noninvasive
complications. While it is impossible and factors associated with cardiac arrest complicating
ventilation improves preoxygenation before intubation
emergency airway management. Resuscitation. 2013
to prevent these complications entirely, Nov;84(11):1500-1504. of hypoxic patients. Am J Respir Crit Care Med. 2006
5. Kim WY, Kwak MK, Ko BS, et al. Factors associated Jul 15;174(2):171-177
understanding the pathophysiology with the occurrence of cardiac arrest after emergency 12. Frat JP, Thille AW, Mercat A, et al. High-flow oxygen
through nasal cannula in acute hypoxemic respiratory
involved can inform basic interventions tracheal intubation in the emergency department. PLoS
One. 2014 Nov 17;9(11): e112779. failure. N Engl J Med. 2015 Jun 4;372(23):2185-2196.
13. Miguel-Montanes R, Hajage D, Messika J, et al. Use
that may limit harmful effects and improve 6. Heffner AC, Swords DS, Nussbaum ML, Kline JA, Jones
of high-flow nasal cannula oxygen therapy to prevent
AE. Predictors of the complication of postintubation
patient outcomes. hypotension during emergency airway management. J
desaturation during tracheal intubation of intensive
care patients with mild-to-moderate hypoxemia. Crit
Crit Care. 2012 Dec;27(6):587-593. Care Med. 2015 Mar;43(3):574-583.
7. Johnson KB, Egan TD, Kern SE, et al. The influence of
REFERENCES hemorrhagic shock on propofol: a pharmacokinetic and
14. Jaber S, Monnin M, Girard M, et al. Apnoeic
oxygenation via high-flow nasal cannula oxygen
1. Morris C, Perris A, Klein J, Mahoney P. Anaesthesia in pharmacodynamic analysis. Anesthesiology. 2003 Aug; combined with non-invasive ventilation preoxygenation
haemodynamically compromised emergency patients: 99(2):409-420. for intubation in hypoxaemic patients in the intensive
does ketamine represent the best choice of induction 8. Green RS, Fergusson DA, Turgeon AF, et al. care unit: the single-centre, blinded, randomized
agent? Anaesthesia. 2009 May;64(5):532-539. Resuscitation prior to emergency endotracheal controlled OPTINIV trial. Intensive Care Med. 2016
2. Franklin C, Samuel J, Hu TC. Life-threatening intubation: results of a national survey. West J Emerg Dec;42(12):1877-1887.
hypotension associated with emergency intubation and Med. 2016 Sep;17(5):542-548. 15. Blow O, Magliore L, Claridge JA, Butler K, Young JS.
the initiation of mechanical ventilation. Am J Emerg 9. Mort TC. The incidence and risk factors for cardiac The golden hour and the silver day: detection and
correction of occult hypoperfusion within 24 hours
improves outcome from major trauma. J Trauma. 1999
Nov;47(5):964-969.
16. Fuller BM, Dellinger RP. Lactate as a hemodynamic
marker in the critically ill. Curr Opin Crit Care. 2012
Jun;18(3):267-272
17. Shapiro JI, Whalen M, Kucera R, Kindig N, Filley G,
Chan L. Brain pH responses to sodium bicarbonate and
Carbicarb during systemic acidosis. Am J Physiol. 1989
May;256(5 Pt 2):H1316-H1321.
18. Jabre P, Combes X, Lapostolle F, et al. Etomidate versus
n Failing to recognize that any medication used for induction can decrease ketamine for rapid sequence intubation in acutely ill
patients: a multicentre randomised controlled trial.
sympathetic tone and thereby precipitate hypotension. Lancet. 2009 Jul 25;374(9686):293-300.
n Administering sodium bicarbonate in an attempt to treat acidemia before 19. Oddo M, Feihl F, Schaller MD, Perret C. Management of
mechanical ventilation in acute severe asthma: practical
intubation. aspects. Intensive Care Med. 2006 Apr; 32(4):501-510.
n Increasing, rather than decreasing, the respiratory rate on the ventilator for 20. Ward NS, Dushay KM. Clinical concise review:
mechanical ventilation of patients with chronic
patients who are demonstrating intrinsic PEEP and limited expiratory flow. obstructive pulmonary disease. Crit Care Med. 2008
May;36(5):1614-1619.
July 2021 n Volume 35 Number 7 7
You might also like
- HK MJ 208944Document3 pagesHK MJ 208944Bianca CaterinalisendraNo ratings yet
- Case Study, Chapter 20, Assessment of Respiratory FunctionDocument11 pagesCase Study, Chapter 20, Assessment of Respiratory FunctionMaddyNo ratings yet
- Management of Life Threatening Asthma. Severe Asthma Series. CHEST 2022Document10 pagesManagement of Life Threatening Asthma. Severe Asthma Series. CHEST 2022carla jazmin cortes rodriguezNo ratings yet
- Management of Life-Threatening Asthma (@ eDocument10 pagesManagement of Life-Threatening Asthma (@ eLex X PabloNo ratings yet
- Alta - Poster InasiaDocument1 pageAlta - Poster InasiaaltaikhsannurNo ratings yet
- Thoracic Epidural For Modified Radical Mastectomy in A High-Risk PatientDocument2 pagesThoracic Epidural For Modified Radical Mastectomy in A High-Risk PatientBianca CaterinalisendraNo ratings yet
- Critical Care Review: Airway Management of The Critically Ill PatientDocument16 pagesCritical Care Review: Airway Management of The Critically Ill PatientNikita ShakyaNo ratings yet
- RSI - Children 2 PDFDocument6 pagesRSI - Children 2 PDFAbdul RachmanNo ratings yet
- 1 s2.0 S0733862722000384 MainDocument13 pages1 s2.0 S0733862722000384 Maincoca12451No ratings yet
- Dr. AftabDocument87 pagesDr. Aftabalhada azofit almaNo ratings yet
- Anesthesia Considerations in Microlaryngoscopy or Direct LaryngosDocument6 pagesAnesthesia Considerations in Microlaryngoscopy or Direct LaryngosRubén Darío HerediaNo ratings yet
- Clinical Replacement Student Packet-3Document12 pagesClinical Replacement Student Packet-3ida100% (1)
- Diificult AirwayDocument13 pagesDiificult AirwayBhi-An BatobalonosNo ratings yet
- Anesthesia in Prehospital Emergencies and in The Emergency DepartmentDocument7 pagesAnesthesia in Prehospital Emergencies and in The Emergency DepartmentIvan TapiaNo ratings yet
- Secuencia Rapida GuiasDocument29 pagesSecuencia Rapida GuiasToñoGomezNo ratings yet
- AHA 2020 Resusitasi PediatrikDocument74 pagesAHA 2020 Resusitasi PediatrikmeritabasrilNo ratings yet
- Acute Life-Threatening Hypoxemia During Mechanical VentilationDocument8 pagesAcute Life-Threatening Hypoxemia During Mechanical VentilationCesar Rivas CamposNo ratings yet
- Accepted Manuscript: 10.1016/j.chest.2016.03.043Document22 pagesAccepted Manuscript: 10.1016/j.chest.2016.03.043Med Issam MahouachiNo ratings yet
- Delayed Sequence Intubation - 2016Document8 pagesDelayed Sequence Intubation - 2016Ivan HarizanovNo ratings yet
- Basic Life Suppor T: Monalyn B. La-Ao, RN Glenn Ryan Palao-Ay, RNDocument37 pagesBasic Life Suppor T: Monalyn B. La-Ao, RN Glenn Ryan Palao-Ay, RNMarlon Pilis B CanggatNo ratings yet
- Hospital Acquired PneumoniaDocument20 pagesHospital Acquired PneumoniaMradipta Arrya MNo ratings yet
- Chest Physical Therapy For Patients in Intensive Care Unit: Key WordsDocument17 pagesChest Physical Therapy For Patients in Intensive Care Unit: Key WordsNeil Francis VillagonzaloNo ratings yet
- Gadar 1Document7 pagesGadar 1Mega MemoryNo ratings yet
- Wa0006Document9 pagesWa0006Venkata Nagaraj MummadisettyNo ratings yet
- Clinical Investigations in Critical Care: Spinal Muscular Atrophy Type 1Document6 pagesClinical Investigations in Critical Care: Spinal Muscular Atrophy Type 1Aziz RosyidNo ratings yet
- Modified RapidseqDocument8 pagesModified RapidseqzaheermechNo ratings yet
- Nursing Management of A Patient With COVID-19 Receiving ECMO - A Case ReportDocument11 pagesNursing Management of A Patient With COVID-19 Receiving ECMO - A Case ReportMedicina Critica FcvNo ratings yet
- (Mayo Clinic Proceedings, Dec 2022) - 82 Year Old Man With Chest Pain and Shortness of BreathDocument5 pages(Mayo Clinic Proceedings, Dec 2022) - 82 Year Old Man With Chest Pain and Shortness of BreathNigelyulNo ratings yet
- Blunt Chest Trauma GuidelineDocument19 pagesBlunt Chest Trauma Guidelineana9filimonNo ratings yet
- Chest Physical Therapy For Patients in Intensive Care Unit: Key WordsDocument17 pagesChest Physical Therapy For Patients in Intensive Care Unit: Key Wordsketrin maladaNo ratings yet
- Rosen's MCQs 10th Edition (1) .Document304 pagesRosen's MCQs 10th Edition (1) .abdoesra82No ratings yet
- Alexanders Care of The Patient in Surgery 16th Edition Rothrock Test BankDocument11 pagesAlexanders Care of The Patient in Surgery 16th Edition Rothrock Test Banklilykeva56r100% (32)
- Alexanders Care of The Patient in Surgery 16th Edition Rothrock Test Bank Full Chapter PDFDocument32 pagesAlexanders Care of The Patient in Surgery 16th Edition Rothrock Test Bank Full Chapter PDFwilliamboydnatcwzpofb100% (12)
- Secuencia de Intubación RápidaDocument16 pagesSecuencia de Intubación Rápidaalis_maNo ratings yet
- Chapter 11Document5 pagesChapter 11DEENo ratings yet
- HP May00 Sedat PDFDocument9 pagesHP May00 Sedat PDFSaurabh SatheNo ratings yet
- Rehabilitacion Pulmonar en La UciDocument19 pagesRehabilitacion Pulmonar en La UcimavhelllinaNo ratings yet
- Evid TT 2200305Document4 pagesEvid TT 2200305Muthia Farah AshmaNo ratings yet
- Care Unit Chest Physical Therapy For Patients in The IntensiveDocument19 pagesCare Unit Chest Physical Therapy For Patients in The IntensivezaqiyahNo ratings yet
- Emergency Department Management of Acute Asthma ExacerbationsDocument32 pagesEmergency Department Management of Acute Asthma ExacerbationsFercho MedNo ratings yet
- Cervical Epidural For Total Thyroidectomy in A Patient With Large Thyroid Nodule With Retrosternal Extension With Superior Vena Caval Compression SyndromeDocument2 pagesCervical Epidural For Total Thyroidectomy in A Patient With Large Thyroid Nodule With Retrosternal Extension With Superior Vena Caval Compression SyndromeInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- ArdsDocument18 pagesArdsSana SanaNo ratings yet
- Extubacion en Pacientes Con Enfermedades NeuromuscularesDocument9 pagesExtubacion en Pacientes Con Enfermedades NeuromuscularesjuliasimonassiNo ratings yet
- Case Study Chapter 20 (Oct 16th)Document2 pagesCase Study Chapter 20 (Oct 16th)Anz MingNo ratings yet
- Cardiovascular CareDocument2 pagesCardiovascular CareGeof EnobNo ratings yet
- Driver 2016Document2 pagesDriver 2016clichegalNo ratings yet
- Critical Care - Improving OutcomesDocument81 pagesCritical Care - Improving OutcomeshimanshuNo ratings yet
- E Posters PDFDocument349 pagesE Posters PDFpriyadikkalaNo ratings yet
- Bell 2015Document5 pagesBell 2015Afien MuktiNo ratings yet
- 01 Clinical Anesthesiology OverviewDocument2 pages01 Clinical Anesthesiology OverviewJim Jose AntonyNo ratings yet
- 2020 TonicClonicSeizures Spinalanesthesia PDFDocument2 pages2020 TonicClonicSeizures Spinalanesthesia PDFGin RummyNo ratings yet
- Critical Care Nursing Diagnosis and Management UrdenDocument8 pagesCritical Care Nursing Diagnosis and Management UrdenMonet0% (1)
- Chest PT in Icu 1996@609.full PDFDocument17 pagesChest PT in Icu 1996@609.full PDFDyah SafitriNo ratings yet
- Non-Invasive Positive Pressure Ventilation in Acute Respiratory Failure: Providing Competent CareDocument9 pagesNon-Invasive Positive Pressure Ventilation in Acute Respiratory Failure: Providing Competent CareAndana TrisaviNo ratings yet
- Non-Invasive Ventilation in Acute Respiratory Failure: Bts GuidelineDocument21 pagesNon-Invasive Ventilation in Acute Respiratory Failure: Bts GuidelineddubbNo ratings yet
- Cardiac Arrest in Labour Leading To Perimortem Caesarean Section in A Woman With A Body Mass Index 46 With A Successful OutcomeDocument3 pagesCardiac Arrest in Labour Leading To Perimortem Caesarean Section in A Woman With A Body Mass Index 46 With A Successful OutcomeFhyah Vhie PhiepiNo ratings yet
- VSIM Nursing Clinical Rotation WorksheetDocument13 pagesVSIM Nursing Clinical Rotation WorksheetVin Lorenzo CampbellNo ratings yet
- Anaesthesia For Trauma PatientsDocument42 pagesAnaesthesia For Trauma PatientsMerindukan Surga MuNo ratings yet
- Du ProfessorsDocument28 pagesDu Professorsalka sharmaNo ratings yet
- USP Initiatives in Promoting The Quality of Medicines GloballyDocument33 pagesUSP Initiatives in Promoting The Quality of Medicines GloballyMiles MudzvitiNo ratings yet
- Arvophillia Candidate Instructions PDFDocument2 pagesArvophillia Candidate Instructions PDFRose Diop67% (3)
- Health Risk AssessmentDocument45 pagesHealth Risk AssessmentAboghassanNo ratings yet
- Garcia v. Salvador G.R. NO. 168512, March 20, 2007Document9 pagesGarcia v. Salvador G.R. NO. 168512, March 20, 2007ChatNo ratings yet
- Ultrasound Guided Versus Conventional Lung.6Document10 pagesUltrasound Guided Versus Conventional Lung.6Hyo Jun YangNo ratings yet
- Comparison of 3D C-Arm Fluoroscopy and 3D Image-GuidedDocument8 pagesComparison of 3D C-Arm Fluoroscopy and 3D Image-Guidedgevowo3277No ratings yet
- Count To Ten Allowing YourselfDocument1 pageCount To Ten Allowing YourselfwisgeorgekwokNo ratings yet
- 101 NotesDocument27 pages101 Notesgmcym8w9ppNo ratings yet
- Strategic Management - Phase 1 - ANAMARTINEZ - 212053 - 7Document13 pagesStrategic Management - Phase 1 - ANAMARTINEZ - 212053 - 7AnaNo ratings yet
- Process RecordingDocument8 pagesProcess RecordingjoanneNo ratings yet
- Josseicka Reynoso ResumeDocument1 pageJosseicka Reynoso ResumeLouis MarchiNo ratings yet
- ATEXDocument1 pageATEXmigelNo ratings yet
- DEvinDocument7 pagesDEvinTuriyo AnthonyNo ratings yet
- National Rehabilitation Strategic Plan (2020-2024) - English (REVISED)Document44 pagesNational Rehabilitation Strategic Plan (2020-2024) - English (REVISED)Sergio CurteanNo ratings yet
- Crab LouseDocument4 pagesCrab Louseenzo abrahamNo ratings yet
- Adoc - Pub - Arikunto S 2010 Prosedur Penelitian Rev Ed JakartaDocument5 pagesAdoc - Pub - Arikunto S 2010 Prosedur Penelitian Rev Ed JakartaResa Eni Santi WulandariNo ratings yet
- Vaporesso XROS 3 User Manual A1 20221102Document33 pagesVaporesso XROS 3 User Manual A1 20221102EnricoNo ratings yet
- Confusion Matrix: For Evaluating The KNN ModelDocument17 pagesConfusion Matrix: For Evaluating The KNN ModelSUHRIT BISWASNo ratings yet
- Falcon Maritime and Allied Services Vs Angelito Pangasian - 3HPajaritoDocument2 pagesFalcon Maritime and Allied Services Vs Angelito Pangasian - 3HPajaritoHenio PajaritoNo ratings yet
- Nursing Philosohy ApaDocument4 pagesNursing Philosohy Apaapi-520823631No ratings yet
- Perfection: Setting StandardsDocument2 pagesPerfection: Setting StandardsGustavo MataNo ratings yet
- Travel Hassle-Free With..Document3 pagesTravel Hassle-Free With..Muthuraman Lakshmanan100% (1)
- RCVS Exam GuidanceDocument37 pagesRCVS Exam GuidanceRenan RodriguesNo ratings yet
- Online Rules and Regulations: QR-ACA-CAE04-002Document51 pagesOnline Rules and Regulations: QR-ACA-CAE04-002Loren Marie Lemana AceboNo ratings yet
- Socioeconomic Status ScaleDocument27 pagesSocioeconomic Status ScaleBandi KotreshNo ratings yet
- Perspective: New England Journal MedicineDocument3 pagesPerspective: New England Journal MedicinePatrick CommettantNo ratings yet
- CA HDKN Wacker YA47895 & YA47897 PDFDocument4 pagesCA HDKN Wacker YA47895 & YA47897 PDFSatak ArHundaNo ratings yet
- CPR ReportingDocument39 pagesCPR ReportingNheler SonNo ratings yet
- Nme 427 1meDocument33 pagesNme 427 1meAriel Gamboa100% (1)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)From EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Rating: 3 out of 5 stars3/5 (1)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (4)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (404)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 4 out of 5 stars4/5 (4)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 4.5 out of 5 stars4.5/5 (82)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (34)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (46)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (6)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeRating: 2 out of 5 stars2/5 (1)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (170)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeFrom EverandThe Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeRating: 4.5 out of 5 stars4.5/5 (2)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesFrom EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesRating: 4.5 out of 5 stars4.5/5 (1412)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (44)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisFrom EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisRating: 5 out of 5 stars5/5 (8)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- How to ADHD: The Ultimate Guide and Strategies for Productivity and Well-BeingFrom EverandHow to ADHD: The Ultimate Guide and Strategies for Productivity and Well-BeingRating: 1 out of 5 stars1/5 (2)
- To Explain the World: The Discovery of Modern ScienceFrom EverandTo Explain the World: The Discovery of Modern ScienceRating: 3.5 out of 5 stars3.5/5 (51)
- Self-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!From EverandSelf-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!Rating: 5 out of 5 stars5/5 (1)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsFrom EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsRating: 4.5 out of 5 stars4.5/5 (39)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (254)