Volume 8, Issue 1, January – 2023 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
The Effect of Intravenously Administered
Dexmedetomidine on Haemodynamic Response to
Intubation in Patients Undergoing Surgery Under
General Anaesthesia
Dr.K.Yashaswi Srivasthava Dr. Y. V. Somashekar
Anesthesiology Anesthesiology
Kurnool Medical College Kurnool Medical College
Kurnool, India Kurnool, India
Abstract I. INTRODUCTION
Back ground: This study took for comparing efficacy of
IV Dexmedetomidine 0.5µg/kg and IV Dexmedetomidine Laryngoscopy and endotracheal intubation is often
1µg /kg in obtunding the hemodynamic response to associated with hypertension and tachycardia because of
laryngoscopy and endotracheal intubation when sympatho-adrenal stimulation which is usually transient
administered 10 minutes before induction. and lasts for about 5-10 minutes.
In patients with cardiovascular and cerebrovascular
Methodology: A Ninety patients scheduled for various diseases, the sudden hemodynamic response can produce
elective and emergency surgical procedures under deleterious effects in the form of myocardial ischaemia or
general anesthesia belonging to ASA class I & II and infarction, arrhythmias, cardiac failure, raised ICP and
Mallampati grade I & II in the age group of 18 years to cerebral haemorrhage.
60 years were included in the study. In view of this, the present study was undertaken to
compare the efficacy of IV Dexmedetomidine 0.5µg/kg
The study population was randomly divided into three and IV Dexmedetomidine 1µg /kg in obtunding the
groups group A received normal saline and represent as hemodynamic response to laryngoscopy and endotracheal
control , group B received IV Dexmedetomidine in a dose intubation when administered 10 minutes before
of 0.5µg/kg, group C received IV Dexmedetomidine in a induction.
dose of 1µg/kg
II. AIMS AND OBJECTIVES
The HR, SBP, DBP and MAP were recorded at the
following intervals, namely, basal reading before giving Aim of the study is to evaluate and compare the efficacy
the study drug, at 5 minute intervals from the end of drug of IV Dexmedetomidine 0.5μg/kg and IV Dexmedetomidine
infusion until induction, post induction/ pre- 1μg /kg in attenuating the adverse hemodynamic responses to
laryngoscopy and at 1, 2.5, 5, 10, 15 and 20 minutes laryngoscopy and endotracheal intubation when infused over
following tracheal intubation. 10 minutes, 10 minutes before induction.
Results : Analysis of the post induction and post III. MATERIALS AND METHODS
intubation values of mean HR and MAP variation from
the baseline values in the Group B and C depicts a This is a prospective double blinded study .
statistically significant difference (p < 0.001). Between A Ninety patients scheduled for various elective and
the two groups with the Group C demonstrated a greater emergency surgical procedures under general anesthesia
suppression of HR and MAP to intubation. There was no belonging to ASA class I & II and Mallampati grade I &
clinically significant difference between the two doses of II in the age group of 18 yrs to 60 yrs were included in the
the study drug in their efficacy. study.
The study population was randomly divided into three
Conclusion : Dexmedetomidine in a dose of 0.5μg/kg, groups Group A – (n=30) – received IV Normal saline
significantly attenuates the hemodynamic response to 20ml administered over 10 minutes, 10 minutes before
laryngoscopy and intubation for 10 minutes (p<0.001) induction of anesthesia.
with minimal adverse effects. Group B– (n=30) – received IV Dexmedetomidine in a
dose of 0.5µg/kg diluted in 20ml of normal saline infused
Keywords:- Dexmedetomidine, Hemodynamic Response. over 10 minutes, administered 10 minutes before
induction of anesthesia.
IJISRT23JAN311 www.ijisrt.com 260
Volume 8, Issue 1, January – 2023 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
Group C- (n=30)-received IV Dexmedetomidine in a dose
of 1µg/kg diluted in 20ml of normal saline infused over
10 minutes, administered 10 minutes before induction of
anesthesia.
All patients were premedicated with Inj Ondansetron
0.08mg/kg IV and Inj Fentanyl 2µg/kg IV prior to
induction. Anesthesia was induced after the
administration of the study drug using Inj Propofol IV
titrated to the loss of verbal response.
This was followed by Inj Atracurium 0.5mg/kg IV.
Laryngoscopy and endotracheal intubation was done after
3 minutes.
The HR, SBP, DBP and MAP were recorded at the
following intervals, namely, basal reading before giving
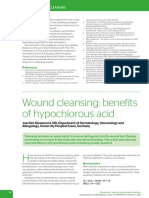
the study drug, at 5 minute intervals from the end of drug Fig 1: comparison of heart rates between study groups
infusion until induction, post induction/ pre-laryngoscopy
and at 1, 2.5, 5, 10, 15 and 20 minutes following tracheal In group A(control ) the mean HR was 84.60±12.73,
intubation. which didn't change with administration of control drug.
Post induction of anesthesia HR was 84.60±12.73. Post
Statistical Analysis Intubation there was a rise in the mean heart rate values
Descriptive and inferential statistical analysis has been from the base line value by 17.5b/min at 1 minute,
carried out . Results on continuous measurements are 12.63b/min at 2.5 minutes, 0.47b/min at 5 minutes,
presented on Mean SD (Min-Max) and results on categorical 2.47b/min at 10 minutes, finally returning close to pre-
measurements are presented in Number (%). Significance is laryngoscopic values at 10 minutes.The maximum rise of
assessed at 5 % level of significance. heart rate was at 1 minute.
In group B(Dexmedetomidine 0.5µg) the mean base line
Analysis of variance (ANOVA) has been used to find HR was 85.33±13.34 which decreased by 22.26 following
the significance of study parameters between three or more induction. Post Intubation there was a mean decrease in
groups of patients , Post-hoc Tukey test has been used to find the HR values from the base line values by 25.98b/min at
the pair wise significance. 1minute, 24.96b/min at 2.5minutes, 29.63b/min at
5minutes, 29.66b/min at 10minutes, 29.82b/min at
Statistical soft ware namely SAS9.2,SPSS15.0 were 15minutes
used for analysis of data. In group C(Dexmedetomidine 1µg) the mean base line
HR was 81.13±11.97 which decreased by 18.17 following
IV. RESULTS induction. Post Intubation there was a mean decrease in
the HR values from the base line values by 17.03 at
Table 1 : comparison of heart rates between study groups 1minute, 27.9b/min at 2.5minutes, 26.3b/min at 5minutes
25.93b/min at 10minutes, 25.56b/min at 15minutes.
Both study groups(B & C) were comparable with respect
to there HR at base line, 1 minute, 2.5 minutes, 5 and 10
minutes after administration of the study drug. There was
a statistically significant difference between the two study
groups when compared to the control group with regard
to their HR values(p values being <0.01). Group
C(Dexmedetomidine 1µg) demonstrated a greater
suppression of chronotropic response to intubation as
compared to other groups.
Comparison between the two groups demonstrated that
there was no statistically significant difference between
the mean HR values of the two groups upto 15 minutes
after the administration of the study drug.
Thus it may be said that there was no clinically
significant difference between the two study drugs in their
efficacy to attenuate the chronotropic response to
intubation. But when compared to control group there was
a significant difference and clinically signifiacant
suppression of HR.
IJISRT23JAN311 www.ijisrt.com 261
Volume 8, Issue 1, January – 2023 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
In group B 4 patients required treatment for bradycardia, mean MAP rise above the base line mean MAP value of
where as in group C, 11 patients required treatment for the study population in this group. The maximum fall of
bradycardia. MAP was at 1minute post induction.
In Group C, the mean base line MAP was 78.00±11.4
Table 2 : comparison of mean arterial pressure among study which decreased by 15.42mmHg after induction of
groups anesthesia. Post intubation there was a decrease in mean
MAP values from base line values 11.24mmHg at
1minute, 16.42mmHg at 2.5minutes, decreased by
19.76mmHg at 5minutes, 18.22mmHg at 10minutes,
18.71mmHg at 15minutes.
The mean MAP values persistently remained low
throughout observation. At no point of time during the
post induction period did the mean MAP rise above the
base line mean MAP value of the study population in this
group. The maximum fall of MAP was at 5minutes post
intubation.
Comparison between the two groups demonstrated that
there was no statistically significant difference between
the mean MAP values of the two groups upto 10 minutes
after the administration of the study drug.
Thus it may be said that there was no clinically significant
difference between the two study drugs in their efficacy
to attenuate the pressor response to tracheal intubation
.But when compared to control group there was a
significant difference clinically and statistically.
In group II 4 patients required treatment for hypotension,
where has in group III, 11 patients required treatment for
hypotension
CONCLUSION
Analysis of the post induction and post intubation values
of mean HR and MAP variation from the baseline values
in the Group B and C depicts a statistically significant
difference (p < 0.001). Between the two groups with the
Group C demonstrated a greater suppression of HR and
MAP to intubation. There was no clinically significant
Fig 2 : comparison of mean arterial pressure among study
difference between the two doses of the study drug in their
groups
efficacy.
Dexmedetomidine in a dose of 0.5μg/kg, significantly
In Group A control, the mean base line MAP was
attenuates the hemodynamic response to laryngoscopy
78.38±11.59 which decreased by 4.91mmHg after
and intubation for 10 minutes (p<0.001) with minimal
induction of anesthesia. Post intubation there was a rise in
adverse effects.
mean MAP values from the base line values 11.62mmHg
at 1minute, 1.44mmHg at 2.5minutes, decreased by
REFERENCES
10.85mmHg at 5minutes, finally returning close to
prelaryngoscopic values at 10minutes. The maximum rise
[1]. Miller RD, Eriksson LI, Fleisher LA, Wiener-Kronish
in MAP was at 1minute.
JP, Young WL. Miller’s Anesthesia. Philadelphia,
Churchill Livingstone, 7th edition; 1585-1600
In Group B, the mean base line MAP was 76.04±11.88
[2]. Stoelting RK et al. Circulatory changes during direct
which decreased by 17mmHg after induction of
laryngoscopy and tracheal intubation: Influence of
anesthesia. Post intubation there was a decrease in mean
duration of laryngoscopy with or without prior
MAP values from the base line values 20.26mmHg at
lidocaine. Anaesthesiology, 1977; 47: 381 – 84.
1minute, 19.08mmHg at 2.5minutes, decreased by
[3]. Sagiroglu EA, Celik M, Orhon Z, Yuzer S, Sen B.
19.8mmHg at 5minutes, 16.28mmHg at 10minutes,
Different Doses of Dexmedetomidine on Controlling
13.57mmHg at 15minutes. The mean MAP values
Haemodynamic responses to tracheal Intubation.
persistently remained low throughout observation. At no
Internet Journal of Anesthesiology, 2010; 27(2)
point of time during the post induction period did the
IJISRT23JAN311 www.ijisrt.com 262
You might also like
- Pregnancy and Birth Source BookDocument666 pagesPregnancy and Birth Source BookRaluca Horhat100% (3)
- DIVA-5 Diva 5 Id English FormDocument20 pagesDIVA-5 Diva 5 Id English FormEspíritu Ciudadano92% (26)
- Trusted Medical Answers-In Seconds.: Helminth InfectionsDocument33 pagesTrusted Medical Answers-In Seconds.: Helminth InfectionsntnquynhproNo ratings yet
- Priscillas Medicine PDFDocument442 pagesPriscillas Medicine PDFZul Hisyam Fikri100% (1)
- Nagpur Gynecologist ListDocument46 pagesNagpur Gynecologist ListsreevidyaNo ratings yet
- Does Intravenous Low Dose Dexmedetomidine Supplementation Has Beneficial Effects On Spinal Anaesthesia?Document4 pagesDoes Intravenous Low Dose Dexmedetomidine Supplementation Has Beneficial Effects On Spinal Anaesthesia?MOHAMMED IQBALNo ratings yet
- 2 Article JCDR FinalDocument4 pages2 Article JCDR FinalMythology KingdomNo ratings yet
- Intravenous Dexmedetomidine Prolongs Bupivacaine Spinal Analgesia M Ma - M, I ZB, H Ma - A, B Aa - B, I MM S M. A - GDocument8 pagesIntravenous Dexmedetomidine Prolongs Bupivacaine Spinal Analgesia M Ma - M, I ZB, H Ma - A, B Aa - B, I MM S M. A - GMOHAMMED IQBALNo ratings yet
- AnthropometryDocument6 pagesAnthropometryMinaz PatelNo ratings yet
- 1 s2.0 S0104001421002037 MainDocument7 pages1 s2.0 S0104001421002037 MainFarhana MardilaNo ratings yet
- Comparison Efectiveness of Dexmedetomidine Versus Dexmedetomidine With Ketamine For Tympanoplasty Surgery Done Under Monitoredanaesthesia CareDocument7 pagesComparison Efectiveness of Dexmedetomidine Versus Dexmedetomidine With Ketamine For Tympanoplasty Surgery Done Under Monitoredanaesthesia CareIJAR JOURNALNo ratings yet
- KetamineDocument7 pagesKetamineAshiyan IrfanNo ratings yet
- A Double Blind, Randomised, Controlled Trial To Study The Effect of Dexmeditomidine On Hemodynamic and Recovery Responses During Tracheal ExtubationDocument1 pageA Double Blind, Randomised, Controlled Trial To Study The Effect of Dexmeditomidine On Hemodynamic and Recovery Responses During Tracheal ExtubationramukolakiNo ratings yet
- Ketamina y Dexmedetomidina en QuemadosDocument6 pagesKetamina y Dexmedetomidina en QuemadosVicky CascorNo ratings yet
- The Effects of Dexmedetomidine Added To Spinal Bupivacaine For Lower Limb SurgeryDocument4 pagesThe Effects of Dexmedetomidine Added To Spinal Bupivacaine For Lower Limb SurgeryInternational Organization of Scientific Research (IOSR)No ratings yet
- AN4 OA Sidharth-2Document6 pagesAN4 OA Sidharth-2Dede TarunaNo ratings yet
- Journal Homepage: - : IntroductionDocument8 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- Buharan MDDocument7 pagesBuharan MDNeha MasarkarNo ratings yet
- Effectiveness of Bolus Administration of Continuous Intravenous Lidocaine On Pain Intensity After Mastectomy SurgeryDocument6 pagesEffectiveness of Bolus Administration of Continuous Intravenous Lidocaine On Pain Intensity After Mastectomy SurgeryInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Effect of Intraoperative Dexmedetomidine On Post-Craniotomy PainDocument9 pagesEffect of Intraoperative Dexmedetomidine On Post-Craniotomy PainIva SantikaNo ratings yet
- JAMP - Mohamed Ali Edit.Document6 pagesJAMP - Mohamed Ali Edit.Iniya RajendranNo ratings yet
- IJPCR, Vol 15, Issue 9, Article 245Document5 pagesIJPCR, Vol 15, Issue 9, Article 245Jaldeep PatelNo ratings yet
- Cag La Oz Bak Isak Kurt 2009Document7 pagesCag La Oz Bak Isak Kurt 2009Arturo AlcantaraNo ratings yet
- Diamorfina SpinalDocument5 pagesDiamorfina SpinalAurora TrifaNo ratings yet
- Intravenous Lidocaine As A Suppressant of Coughing During Tracheal Intubation - Yukioka Et AlDocument4 pagesIntravenous Lidocaine As A Suppressant of Coughing During Tracheal Intubation - Yukioka Et AlnejdNo ratings yet
- DR Sourab Bokil ThesisDocument8 pagesDR Sourab Bokil ThesisPurushotham N PuruNo ratings yet
- MAC DexmethomidineDocument5 pagesMAC DexmethomidinedhitabwNo ratings yet
- Kim 2014Document5 pagesKim 2014Santosa TandiNo ratings yet
- IndianJAnaesth582138-632895 173449Document5 pagesIndianJAnaesth582138-632895 173449xxxvrgntNo ratings yet
- Anjali Bhure, Neelakshi Kalita, Prasad Ingley, C.P. Gadkari: Research ArticleDocument5 pagesAnjali Bhure, Neelakshi Kalita, Prasad Ingley, C.P. Gadkari: Research ArticleTedja PrakosoNo ratings yet
- Effects of Intravenous Dexmedetomidine On Hyperbaric Bupivacaine Spinal Anesthesia: A Randomized StudyDocument8 pagesEffects of Intravenous Dexmedetomidine On Hyperbaric Bupivacaine Spinal Anesthesia: A Randomized StudyMOHAMMED IQBALNo ratings yet
- Effect of Supplementation of Low Dose Intravenous Dexmedetomidine On Characteristics of Spinal Anaesthesia With Hyperbaric BupivacaineDocument5 pagesEffect of Supplementation of Low Dose Intravenous Dexmedetomidine On Characteristics of Spinal Anaesthesia With Hyperbaric BupivacaineMOHAMMED IQBALNo ratings yet
- Comparative Study of A Low-Dose With Standard Dose Propofol in Electroconvulsive Therapy (ECT) in Federal Neuropsychiatric Hospital, KadunaDocument5 pagesComparative Study of A Low-Dose With Standard Dose Propofol in Electroconvulsive Therapy (ECT) in Federal Neuropsychiatric Hospital, KadunaAdeyemi OlusolaNo ratings yet
- EtamolDocument5 pagesEtamolthonyyanmuNo ratings yet
- Annals of International Medical and Dental ResearchDocument4 pagesAnnals of International Medical and Dental ResearchDr Rohit varshneyNo ratings yet
- 5 Dexmedetomidine As Rescue Drug During Awake Craniotomy For Cortical Motor Mapping and Tumor Resection - Case Report - Anesth Analg 2006 1021556-8Document3 pages5 Dexmedetomidine As Rescue Drug During Awake Craniotomy For Cortical Motor Mapping and Tumor Resection - Case Report - Anesth Analg 2006 1021556-8Meenal Chauhan MendirattaNo ratings yet
- Yurnal 1Document5 pagesYurnal 1Nopriza AidyNo ratings yet
- Dr. - Nataraj - EJCM 132 1888 1893 2023Document7 pagesDr. - Nataraj - EJCM 132 1888 1893 2023vithz kNo ratings yet
- 3959-Article Text-28779-2-10-20210715Document6 pages3959-Article Text-28779-2-10-20210715Mehroze SalmanNo ratings yet
- Intravenous Dexmedetomidine and Butorphanol Prolongs Bupivacaine Sensory Analgesia in Lower Abdominal Surgeries.Document5 pagesIntravenous Dexmedetomidine and Butorphanol Prolongs Bupivacaine Sensory Analgesia in Lower Abdominal Surgeries.International Organization of Scientific Research (IOSR)No ratings yet
- Yang Et Al-2019-Pediatric AnesthesiaDocument7 pagesYang Et Al-2019-Pediatric Anesthesiaabhaytyagi4130No ratings yet
- Journal Homepage: - : Manuscript HistoryDocument7 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- Efficacy of Postoperative Analgesia of Local Ketamine Wound Instillation Following Total ThyroidectomyDocument20 pagesEfficacy of Postoperative Analgesia of Local Ketamine Wound Instillation Following Total ThyroidectomyCristina RamirezNo ratings yet
- Comparison of Hyperbaric Levobupivacaine/ Bupivacaine For Ceserean SectionDocument6 pagesComparison of Hyperbaric Levobupivacaine/ Bupivacaine For Ceserean SectionIJAR JOURNALNo ratings yet
- Pediatric Premedication: A Double-Blind Randomized Trial of Dexmedetomidine or Ketamine Alone Versus A Combination of Dexmedetomidine and KetamineDocument7 pagesPediatric Premedication: A Double-Blind Randomized Trial of Dexmedetomidine or Ketamine Alone Versus A Combination of Dexmedetomidine and KetamineFatty MaulidiraNo ratings yet
- Artikel B.ind B.ing - Id.enDocument8 pagesArtikel B.ind B.ing - Id.enwikaNo ratings yet
- Negi 2014Document14 pagesNegi 2014Olivia LimNo ratings yet
- Dexme IntratechalDocument5 pagesDexme IntratechalDianWindiAmaliaNo ratings yet
- Early Postoperative ComplicationsDocument6 pagesEarly Postoperative Complications49hr84j7spNo ratings yet
- Effect of Optimizing The Induction Regimen in Preventing Cough - 2024 - ClinicalDocument6 pagesEffect of Optimizing The Induction Regimen in Preventing Cough - 2024 - ClinicalLuis GómezNo ratings yet
- Anafilaxia MidazolamDocument3 pagesAnafilaxia MidazolamDiana PintorNo ratings yet
- Anesth Analg 2019 129 6 1504-11Document8 pagesAnesth Analg 2019 129 6 1504-11Fernando SousaNo ratings yet
- Pub 3Document5 pagesPub 3Shreyas KateNo ratings yet
- Ó Canadian Anesthesiologists' Society 2009Document7 pagesÓ Canadian Anesthesiologists' Society 2009MOHAMMED IQBALNo ratings yet
- ClonidineDocument4 pagesClonidineDR RAVI ANANDNo ratings yet
- Clonidin As SedativeDocument7 pagesClonidin As SedativeHajar Rafika RaniNo ratings yet
- Meperidin: Toxicity SummaryDocument11 pagesMeperidin: Toxicity SummaryrosaNo ratings yet
- 2264-Article Text-5024-4-10-20151024Document6 pages2264-Article Text-5024-4-10-20151024shivamNo ratings yet
- Comparison of The Patient's Postoperative Sore Throat With General Anesthesia On The Use of Lidocaine Nebulizer and Ketamine Nebulizer in Haji Adam Malik Hospital MedanDocument7 pagesComparison of The Patient's Postoperative Sore Throat With General Anesthesia On The Use of Lidocaine Nebulizer and Ketamine Nebulizer in Haji Adam Malik Hospital MedanAnonymous izrFWiQNo ratings yet
- MRN000410 BnCWy5eDocument11 pagesMRN000410 BnCWy5eAn JNo ratings yet
- Effect of Intravenous Dexamethasone On The Regression of Isobaric Bupivacaine Spinal Anesthesia: A Randomized Controlled TrialDocument4 pagesEffect of Intravenous Dexamethasone On The Regression of Isobaric Bupivacaine Spinal Anesthesia: A Randomized Controlled TrialAndhi Riawan Eko WiikramatunggadewaNo ratings yet
- A Comparison of The Analgesic Effi Cacy of Transforaminal Methylprednisolone Alone and With Low Doses of Clonidine in Lumbo-Sacral RadiculopathyDocument9 pagesA Comparison of The Analgesic Effi Cacy of Transforaminal Methylprednisolone Alone and With Low Doses of Clonidine in Lumbo-Sacral RadiculopathyJumatun Mona WarahNo ratings yet
- A Double Blind, Randomised, Controlled Trial To Study The Effect of Dexmeditomidine On Hemodynamic and Recovery Responses During Tracheal ExtubationDocument8 pagesA Double Blind, Randomised, Controlled Trial To Study The Effect of Dexmeditomidine On Hemodynamic and Recovery Responses During Tracheal ExtubationramukolakiNo ratings yet
- Journal Homepage: - : Manuscript HistoryDocument10 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- Cyber Security Awareness and Educational Outcomes of Grade 4 LearnersDocument33 pagesCyber Security Awareness and Educational Outcomes of Grade 4 LearnersInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Factors Influencing The Use of Improved Maize Seed and Participation in The Seed Demonstration Program by Smallholder Farmers in Kwali Area Council Abuja, NigeriaDocument6 pagesFactors Influencing The Use of Improved Maize Seed and Participation in The Seed Demonstration Program by Smallholder Farmers in Kwali Area Council Abuja, NigeriaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Parastomal Hernia: A Case Report, Repaired by Modified Laparascopic Sugarbaker TechniqueDocument2 pagesParastomal Hernia: A Case Report, Repaired by Modified Laparascopic Sugarbaker TechniqueInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Smart Health Care SystemDocument8 pagesSmart Health Care SystemInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Blockchain Based Decentralized ApplicationDocument7 pagesBlockchain Based Decentralized ApplicationInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Unmasking Phishing Threats Through Cutting-Edge Machine LearningDocument8 pagesUnmasking Phishing Threats Through Cutting-Edge Machine LearningInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Study Assessing Viability of Installing 20kw Solar Power For The Electrical & Electronic Engineering Department Rufus Giwa Polytechnic OwoDocument6 pagesStudy Assessing Viability of Installing 20kw Solar Power For The Electrical & Electronic Engineering Department Rufus Giwa Polytechnic OwoInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- An Industry That Capitalizes Off of Women's Insecurities?Document8 pagesAn Industry That Capitalizes Off of Women's Insecurities?International Journal of Innovative Science and Research TechnologyNo ratings yet
- Visual Water: An Integration of App and Web To Understand Chemical ElementsDocument5 pagesVisual Water: An Integration of App and Web To Understand Chemical ElementsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Insights Into Nipah Virus: A Review of Epidemiology, Pathogenesis, and Therapeutic AdvancesDocument8 pagesInsights Into Nipah Virus: A Review of Epidemiology, Pathogenesis, and Therapeutic AdvancesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Smart Cities: Boosting Economic Growth Through Innovation and EfficiencyDocument19 pagesSmart Cities: Boosting Economic Growth Through Innovation and EfficiencyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Parkinson's Detection Using Voice Features and Spiral DrawingsDocument5 pagesParkinson's Detection Using Voice Features and Spiral DrawingsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Impact of Silver Nanoparticles Infused in Blood in A Stenosed Artery Under The Effect of Magnetic Field Imp. of Silver Nano. Inf. in Blood in A Sten. Art. Under The Eff. of Mag. FieldDocument6 pagesImpact of Silver Nanoparticles Infused in Blood in A Stenosed Artery Under The Effect of Magnetic Field Imp. of Silver Nano. Inf. in Blood in A Sten. Art. Under The Eff. of Mag. FieldInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Compact and Wearable Ventilator System For Enhanced Patient CareDocument4 pagesCompact and Wearable Ventilator System For Enhanced Patient CareInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Air Quality Index Prediction Using Bi-LSTMDocument8 pagesAir Quality Index Prediction Using Bi-LSTMInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Predict The Heart Attack Possibilities Using Machine LearningDocument2 pagesPredict The Heart Attack Possibilities Using Machine LearningInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Investigating Factors Influencing Employee Absenteeism: A Case Study of Secondary Schools in MuscatDocument16 pagesInvestigating Factors Influencing Employee Absenteeism: A Case Study of Secondary Schools in MuscatInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Relationship Between Teacher Reflective Practice and Students Engagement in The Public Elementary SchoolDocument31 pagesThe Relationship Between Teacher Reflective Practice and Students Engagement in The Public Elementary SchoolInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Diabetic Retinopathy Stage Detection Using CNN and Inception V3Document9 pagesDiabetic Retinopathy Stage Detection Using CNN and Inception V3International Journal of Innovative Science and Research TechnologyNo ratings yet
- An Analysis On Mental Health Issues Among IndividualsDocument6 pagesAn Analysis On Mental Health Issues Among IndividualsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Implications of Adnexal Invasions in Primary Extramammary Paget's Disease: A Systematic ReviewDocument6 pagesImplications of Adnexal Invasions in Primary Extramammary Paget's Disease: A Systematic ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Harnessing Open Innovation For Translating Global Languages Into Indian LanuagesDocument7 pagesHarnessing Open Innovation For Translating Global Languages Into Indian LanuagesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Keywords:-Ibadhy Chooranam, Cataract, Kann Kasam,: Siddha Medicine, Kann NoigalDocument7 pagesKeywords:-Ibadhy Chooranam, Cataract, Kann Kasam,: Siddha Medicine, Kann NoigalInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Utilization of Date Palm (Phoenix Dactylifera) Leaf Fiber As A Main Component in Making An Improvised Water FilterDocument11 pagesThe Utilization of Date Palm (Phoenix Dactylifera) Leaf Fiber As A Main Component in Making An Improvised Water FilterInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Impact of Digital Marketing Dimensions On Customer SatisfactionDocument6 pagesThe Impact of Digital Marketing Dimensions On Customer SatisfactionInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Dense Wavelength Division Multiplexing (DWDM) in IT Networks: A Leap Beyond Synchronous Digital Hierarchy (SDH)Document2 pagesDense Wavelength Division Multiplexing (DWDM) in IT Networks: A Leap Beyond Synchronous Digital Hierarchy (SDH)International Journal of Innovative Science and Research TechnologyNo ratings yet
- Advancing Healthcare Predictions: Harnessing Machine Learning For Accurate Health Index PrognosisDocument8 pagesAdvancing Healthcare Predictions: Harnessing Machine Learning For Accurate Health Index PrognosisInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Making of Object Recognition Eyeglasses For The Visually Impaired Using Image AIDocument6 pagesThe Making of Object Recognition Eyeglasses For The Visually Impaired Using Image AIInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Formulation and Evaluation of Poly Herbal Body ScrubDocument6 pagesFormulation and Evaluation of Poly Herbal Body ScrubInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Terracing As An Old-Style Scheme of Soil Water Preservation in Djingliya-Mandara Mountains - CameroonDocument14 pagesTerracing As An Old-Style Scheme of Soil Water Preservation in Djingliya-Mandara Mountains - CameroonInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Haemoglobin Levels in Patients With Oral Submucous FibrosisDocument5 pagesHaemoglobin Levels in Patients With Oral Submucous FibrosisDr Monal YuwanatiNo ratings yet
- Blood Gas AnalysisDocument28 pagesBlood Gas AnalysiskempolonNo ratings yet
- Microbial Diseases of The Nervous SystemDocument7 pagesMicrobial Diseases of The Nervous SystemAnaNo ratings yet
- Outline For History TakingDocument2 pagesOutline For History TakingBlancheNo ratings yet
- Hema I Chapter 12 - ESRDocument30 pagesHema I Chapter 12 - ESRTesfaNo ratings yet
- Obstetrics and GynaecologyDocument7 pagesObstetrics and GynaecologyRashed ShatnawiNo ratings yet
- Basic Emergency Life Support Depart Anesthesiology and Reanimation Dr. Soetomo Hospital - Airlangga UniversityDocument26 pagesBasic Emergency Life Support Depart Anesthesiology and Reanimation Dr. Soetomo Hospital - Airlangga Universityabee80No ratings yet
- Resume Anna BalancioDocument3 pagesResume Anna Balanciojihn isis tengcoNo ratings yet
- TABLE 77-1: Differential Diagnosis and Management of Dermal MelanocytosisDocument29 pagesTABLE 77-1: Differential Diagnosis and Management of Dermal MelanocytosisHellenPertiwiWulandariNo ratings yet
- Achillea FragrantissimaDocument5 pagesAchillea FragrantissimaMuhammad HasanNo ratings yet
- Gambaran Dan Lesi Rahang Pada Radiograf: Border Periosteal ReactionDocument6 pagesGambaran Dan Lesi Rahang Pada Radiograf: Border Periosteal ReactionI Dewa Ayu SavitriNo ratings yet
- Jake Yvan Dizon Case Study, Chapter 49, Assessment and Management of Patients With Hepatic DisordersDocument8 pagesJake Yvan Dizon Case Study, Chapter 49, Assessment and Management of Patients With Hepatic DisordersJake Yvan DizonNo ratings yet
- DR Amao Core Principles of Interpreting Ecg TracingDocument39 pagesDR Amao Core Principles of Interpreting Ecg Tracingdan ekelemeNo ratings yet
- Taper Dosing CalculatorDocument1 pageTaper Dosing Calculatorandirio7486No ratings yet
- Alloderm - Breast ReconstructionDocument180 pagesAlloderm - Breast ReconstructionFlorina PopaNo ratings yet
- Chapter17 Golong PPTDocument24 pagesChapter17 Golong PPTSamii JoNo ratings yet
- 2.1 Common Childhood Sense Organ AilmentsDocument30 pages2.1 Common Childhood Sense Organ AilmentsMary Christine RagueroNo ratings yet
- Piero Cascone 2017Document6 pagesPiero Cascone 2017João Paulo DutraNo ratings yet
- Chapter 18 Vaccines and Sera - StudentDocument27 pagesChapter 18 Vaccines and Sera - StudentKumarswamy BNo ratings yet
- Bragdon V AbbottDocument22 pagesBragdon V AbbottZNo ratings yet
- Workplace Handbook Version 2 Sept 13 2021Document108 pagesWorkplace Handbook Version 2 Sept 13 2021Joseph Raymund BautistaNo ratings yet
- Wound Cleansing: Benefits of Hypochlorous AcidDocument5 pagesWound Cleansing: Benefits of Hypochlorous Acidlps DiamondNo ratings yet
- Advocacy in PharmacyDocument3 pagesAdvocacy in PharmacyZofia RanadaNo ratings yet
- Clasification of Erectile DysfunctionDocument3 pagesClasification of Erectile DysfunctionSebastian Cardona LondoñoNo ratings yet
- Penyakit Jantung KongenitalDocument30 pagesPenyakit Jantung KongenitalrintiikNo ratings yet