You might also like
- وضعيات ViewDocument23 pagesوضعيات ViewomarNo ratings yet
- Protocol and Technique ChartDocument5 pagesProtocol and Technique ChartvictoriaNo ratings yet
- Posisi Rontgen KonvensionalDocument3 pagesPosisi Rontgen Konvensionalainil mardiahNo ratings yet
- Form Permintaan PX RadiologiDocument3 pagesForm Permintaan PX Radiologiradiologi syifaNo ratings yet
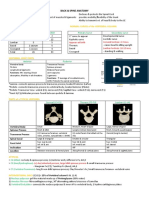
- Data Sheet of X-Ray With PictureDocument14 pagesData Sheet of X-Ray With PictureZihad DmrtNo ratings yet
- Data Sheet of X-Ray VeiwDocument1 pageData Sheet of X-Ray VeiwZihad DmrtNo ratings yet
- RM 095 Permintaan Pemeriksaan LaboratoriumDocument2 pagesRM 095 Permintaan Pemeriksaan Laboratoriumagus sabdarNo ratings yet
- MSK Protocols 082020Document116 pagesMSK Protocols 082020Murat EksiNo ratings yet
- RM 099-Ii-2017-Rev Permintaan Pemeriksaan RadiologiDocument1 pageRM 099-Ii-2017-Rev Permintaan Pemeriksaan RadiologiFitriani Ciboru CopangNo ratings yet
- Rangkuman FrakturDocument12 pagesRangkuman FrakturalexNo ratings yet
- Survey Report GRDocument13 pagesSurvey Report GRLena Tas BatamNo ratings yet
- Blanko Pemeriksaan Rad LuarDocument1 pageBlanko Pemeriksaan Rad Luarradiologi rsud solokNo ratings yet
- Clavicle, AC Joints and Scapula Procedures - 2020Document21 pagesClavicle, AC Joints and Scapula Procedures - 2020Melanie RamdassNo ratings yet
- 17 Lower Extremity (FINAL)Document32 pages17 Lower Extremity (FINAL)kath-kath100% (1)
- Jenis Pemeriksaan Konvesional RadiologiDocument1 pageJenis Pemeriksaan Konvesional RadiologiDyah PurwitaNo ratings yet
- Approaches Summary Ortho PDFDocument4 pagesApproaches Summary Ortho PDFgehadbeddaNo ratings yet
- Terminology: Basic Terms of RelationsDocument11 pagesTerminology: Basic Terms of RelationsAzkia InayahNo ratings yet
- Pelvis-2019 AbadierrrtDocument47 pagesPelvis-2019 AbadierrrtGenevieve Marie MacabudbudNo ratings yet
- Screenshot - Hip and Knee ComplexDocument8 pagesScreenshot - Hip and Knee Complexno nameNo ratings yet
- RadPos Summary 2Document9 pagesRadPos Summary 2Jocel LongosNo ratings yet
- Pelvic GirdleDocument4 pagesPelvic GirdleGynewNo ratings yet
- General X-Ray ProjectionsDocument19 pagesGeneral X-Ray ProjectionsattooNo ratings yet
- Positioning QuizzesDocument7 pagesPositioning QuizzesSahaj PrakashNo ratings yet
- Posture Assessment SheetDocument1 pagePosture Assessment Sheetharmziie100% (1)
- UME Radiology Musculoskeletal Imaging (Review)Document52 pagesUME Radiology Musculoskeletal Imaging (Review)Nguyễn Hoàng SơnNo ratings yet
- Ears: Nose: EyeDocument1 pageEars: Nose: Eyeapi-72312524No ratings yet
- Sample Patient Initial EvaluationDocument8 pagesSample Patient Initial EvaluationYang TubioNo ratings yet
- PositioningDocument22 pagesPositioningRadio MVMCNo ratings yet
- Midterm Practical (Alphabet Exercise A-I)Document2 pagesMidterm Practical (Alphabet Exercise A-I)Princess Trixie SalvadorNo ratings yet
- Vertebral ColumnDocument84 pagesVertebral ColumnGenesis GeronagaNo ratings yet
- Formulir Permintaan Pemeriksaan Radiologi: RontgenDocument2 pagesFormulir Permintaan Pemeriksaan Radiologi: RontgenIRAYANANo ratings yet
- CTprotocols MSK PDFDocument72 pagesCTprotocols MSK PDFdrqazi777No ratings yet
- radio-UL, Pelvic, LLDocument125 pagesradio-UL, Pelvic, LLsirfayNo ratings yet
- Possible Q N ADocument5 pagesPossible Q N ANisrina Nur FitrayaniNo ratings yet
- Pemerintah Provinsi Maluku No - Rekam Medis:: Rsud Dr. H. Ishak UmarellaDocument3 pagesPemerintah Provinsi Maluku No - Rekam Medis:: Rsud Dr. H. Ishak UmarellaEjha JackvegaNo ratings yet
- Cervical Proyeksi Ap Open MouthDocument17 pagesCervical Proyeksi Ap Open MouthAgil SarengatNo ratings yet
- Upper Xtrem QuesDocument9 pagesUpper Xtrem QuesSahaj PrakashNo ratings yet
- Calcaneus: Weight-Bearing Coalition PositionDocument5 pagesCalcaneus: Weight-Bearing Coalition PositionHazel ConjeNo ratings yet
- Balance Notes PDFDocument4 pagesBalance Notes PDFFarhan Ullah KhanNo ratings yet
- Back Spine AnatomyDocument3 pagesBack Spine AnatomyNinjaNo ratings yet
- Rad Posi Prelim (Sir Mike)Document29 pagesRad Posi Prelim (Sir Mike)Mark Cielo PeraltaNo ratings yet
- CVS, Respi Heent ExamDocument8 pagesCVS, Respi Heent ExamDranreb Berylle MasangkayNo ratings yet
- Radiography of The Thoracic SpineDocument59 pagesRadiography of The Thoracic SpineEzra NserekoNo ratings yet
- Ue MMTDocument5 pagesUe MMTKali AceñaNo ratings yet
- My Powerlifting SpreadsheetDocument39 pagesMy Powerlifting Spreadsheetberstuck100% (1)
- Skull: by NurohmanDocument106 pagesSkull: by NurohmanAdi SupriyantoNo ratings yet
- Radiology Final ChartDocument5 pagesRadiology Final Chartwhatsup11No ratings yet
- Examination of The ShoulderDocument33 pagesExamination of The ShoulderAnonymous 9QxPDpNo ratings yet
- Position, Chapter 5 Thorax and AbdomenDocument30 pagesPosition, Chapter 5 Thorax and Abdomengirmateddy437No ratings yet
- Pelvis (Summary)Document6 pagesPelvis (Summary)Michaella SangcapNo ratings yet
- Integrated Anatomy: Imaging: of The SpineDocument13 pagesIntegrated Anatomy: Imaging: of The SpineFlo RenceNo ratings yet
- CAPM Exam 3Document11 pagesCAPM Exam 3wamaithamargaret257No ratings yet
- SKULLDocument105 pagesSKULLradiologi stikescirebonNo ratings yet
- نسخة نسخة الاشعةDocument10 pagesنسخة نسخة الاشعةDina MohamedNo ratings yet
- Tender Point Reference SheetDocument12 pagesTender Point Reference SheetSafariDuckNo ratings yet
- Handouts SkullDocument17 pagesHandouts Skullkearlleomacahilas13No ratings yet
- Radiographic Positioning: (Reinforcement)Document646 pagesRadiographic Positioning: (Reinforcement)BeverlyNo ratings yet
- Upper Extremity Venous Protocol 14Document2 pagesUpper Extremity Venous Protocol 14api-349402240No ratings yet
- The American Physical Therapy Association Book of Body Repair and Maintenance: Hundreds of Stretches and Exercises for Every Part of the Human BodyFrom EverandThe American Physical Therapy Association Book of Body Repair and Maintenance: Hundreds of Stretches and Exercises for Every Part of the Human BodyRating: 4 out of 5 stars4/5 (9)
- 3.3 Fish Pituitary GlandDocument12 pages3.3 Fish Pituitary GlandOla Joel Ajamu0% (1)
- Ceph (2) / Orthodontic Courses by Indian Dental AcademyDocument112 pagesCeph (2) / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
- Chapter # 1Document19 pagesChapter # 1Hadiqa Afzal855No ratings yet
- Friedman and Daeshler 2006 Late Devonian (Famennian) Lungfishes From The Catskill Formation of Pennsylvania, UsaDocument17 pagesFriedman and Daeshler 2006 Late Devonian (Famennian) Lungfishes From The Catskill Formation of Pennsylvania, UsaFernando Arthur GregolNo ratings yet
- Cummings 6th Ed TitlesDocument8 pagesCummings 6th Ed TitlesBurhan QureshiNo ratings yet
- Anatomy - Physiology (Chapter 6 - Skeletal System)Document43 pagesAnatomy - Physiology (Chapter 6 - Skeletal System)Kyla DuenaNo ratings yet
- Degisim SinaviDocument28 pagesDegisim SinaviaytajNo ratings yet
- Intrapartum NCM 107Document8 pagesIntrapartum NCM 107Kimberly Sharah Mae FortunoNo ratings yet
- Handouts in Skeletal SystemDocument6 pagesHandouts in Skeletal SystemShiela Mae EslumNo ratings yet
- Viswass School & College of Nursing GNM 1 Year Anatomy and Physiology UNIT-13 The Skeletal System Long Questions and AnswersDocument33 pagesViswass School & College of Nursing GNM 1 Year Anatomy and Physiology UNIT-13 The Skeletal System Long Questions and Answersshubham vermaNo ratings yet
- The Beginnings of Filipino Society and Culture 1962Document5 pagesThe Beginnings of Filipino Society and Culture 1962Merra Mae S. ArmadaNo ratings yet
- TNCC StudyDocument22 pagesTNCC StudyDallas Lindsey100% (5)
- Osteology of Maxillofacial Skeleton IDocument36 pagesOsteology of Maxillofacial Skeleton Isailajanekkanti03No ratings yet
- List Procedur ICD-9CMDocument232 pagesList Procedur ICD-9CMEKO FEBRIANTORONo ratings yet
- Perimortem Trauma in King Richard III: A Skeletal Analysis: ArticlesDocument7 pagesPerimortem Trauma in King Richard III: A Skeletal Analysis: ArticlesFredgar22No ratings yet
- The Skeletal System HDocument23 pagesThe Skeletal System HRajorshi MishraNo ratings yet
- The Nursing Care of A Family With A NewbornDocument5 pagesThe Nursing Care of A Family With A NewbornDonell EscalanteNo ratings yet
- Forensic Science Forensic AnthropologyDocument3 pagesForensic Science Forensic Anthropologyapi-261373114No ratings yet
- Anatomy of The Scalp and FaceDocument33 pagesAnatomy of The Scalp and FaceSaidu TanimuNo ratings yet
- Guidelines About Head and Neck Regio1-1Document20 pagesGuidelines About Head and Neck Regio1-1zeeshanNo ratings yet
- Novel Surgical Approach To AcalvariaDocument2 pagesNovel Surgical Approach To AcalvariaKezia Rachellea MustakimNo ratings yet
- Anatomy and Physiology 6th Edition Marieb Solutions ManualDocument20 pagesAnatomy and Physiology 6th Edition Marieb Solutions Manualstephenthanh1huo100% (28)
- A Typical Kronlein Shot? A Rare Case of Submental-Facio-Cranial Bullet Trajectory With Brain ExenterationDocument4 pagesA Typical Kronlein Shot? A Rare Case of Submental-Facio-Cranial Bullet Trajectory With Brain ExenterationValdi DwiramaNo ratings yet
- Cephalohematoma, CaputDocument5 pagesCephalohematoma, CaputSusana TorresNo ratings yet
- Hospital Corpsman ManualDocument574 pagesHospital Corpsman ManualNes Navarro100% (1)
- Anatomi Kepala Dan Leher: Oleh: Abdullah Putra Perdana Ppds Ilmu Bedah FK Ulm 2017Document32 pagesAnatomi Kepala Dan Leher: Oleh: Abdullah Putra Perdana Ppds Ilmu Bedah FK Ulm 2017drhendyjuniorNo ratings yet
- Cephalometric RadiographyDocument8 pagesCephalometric Radiographymkhaddas100% (3)
- Ricketts Lateral Ceph ChartDocument1 pageRicketts Lateral Ceph ChartMinh Đạt100% (1)
- m4 MCN - m4Document140 pagesm4 MCN - m4Kristine KimNo ratings yet
- 3D Printed Bone Models in Oral and Cranio-Maxillofacial Surgery: A Systematic ReviewDocument19 pages3D Printed Bone Models in Oral and Cranio-Maxillofacial Surgery: A Systematic ReviewWahyuNo ratings yet