You might also like
- Afterlife: The Strange Science of DecayDocument4 pagesAfterlife: The Strange Science of DecayPhoenix Che-LaiNo ratings yet
- Condensate Drain Calculation - Lab AHU PDFDocument1 pageCondensate Drain Calculation - Lab AHU PDFAltaf KhanNo ratings yet
- CD007449 Abstract PDFDocument3 pagesCD007449 Abstract PDFShintya ShintyaNo ratings yet
- Wiysonge Et Al-2017-Cochrane Database of Systematic ReviewsDocument4 pagesWiysonge Et Al-2017-Cochrane Database of Systematic ReviewsAnthony John A. MagnoNo ratings yet
- Vuorio Et Al-2019-Cochrane Database of Systematic ReviewsDocument49 pagesVuorio Et Al-2019-Cochrane Database of Systematic ReviewslesterNo ratings yet
- Hazlewood 2016 Methotrexate Monotherapy and MethotDocument68 pagesHazlewood 2016 Methotrexate Monotherapy and MethotPeter petroffNo ratings yet
- CD004649 AbstractDocument3 pagesCD004649 AbstractTheresa Binayu PrabhawatiNo ratings yet
- CD007187 StandardDocument94 pagesCD007187 StandardmariobrosiNo ratings yet
- Daley Et Al-2014-Cochrane Database of Systematic ReviewsDocument22 pagesDaley Et Al-2014-Cochrane Database of Systematic ReviewsJoaquín Guillermo González ArocaNo ratings yet
- Terapi rekompresi penyakit dekompresiDocument26 pagesTerapi rekompresi penyakit dekompresiJohn HetharieNo ratings yet
- Corticosteroids For Periorbital and Orbital Cellulitis (Protocol)Document23 pagesCorticosteroids For Periorbital and Orbital Cellulitis (Protocol)Putri kartiniNo ratings yet
- Hahn Et Al-2018-Cochrane Database of Systematic ReviewsDocument76 pagesHahn Et Al-2018-Cochrane Database of Systematic Reviewscarlos huertaNo ratings yet
- CD005491Document44 pagesCD005491Robert ThiodorusNo ratings yet
- GBS Review2Document64 pagesGBS Review2Vladimir BasurtoNo ratings yet
- Article 1608375149Document3 pagesArticle 1608375149devstararnNo ratings yet
- Hydrochlorothiazide Versus Chlorthalidone: Brief ReviewDocument6 pagesHydrochlorothiazide Versus Chlorthalidone: Brief ReviewAnj RodriguezNo ratings yet
- Bradford Et Al-2020-Cochrane Database of Systematic ReviewsDocument37 pagesBradford Et Al-2020-Cochrane Database of Systematic ReviewsCarla Jacqueline Duménez AranedaNo ratings yet
- 9Document520 pages9parameswarannirushanNo ratings yet
- Liu Et Al-2021-Cochrane Database of Systematic ReviewsDocument31 pagesLiu Et Al-2021-Cochrane Database of Systematic ReviewsNurlyanti RustamNo ratings yet
- AnsiedadeDocument15 pagesAnsiedadeTayná MayerNo ratings yet
- CD013180Document12 pagesCD013180Yoya LoyaNo ratings yet
- Health Teaching Plan: Dontogan, JohannahDocument5 pagesHealth Teaching Plan: Dontogan, JohannahRushnol Jade Piluden-TupacNo ratings yet
- Nielsen Et Al-2019-Cochrane Database of Systematic ReviewsDocument4 pagesNielsen Et Al-2019-Cochrane Database of Systematic ReviewsRobbie ShawNo ratings yet
- A Comparitive Clinical Study of Chaturushan On Modifiable Factors of Framingham Heart Score in Cardio-Vascular RiskDocument12 pagesA Comparitive Clinical Study of Chaturushan On Modifiable Factors of Framingham Heart Score in Cardio-Vascular RiskIJAR JOURNALNo ratings yet
- Dosis Estrés 2019Document6 pagesDosis Estrés 2019Braulio SantanaNo ratings yet
- Low Et Al-2016-Cochrane Database of Systematic ReviewsDocument55 pagesLow Et Al-2016-Cochrane Database of Systematic ReviewsGeuman ChajgoNo ratings yet
- JAyurvedaIntegrMed LSParticle PDFDocument10 pagesJAyurvedaIntegrMed LSParticle PDFMayank kNo ratings yet
- Blood Pressure Lowering Eficacy of Coenzyme Q10 For PrimaryDocument24 pagesBlood Pressure Lowering Eficacy of Coenzyme Q10 For PrimaryRaquel SennaNo ratings yet
- Treatment For Subclinical Hyperthyroidism in Adults (Protocol)Document4 pagesTreatment For Subclinical Hyperthyroidism in Adults (Protocol)Anisa Iswari Pombaile-NgurawanNo ratings yet
- 2021 02 19 21252066v1 FullDocument29 pages2021 02 19 21252066v1 FullВадим ЖебельNo ratings yet
- Principles of Fluid ManagementDocument17 pagesPrinciples of Fluid ManagementBrainy-Paykiesaurus LuminirexNo ratings yet
- Treatment For Amphetamine WithdrawalDocument24 pagesTreatment For Amphetamine WithdrawalJosé Antonio Alves VilelaNo ratings yet
- Non Pharmacologic Interventions For Reducing Blood Pressure in Adults With Prehypertension To EstablishedDocument138 pagesNon Pharmacologic Interventions For Reducing Blood Pressure in Adults With Prehypertension To EstablishedMargarida LouçãoNo ratings yet
- JCH 6 532Document9 pagesJCH 6 532Yanski DarmantoNo ratings yet
- Scientific Evidence-Based Effects of Hydrotherapy On Various Systems of The BodyDocument16 pagesScientific Evidence-Based Effects of Hydrotherapy On Various Systems of The Bodydonald duckNo ratings yet
- Losartan Fda Bioequivalence RecenteDocument6 pagesLosartan Fda Bioequivalence Recentelamouna.lamittaNo ratings yet
- Nomor 1 Jawabannya Di Abstrak Dalam Hasil Dan DiskusiDocument6 pagesNomor 1 Jawabannya Di Abstrak Dalam Hasil Dan DiskusiPache ChristyoNo ratings yet
- Improvement Ul Function Stroke PtsDocument138 pagesImprovement Ul Function Stroke PtsKandi IssayaNo ratings yet
- Critical Review On Trends in Hydrotherapy ResearchDocument27 pagesCritical Review On Trends in Hydrotherapy ResearchPuneeth RaghavendraNo ratings yet
- Dafpus SGB 20Document32 pagesDafpus SGB 20Anggie Pradetya MaharaniNo ratings yet
- Advance Treatment DirectivesDocument38 pagesAdvance Treatment DirectivesidiosyncraticroutineNo ratings yet
- Rodrigues 2019Document43 pagesRodrigues 2019Santoso SantosoNo ratings yet
- Chlorthalidone, Not Hydrochlorothiazide, Is The Right Diuretic For ComparisonDocument2 pagesChlorthalidone, Not Hydrochlorothiazide, Is The Right Diuretic For ComparisonZeba Sohel KhatriNo ratings yet
- Effects of Dietary Salt On Blood Pressure: January 2015Document7 pagesEffects of Dietary Salt On Blood Pressure: January 2015Zainal AbidinNo ratings yet
- Yoga For Hypertension Posadzki2014Document12 pagesYoga For Hypertension Posadzki2014sipen poltekkesbdgNo ratings yet
- Endocrine Abnormalities in Dilated CardiomyopathyDocument5 pagesEndocrine Abnormalities in Dilated CardiomyopathyAditya SutarNo ratings yet
- The Relationship Between Hydration Status Male Sexual Dysfunction and Depression in Hemodialysis PatientsDocument8 pagesThe Relationship Between Hydration Status Male Sexual Dysfunction and Depression in Hemodialysis PatientsMirko ĆalićNo ratings yet
- Kleinst-Uber Et Al-2014-Cochrane Database of Systematic ReviewsDocument138 pagesKleinst-Uber Et Al-2014-Cochrane Database of Systematic Reviewsokdi pranciscoNo ratings yet
- CD 013260Document25 pagesCD 013260arya wismaNo ratings yet
- KJP2019 02 21Document6 pagesKJP2019 02 21vladislav stankovicNo ratings yet
- Amatya Et Al-2019-Cochrane Database of Systematic ReviewsDocument43 pagesAmatya Et Al-2019-Cochrane Database of Systematic ReviewsAna CostaNo ratings yet
- Harris Et Al-2020-Cochrane Database of Systematic ReviewsDocument15 pagesHarris Et Al-2020-Cochrane Database of Systematic Reviewsgp mhknNo ratings yet
- GNRH 2021Document67 pagesGNRH 2021Sara HossamNo ratings yet
- Improvement Cochrane 2014Document140 pagesImprovement Cochrane 2014Kandi IssayaNo ratings yet
- 2023 - Lower Versus Higher Exposure To Vasopressor Therapy in Vasodilatory Hypotension RSL With Meta-AnalysisDocument13 pages2023 - Lower Versus Higher Exposure To Vasopressor Therapy in Vasodilatory Hypotension RSL With Meta-AnalysisgiseladlrNo ratings yet
- Indian Heart Journal: EditorialDocument4 pagesIndian Heart Journal: Editorialgisella hapsariNo ratings yet
- Redefining Diuretics Use in Hypertension Why.6Document13 pagesRedefining Diuretics Use in Hypertension Why.6michaelwillsonNo ratings yet
- CD 010406Document80 pagesCD 010406capistranflorespalomaNo ratings yet
- CD 004303Document26 pagesCD 004303u3505483No ratings yet
- STEROID IIDocument57 pagesSTEROID IIMurtaza MuhammadNo ratings yet
- Phytomedicine: Garlic For Hypertension: A Systematic Review and Meta-AnalysisDocument10 pagesPhytomedicine: Garlic For Hypertension: A Systematic Review and Meta-Analysisnini_popaNo ratings yet
- SSRN Id2118772Document22 pagesSSRN Id2118772VenessaEdeNo ratings yet
- J ctt18mvnq0 6Document9 pagesJ ctt18mvnq0 6VenessaEdeNo ratings yet
- 10.4159 Harvard.9780674435865.fmDocument6 pages10.4159 Harvard.9780674435865.fmVenessaEdeNo ratings yet
- The Silent Treatment of Class Domination: Critical' Comparative Capitalisms Scholarship and The British StateDocument13 pagesThe Silent Treatment of Class Domination: Critical' Comparative Capitalisms Scholarship and The British StateVenessaEdeNo ratings yet
- J Microc 2020 105027Document31 pagesJ Microc 2020 105027VenessaEdeNo ratings yet
- Rubric Assessment - (2023SP-NURS-3015-B01) Pharmacology - SUNY 1735912397669655Document8 pagesRubric Assessment - (2023SP-NURS-3015-B01) Pharmacology - SUNY 1735912397669655VenessaEdeNo ratings yet
- Ilovepdf MergedDocument9 pagesIlovepdf MergedVenessaEdeNo ratings yet
- Ilovepdf MergedDocument9 pagesIlovepdf MergedVenessaEdeNo ratings yet
- TL102 0 2024 Che3701 0Document12 pagesTL102 0 2024 Che3701 0sollomontlou06No ratings yet
- Breast CancerDocument1 pageBreast CancerAdang FirmansyahNo ratings yet
- Covid19 - Attendance Book, Visitors Book, Field AuditDocument7 pagesCovid19 - Attendance Book, Visitors Book, Field AuditmakhalNo ratings yet
- Kata Kunci: Pengetahuan Gizi Seimbang, Praktik Gizi SeimbangDocument9 pagesKata Kunci: Pengetahuan Gizi Seimbang, Praktik Gizi SeimbangShifa Minhatun Niza'No ratings yet
- Wood Gas Generator or NLDocument94 pagesWood Gas Generator or NLToddharrisNo ratings yet
- Argumentative Essay-Nursing HomesDocument1 pageArgumentative Essay-Nursing HomesHM TanNo ratings yet
- Aprinnova Simply Solid One Page SummaryDocument2 pagesAprinnova Simply Solid One Page SummaryPatrick FlowerdayNo ratings yet
- Ijpcr 22 309Document6 pagesIjpcr 22 309Sriram NagarajanNo ratings yet
- X PPT CH 12 ElectricityDocument12 pagesX PPT CH 12 ElectricityAakriti100% (1)
- PETROWIKI LINKDocument136 pagesPETROWIKI LINKAyush ChandraNo ratings yet
- BurgerKing Versus McDonaldsDocument4 pagesBurgerKing Versus McDonaldsmarkus johannessenNo ratings yet
- Wire Rope Slings Si 2 - 2 EmmDocument2 pagesWire Rope Slings Si 2 - 2 EmmheppyfaebanffNo ratings yet
- 2 Second Grade English Diagnostic Test (Autoguardado)Document5 pages2 Second Grade English Diagnostic Test (Autoguardado)MELISSA KARENTH MONTES PINTONo ratings yet
- The Scientific Facts About WaterDocument7 pagesThe Scientific Facts About WaterNizam HasniNo ratings yet
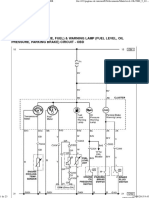
- Dokumen - Tips Daewoo Service Manual Instrument Cluster Matiz-2023Document23 pagesDokumen - Tips Daewoo Service Manual Instrument Cluster Matiz-2023urexalg AlgériaNo ratings yet
- ACKSDocument4 pagesACKSPinky Bhattacharyya50% (2)
- 2000-03 Taconic Running Life March 2000Document24 pages2000-03 Taconic Running Life March 2000TaconicArchiveNo ratings yet
- Ethics in Animal-Based Research: Dominik Gross René H. TolbaDocument15 pagesEthics in Animal-Based Research: Dominik Gross René H. TolbaIuliana MogaNo ratings yet
- Cerebrospinal Fluid Penetration of Amikacin in Children With Community-Acquired Bacterial MeningitisDocument3 pagesCerebrospinal Fluid Penetration of Amikacin in Children With Community-Acquired Bacterial MeningitisDanny JacobusNo ratings yet
- Brochure HMS LIME 12-04-22 V21Document14 pagesBrochure HMS LIME 12-04-22 V21i10 Sport PlusNo ratings yet
- Guide To Rural England - ShropshireDocument54 pagesGuide To Rural England - ShropshireTravel Publishing100% (2)
- If You Have Guts Then Dare To Be DIFFERENTDocument20 pagesIf You Have Guts Then Dare To Be DIFFERENTChirag Saiya (PHILOSOPHER) - SPIRITUAL Speaker and Writer100% (1)
- MetallizationDocument51 pagesMetallizationjust4u2cjoshy67% (3)
- Bonding in Organic Compounds - Organic Synthesis Marks SchemeDocument96 pagesBonding in Organic Compounds - Organic Synthesis Marks SchemeRaiyan RahmanNo ratings yet
- Questionnaire - Yash PareekDocument4 pagesQuestionnaire - Yash PareekYash PareekNo ratings yet
- CH 2Document123 pagesCH 2Caitlin HurleyNo ratings yet
- SAFETY NAVIGATION MANAGEMENT at MALACCA STRAIT PDFDocument18 pagesSAFETY NAVIGATION MANAGEMENT at MALACCA STRAIT PDFAditama Dirga100% (1)
- Federal Democratic Republic of Ethiopia's 2017 Voluntary National Reviews on SDGsDocument52 pagesFederal Democratic Republic of Ethiopia's 2017 Voluntary National Reviews on SDGsAshagre MekuriaNo ratings yet