You might also like
- Muscular Assessment ChecklistDocument2 pagesMuscular Assessment ChecklistSherma Sheikh karimNo ratings yet
- The Chicago Review Press NCLEX-RN Practice Test and ReviewFrom EverandThe Chicago Review Press NCLEX-RN Practice Test and ReviewRating: 4 out of 5 stars4/5 (20)
- CRS-R Manual20201210Document17 pagesCRS-R Manual20201210Maria CeciliaNo ratings yet
- Nursing Role of Cardiac and Respiratory Arrest Checklist 2022 ApproveDocument3 pagesNursing Role of Cardiac and Respiratory Arrest Checklist 2022 ApproveDo0odi AlharbiNo ratings yet
- GUIA PEDIATRIA REVISADA MALLA 2018 - RemovedDocument8 pagesGUIA PEDIATRIA REVISADA MALLA 2018 - RemovedYostin SokoNo ratings yet
- How to perform MODIFIED RANKIN SCALE ASSESSMENTSDocument15 pagesHow to perform MODIFIED RANKIN SCALE ASSESSMENTSKNI Maret 2023No ratings yet
- WEEK-4 - LectureDocument2 pagesWEEK-4 - LectureBritney TamuraNo ratings yet
- EMS audit checklistDocument6 pagesEMS audit checklistArati GuptaNo ratings yet
- Objective Structured Practical ExamDocument37 pagesObjective Structured Practical ExamDr.Mohammad Idrees AnwarNo ratings yet
- Central Mindanao University: Scale Description Interpretation Assistance NeededDocument2 pagesCentral Mindanao University: Scale Description Interpretation Assistance NeededBrandon Sydnee GonzalesNo ratings yet
- Information:: YellowDocument6 pagesInformation:: YellowAkhosh KrishnaNo ratings yet
- Using The Glasgow Coma Scale For Patient AssessmentDocument7 pagesUsing The Glasgow Coma Scale For Patient AssessmentJasmin Dela TorreNo ratings yet
- Gross Motor and Balance TestsDocument21 pagesGross Motor and Balance TestsKristine CastilloNo ratings yet
- ED Documentation IssuesDocument26 pagesED Documentation IssuesMNo ratings yet
- Acf 21 Students FileDocument6 pagesAcf 21 Students FileElizabeth JadeNo ratings yet
- NEBOSH International General Certificate in Occupational Health and SafetyDocument5 pagesNEBOSH International General Certificate in Occupational Health and SafetyAshik MuhammedNo ratings yet
- AP Swine ORAL-QUESTIONING-CHECKLISTDocument6 pagesAP Swine ORAL-QUESTIONING-CHECKLISTdaniel,jr BALDOZNo ratings yet
- Sbar Simulation ReflectionDocument3 pagesSbar Simulation Reflectionapi-314635911100% (2)
- NEBOSH International General Certificate in Occupational Health and SafetyDocument4 pagesNEBOSH International General Certificate in Occupational Health and SafetyvarunNo ratings yet
- Our Lady of Fatima University College of Nursing-Valenzuela CityDocument2 pagesOur Lady of Fatima University College of Nursing-Valenzuela CityMichelle Gliselle Guinto MallareNo ratings yet
- Medical Centre AuditDocument10 pagesMedical Centre AuditKim-Honie RudmanNo ratings yet
- National Immunization Program: Manual of Procedures Booklet 9Document24 pagesNational Immunization Program: Manual of Procedures Booklet 9Blue PielagoNo ratings yet
- NEBOSH International General Certificate in Occupational Health and SafetyDocument11 pagesNEBOSH International General Certificate in Occupational Health and SafetybecpavanNo ratings yet
- Musculoskeletal Assessment ChecklistDocument2 pagesMusculoskeletal Assessment ChecklistThe Blue and Gold RvdNo ratings yet
- Activity #4: Review of Systems RubricDocument2 pagesActivity #4: Review of Systems Rubric하나No ratings yet
- The Confusion Assessment Method (CAM) : Training Manual and Coding GuideDocument28 pagesThe Confusion Assessment Method (CAM) : Training Manual and Coding GuideSze Wing LeeNo ratings yet
- Application Plan and Evaluation: Part 1. PlanningDocument1 pageApplication Plan and Evaluation: Part 1. PlanningVirendar SinghNo ratings yet
- 001_Vital Signs CheckingDocument3 pages001_Vital Signs CheckingIPC PFKCCNo ratings yet
- Evaluation FormsDocument13 pagesEvaluation FormsEastern SamarNo ratings yet
- Practice Assessment FormsDocument61 pagesPractice Assessment FormsKunj KaliwadaNo ratings yet
- Clinical EvaluationDocument13 pagesClinical EvaluationYousef JafarNo ratings yet
- Assessment-Task-1 SolutionDocument29 pagesAssessment-Task-1 SolutionMirajur Rahman 1722007No ratings yet
- College of The Bahamas Nursing Care PlanDocument2 pagesCollege of The Bahamas Nursing Care Planrhawnie_babyNo ratings yet
- NEBOSH IGC Health and Safety ReportDocument22 pagesNEBOSH IGC Health and Safety ReportFrank RustonNo ratings yet
- NCM 101 Health Assessment The Eyes: Prepared byDocument28 pagesNCM 101 Health Assessment The Eyes: Prepared byNicole NipasNo ratings yet
- Workplace Health and Safety Student Assessment Booklet (ID 161325)Document35 pagesWorkplace Health and Safety Student Assessment Booklet (ID 161325)Sanjay Rajbhandari100% (1)
- HLTAAP001 Recognise Healthy Body System SAB v3.3 - TheORYDocument38 pagesHLTAAP001 Recognise Healthy Body System SAB v3.3 - TheORYboldguy222No ratings yet
- Blank Ncm119 Nursing Leadership and Management BlankDocument3 pagesBlank Ncm119 Nursing Leadership and Management BlankGwy-Gwy Reyes De PazNo ratings yet
- Gc3 - The Health and Assessor's Marking Sheet Safety Practical ApplicationDocument26 pagesGc3 - The Health and Assessor's Marking Sheet Safety Practical ApplicationpilakkadNo ratings yet
- Supportive Supervision Tool For COVID - After Review With Lab Heads PDFDocument10 pagesSupportive Supervision Tool For COVID - After Review With Lab Heads PDFNzema NgakanaNo ratings yet
- IGC3 - Exam TemplateDocument11 pagesIGC3 - Exam TemplateSreenath Menon KNo ratings yet
- Final Principle - 1 - GPHC - Action - PlanDocument9 pagesFinal Principle - 1 - GPHC - Action - Planc.tupakulaNo ratings yet
- Mini Cex DopsDocument2 pagesMini Cex DopsandhitaNo ratings yet
- SITXFSA002 Assessment 2 - ObservationsDocument22 pagesSITXFSA002 Assessment 2 - ObservationsBaljeet Singh0% (2)
- The 4 Types of Vital SignsDocument30 pagesThe 4 Types of Vital SignsBarlusca JunrryNo ratings yet
- 3 7 Core Procedures APR 2011 FINAL PDFDocument33 pages3 7 Core Procedures APR 2011 FINAL PDFFlorinaZamfirNo ratings yet
- Module One Wellness Plan: GO TO FILE - Choose SAVE AS - Save A Copy of This To Your Computer!Document10 pagesModule One Wellness Plan: GO TO FILE - Choose SAVE AS - Save A Copy of This To Your Computer!Lauren EmNo ratings yet
- 3D-CAM Training Manual Clinical For Website Version 2.1 Final 9-8-14Document15 pages3D-CAM Training Manual Clinical For Website Version 2.1 Final 9-8-14Anonymous 8b1lZnQ0% (1)
- M3A1 EHR Go Case Study Review (Associate)Document4 pagesM3A1 EHR Go Case Study Review (Associate)srgilbert01No ratings yet
- HLTINF006 Student Assessment Task 3Document14 pagesHLTINF006 Student Assessment Task 3Rebeca RaducuNo ratings yet
- Module-6 Instrumenation PracticalDocument18 pagesModule-6 Instrumenation PracticalStephane Durel MbidaNo ratings yet
- IMI RANO Critieria Booklet Nov 2011Document18 pagesIMI RANO Critieria Booklet Nov 2011johnthomas75No ratings yet
- TR - Fish Capture NC IDocument95 pagesTR - Fish Capture NC IInternational Technology Center IncNo ratings yet
- TR Fidh Capture NC IDocument95 pagesTR Fidh Capture NC IInternational Technology Center IncNo ratings yet
- Myers SOP example - Balance VerificationDocument7 pagesMyers SOP example - Balance VerificationRoyal BimhahNo ratings yet
- Pathfit Journal Week 6-3Document4 pagesPathfit Journal Week 6-3Eunice Dimple Caliwag100% (1)
- Assessment Guide - First AidDocument21 pagesAssessment Guide - First AidNiel Brian VillarazoNo ratings yet
- Glasgow Coma Scale Monitoring and DocumentationDocument47 pagesGlasgow Coma Scale Monitoring and DocumentationTripti Pun100% (1)
- Specialty Rotation MayoDocument6 pagesSpecialty Rotation Mayoapi-733590799No ratings yet
- Nucleus ERPDocument3 pagesNucleus ERPdimensionone1No ratings yet
- Filipinism 3Document3 pagesFilipinism 3Shahani Cel MananayNo ratings yet
- Universiti Teknologi Mara Odl Test 1: Confidential 1 EM/ MAY 2020/MEM603Document4 pagesUniversiti Teknologi Mara Odl Test 1: Confidential 1 EM/ MAY 2020/MEM603000No ratings yet
- Man Ssa Ug en 0698Document43 pagesMan Ssa Ug en 0698Andy LNo ratings yet
- Spru I 11444Document24 pagesSpru I 11444aalvarcaNo ratings yet
- Telstra Strategic Issues and CEO Leadership Briefing PaperDocument16 pagesTelstra Strategic Issues and CEO Leadership Briefing PaperIsabel Woods100% (1)
- Huawei Technologies Network Router B681Document12 pagesHuawei Technologies Network Router B681Eduardo Vaz RibeiroNo ratings yet
- SC Project Closeout Report v6Document27 pagesSC Project Closeout Report v6SateeshIngoleNo ratings yet
- Lesson Plan SETS 2 PDFDocument10 pagesLesson Plan SETS 2 PDFHelmi Tarmizi83% (6)
- Mobilization and Participation: Social-Psychological Expansisons of Resource Mobilization TheoryDocument19 pagesMobilization and Participation: Social-Psychological Expansisons of Resource Mobilization TheoryJoaquim OliveiraNo ratings yet
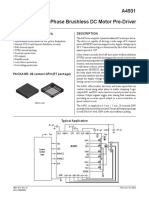
- A4931 DatasheetDocument12 pagesA4931 DatasheetDiego HernandezNo ratings yet
- jrc122457 Dts Survey Deliverable Ver. 5.0-3Document46 pagesjrc122457 Dts Survey Deliverable Ver. 5.0-3Boris Van CyrulnikNo ratings yet
- MDP Module 2Document84 pagesMDP Module 2ADITYA RAJ CHOUDHARYNo ratings yet
- Jhamuna Tower Design DataDocument15 pagesJhamuna Tower Design DataArindam RoyNo ratings yet
- Abdul Jabbar (Mechanical Engineer) AGROFEED KSADocument4 pagesAbdul Jabbar (Mechanical Engineer) AGROFEED KSAftimum1No ratings yet
- DNV OS-B101 Metallic MaterialsDocument48 pagesDNV OS-B101 Metallic MaterialsBoni Luck100% (1)
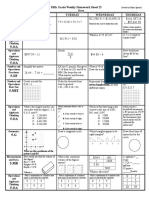
- 3 6 17weekly Homework Sheet Week 23 - 5th Grade - CcssDocument3 pages3 6 17weekly Homework Sheet Week 23 - 5th Grade - Ccssapi-328344919No ratings yet
- BrochureDocument2 pagesBrochureNarayanaNo ratings yet
- BITS Vulnerability Management Maturity ModelDocument19 pagesBITS Vulnerability Management Maturity ModelJack JacksonNo ratings yet
- Uop Teuop-Tech-And-More-Air-Separation-Adsorbents-Articlech and More Air Separation Adsorbents ArticleDocument8 pagesUop Teuop-Tech-And-More-Air-Separation-Adsorbents-Articlech and More Air Separation Adsorbents ArticleRoo FaNo ratings yet
- Intro To Factor AnalysisDocument52 pagesIntro To Factor AnalysisRawnak JahanNo ratings yet
- SpinView Getting StartedDocument16 pagesSpinView Getting StartedRicardo SequeiraNo ratings yet
- Enlightened DespotismDocument19 pagesEnlightened Despotismmeghna mNo ratings yet
- Switches Demystified Assembly PDFDocument1 pageSwitches Demystified Assembly PDFkocekoNo ratings yet
- Omni Lifenet SpecsDocument2 pagesOmni Lifenet SpecsAngel JuarezNo ratings yet
- RADEMAKER) Sophrosyne and The Rhetoric of Self-RestraintDocument392 pagesRADEMAKER) Sophrosyne and The Rhetoric of Self-RestraintLafayers100% (2)
- Memo-on-Orientation and Submission of PNPKIDocument5 pagesMemo-on-Orientation and Submission of PNPKICoronia Mermaly LamsenNo ratings yet
- The Practice of Medicinal Chemistry, 4th EditionDocument2 pagesThe Practice of Medicinal Chemistry, 4th Editionlibrary25400% (1)
- KiaOptima Seccion 002Document7 pagesKiaOptima Seccion 002Luis Enrique PeñaNo ratings yet
- Vedic Maths - India's Approach To Calculating!Document4 pagesVedic Maths - India's Approach To Calculating!padmanaban_cse100% (2)