You might also like
- A Decade of Dementia Care Training Learning Needs PDFDocument10 pagesA Decade of Dementia Care Training Learning Needs PDFYovana Pachón PovedaNo ratings yet
- Uworld RationalesDocument2 pagesUworld RationalesMelissa Sapp67% (3)
- Literature Review: Effect of Benson's Relaxation Therapy (BRT) On Post Caesarean Section Pain and StressDocument6 pagesLiterature Review: Effect of Benson's Relaxation Therapy (BRT) On Post Caesarean Section Pain and StressLaelannie MagpayoNo ratings yet
- Effects of Fenugreek, Ginger, and Turmeric Supplementation On Human Milk Volume and Nutrient Content in Breastfeeding Mothers: A Randomized Double-Blind Controlled TrialDocument6 pagesEffects of Fenugreek, Ginger, and Turmeric Supplementation On Human Milk Volume and Nutrient Content in Breastfeeding Mothers: A Randomized Double-Blind Controlled TrialKhoirotul HidayahNo ratings yet
- Combination of Pelvic Floor and Abdominal Muscle eDocument5 pagesCombination of Pelvic Floor and Abdominal Muscle eNeha SinghNo ratings yet
- The Gerson Therapy For Those Dying of Cancer: Pilgrims BooksDocument43 pagesThe Gerson Therapy For Those Dying of Cancer: Pilgrims BooksAlmira IKNo ratings yet
- Jurnal PersalinanDocument5 pagesJurnal PersalinanEly GusniartiNo ratings yet
- Terapi 2Document7 pagesTerapi 2emma sitahNo ratings yet
- Patient Focus Population Intervention Compariso N OutcomeDocument3 pagesPatient Focus Population Intervention Compariso N OutcomeDarwin AndalNo ratings yet
- Suppression of Puerperal Lactation Using Jasmine Flowers (Jasminum Sambac)Document4 pagesSuppression of Puerperal Lactation Using Jasmine Flowers (Jasminum Sambac)Iara PachêcoNo ratings yet
- Effect of Acupoint Hot Compress On Postpartum Urinary Retention After Vaginal Delivery A Randomized Clinical TrialDocument13 pagesEffect of Acupoint Hot Compress On Postpartum Urinary Retention After Vaginal Delivery A Randomized Clinical Trial陳瑋毅No ratings yet
- Pengaruh Body Massage Terhadap Tingkat Depresi Ibu Nifas Di Bidan Praktik Mandiri Siyamtiningsih KaranganyarDocument8 pagesPengaruh Body Massage Terhadap Tingkat Depresi Ibu Nifas Di Bidan Praktik Mandiri Siyamtiningsih KaranganyarEnzel LinaNo ratings yet
- Jurnal Internasional MasniDocument11 pagesJurnal Internasional MasniMasni SetiawatiNo ratings yet
- 100 197 1 SM PDFDocument9 pages100 197 1 SM PDFtresna ayu mustikaNo ratings yet
- 1 s2.0 S2214139121000500 MainDocument6 pages1 s2.0 S2214139121000500 MainpfhmakatubacNo ratings yet
- Jurnal PersalinanDocument5 pagesJurnal PersalinanEly GusniartiNo ratings yet
- Circumsision & NursingDocument2 pagesCircumsision & NursingAhmetNo ratings yet
- Jurnal Pijat Efluerage-DikonversiDocument4 pagesJurnal Pijat Efluerage-Dikonversisri lestariNo ratings yet
- Acetaminophen Analgesia in Neonatal Circumcision: The Effect On PainDocument8 pagesAcetaminophen Analgesia in Neonatal Circumcision: The Effect On PainDaud GultomNo ratings yet
- 178-Article Text-478-4-10-20210118Document5 pages178-Article Text-478-4-10-20210118tara apriyaniNo ratings yet
- Therapeutic Breast Massage 2015Document10 pagesTherapeutic Breast Massage 2015Dwi Putri KhayyirahNo ratings yet
- DIT SoniyaMDocument6 pagesDIT SoniyaMBella FebriantiNo ratings yet
- The Influence of Effleurage Massage Techniques in Overcoming Afretpain in The Public Practice of Sulistiawati Pekalongan East LampungDocument5 pagesThe Influence of Effleurage Massage Techniques in Overcoming Afretpain in The Public Practice of Sulistiawati Pekalongan East LampungCentral Asian StudiesNo ratings yet
- Efficacy of Birth Ball Exercises On Labour Pain ManagementDocument7 pagesEfficacy of Birth Ball Exercises On Labour Pain ManagementWenny Indah Purnama Eka SariNo ratings yet
- Effect of Pre-Cesarean Foot Reflexology Massage On Anxiety of Primiparous WomenDocument10 pagesEffect of Pre-Cesarean Foot Reflexology Massage On Anxiety of Primiparous Womenwahyuningsi pakayaNo ratings yet
- JMRH Volume 8 Issue 1 Pages 2033-2040Document8 pagesJMRH Volume 8 Issue 1 Pages 2033-2040TriNo ratings yet
- Obg ResearchDocument15 pagesObg ResearchAGERI PUSHPALATHANo ratings yet
- Pengaruh Hypnobirthing Terhadap Penanggulangan Nyeri Pada Masa Persalinan Di UPT Puskesmas Sukamaju Kab. Luwu Utara Tahun 2020Document10 pagesPengaruh Hypnobirthing Terhadap Penanggulangan Nyeri Pada Masa Persalinan Di UPT Puskesmas Sukamaju Kab. Luwu Utara Tahun 2020nanaNo ratings yet
- Jurnal Pijat EfluerageDocument4 pagesJurnal Pijat Eflueragesri lestariNo ratings yet
- Effect of Combination of Hypnobreastfeeding and Acupressure On Anxiety and Wound Pain in Post-Caesarean MothersDocument8 pagesEffect of Combination of Hypnobreastfeeding and Acupressure On Anxiety and Wound Pain in Post-Caesarean MothersIis MaisarohNo ratings yet
- JurnalDocument12 pagesJurnalasriii riqotulNo ratings yet
- Effect of Single Low Dose Intrathecal Labor Analgesia On Maternal and Fetal OutcomeDocument6 pagesEffect of Single Low Dose Intrathecal Labor Analgesia On Maternal and Fetal OutcomeAnnaNo ratings yet
- Ahmar Metastasis Health JournalDocument6 pagesAhmar Metastasis Health Journalsumita rahayuNo ratings yet
- Farr 2019Document7 pagesFarr 2019Shinta RazakNo ratings yet
- Pengaruh Metode Deep Back Massage Terhadap Nyeri Persalinan Kala I Fase AktifDocument7 pagesPengaruh Metode Deep Back Massage Terhadap Nyeri Persalinan Kala I Fase AktifFaishal Bawor Banyumas CockfightNo ratings yet
- 1216-Article Text-5860-1-10-20221222Document10 pages1216-Article Text-5860-1-10-20221222MdcNo ratings yet
- Effect of Massage and Aromatherapy On Stress and Prolactin Level Among Primiparous Puerperal Mothers in Semarang, Central Java, IndonesiaDocument10 pagesEffect of Massage and Aromatherapy On Stress and Prolactin Level Among Primiparous Puerperal Mothers in Semarang, Central Java, IndonesiaAinun KurniatiNo ratings yet
- 3101 20516 2 PBDocument9 pages3101 20516 2 PBNasita Afriani27No ratings yet
- The Effect of Sacral Massage On Labor Pain and Anxiety A Randomized Controlled TrialDocument23 pagesThe Effect of Sacral Massage On Labor Pain and Anxiety A Randomized Controlled TrialAnonymous DDIQ0jIsV9No ratings yet
- ABM ProtocoloDocument7 pagesABM ProtocoloRetina MaranhaoNo ratings yet
- Opioid Analgesia For Medical Abortion: A Randomized Controlled TrialDocument8 pagesOpioid Analgesia For Medical Abortion: A Randomized Controlled TrialGeos KarNo ratings yet
- Teknik Penaganan NyeriDocument8 pagesTeknik Penaganan NyeriSulis SipinNo ratings yet
- Pemberian Ekstrak Kayu Manis Terhadap Nyeri Luka Perineum Pada Ibu PostpartumDocument9 pagesPemberian Ekstrak Kayu Manis Terhadap Nyeri Luka Perineum Pada Ibu Postpartumristiani jvNo ratings yet
- Olor en PrematurosDocument4 pagesOlor en PrematurosJuan FranciscoNo ratings yet
- Pengaruh Teknik Effleurage Massage Terhadap Nyeri Afterpains Pada Ibu Nifasmultipara Di BPM Wanti Dan BPM Sartika Di Kota Medan Tahun 2020Document10 pagesPengaruh Teknik Effleurage Massage Terhadap Nyeri Afterpains Pada Ibu Nifasmultipara Di BPM Wanti Dan BPM Sartika Di Kota Medan Tahun 2020Dewi aprianiNo ratings yet
- Cupping TherapyDocument8 pagesCupping TherapySaputra Hermawan GabroNo ratings yet
- Pengaruh Aromaterapi Bitter Orange Terhadap Penurunan Tingkat Nyeri Persalinan Kala I Pada Ibu BersalinDocument6 pagesPengaruh Aromaterapi Bitter Orange Terhadap Penurunan Tingkat Nyeri Persalinan Kala I Pada Ibu BersalinAchmad RyandaNo ratings yet
- Tratamento Com Acupuntura Avaliação Da Dor Lombar em GestantesDocument9 pagesTratamento Com Acupuntura Avaliação Da Dor Lombar em GestantesVinicius FukumiNo ratings yet
- Jurnal Uts Retno KurniawatiDocument7 pagesJurnal Uts Retno KurniawatiRetno KurniawatiNo ratings yet
- Pengaruh Pemberian Aromaterapi Lavender Terhadap Pengendalian Nyeri Persalinan Kala I Pada Ibu BersalinDocument8 pagesPengaruh Pemberian Aromaterapi Lavender Terhadap Pengendalian Nyeri Persalinan Kala I Pada Ibu BersalinErza FratamaNo ratings yet
- Ijwh 159062 Effectiveness of Nifedipine in Threatened Preterm Labor A R 061418Document7 pagesIjwh 159062 Effectiveness of Nifedipine in Threatened Preterm Labor A R 061418ferry gunawanNo ratings yet
- Opioid Analgesia For Medical Abortion: A Randomized Controlled TrialDocument8 pagesOpioid Analgesia For Medical Abortion: A Randomized Controlled Trialreza1811No ratings yet
- Effectiveness of Early Exercise Against Uterine inDocument7 pagesEffectiveness of Early Exercise Against Uterine infitri amaliah kasimNo ratings yet
- Effect of Selected Nursing Interventions in The Reduction of After-Pains and Involution of Uterus Among Post-Natal Mothers in Selected HospitalsDocument1 pageEffect of Selected Nursing Interventions in The Reduction of After-Pains and Involution of Uterus Among Post-Natal Mothers in Selected HospitalsArti NegiNo ratings yet
- 104-107 Reeja Mariam PDFDocument4 pages104-107 Reeja Mariam PDFMoh. Arif Sahrani Hi. HarunNo ratings yet
- Pemberian Kompres Hangat Pada Ibu Bersalin Kala I Berpengaruh Terhadap Pengurangan Nyeri Persalinan Di Klinik Bersalin Nirmala MedanDocument10 pagesPemberian Kompres Hangat Pada Ibu Bersalin Kala I Berpengaruh Terhadap Pengurangan Nyeri Persalinan Di Klinik Bersalin Nirmala MedanDeff HaningNo ratings yet
- Yoga ExercisesDocument12 pagesYoga ExercisesMusdalifa Tenri UddaniNo ratings yet
- BiblioDocument6 pagesBiblioJohann Mark BagcalNo ratings yet
- The Effect of GB21 Acupressure On PainDocument5 pagesThe Effect of GB21 Acupressure On PainSiti AisahNo ratings yet
- Pengaruh Pemberian Aromaterapi Lavender Terhadap Pengendalian Nyeri Persalinan Kala I Pada Ibu BersalinDocument8 pagesPengaruh Pemberian Aromaterapi Lavender Terhadap Pengendalian Nyeri Persalinan Kala I Pada Ibu BersalinBagas DwipNo ratings yet
- Holistic Postpartum Manual: Maternal Health Manuals, #3From EverandHolistic Postpartum Manual: Maternal Health Manuals, #3No ratings yet
- P 5Document14 pagesP 5Muh AqwilNo ratings yet
- KPD 2Document9 pagesKPD 2Muh AqwilNo ratings yet
- KPD 1Document12 pagesKPD 1Muh AqwilNo ratings yet
- DiagnosticsDocument14 pagesDiagnosticsMuh AqwilNo ratings yet
- P 4Document8 pagesP 4Muh AqwilNo ratings yet
- Ultrasonographic Prediction of Placental Invasion in Placenta Previa by Placenta Accreta IndexDocument8 pagesUltrasonographic Prediction of Placental Invasion in Placenta Previa by Placenta Accreta IndexMuh AqwilNo ratings yet
- P 3Document12 pagesP 3Muh AqwilNo ratings yet
- Perinatal Outcome in Preterm Premature Rupture of Membranes Before 37 Weeks of GestationDocument6 pagesPerinatal Outcome in Preterm Premature Rupture of Membranes Before 37 Weeks of GestationJathzeel LopezNo ratings yet
- Taiwanese Journal of Obstetrics & Gynecology: Review ArticleDocument11 pagesTaiwanese Journal of Obstetrics & Gynecology: Review ArticleMuh AqwilNo ratings yet
- Back Massage Intervention For Relieving Lower Back Pain in Puerperal Women: A Randomized Control Trial StudyDocument6 pagesBack Massage Intervention For Relieving Lower Back Pain in Puerperal Women: A Randomized Control Trial StudyMuh Aqwil100% (1)
- Application of Extra Virgin Olive Oil To Prevent Nipple Cracking in Lactating WomenDocument6 pagesApplication of Extra Virgin Olive Oil To Prevent Nipple Cracking in Lactating WomenMuh AqwilNo ratings yet
- Jurnal Keputihan 1Document6 pagesJurnal Keputihan 1Muh AqwilNo ratings yet
- Integrative Review of The Factors That in Uence Fathers' Involvement in The Breastfeeding of Their InfantsDocument11 pagesIntegrative Review of The Factors That in Uence Fathers' Involvement in The Breastfeeding of Their InfantsMuh AqwilNo ratings yet
- Jurnal Resti 5Document15 pagesJurnal Resti 5Muh AqwilNo ratings yet
- Jurnal Resti 4Document11 pagesJurnal Resti 4Muh AqwilNo ratings yet
- 3 Prevalence and FactorsDocument8 pages3 Prevalence and FactorsMulumebet EshetuNo ratings yet
- Betelvine (Piper Betle L.) - A Comprehensive Insight Into Its Ethnopharmacology, Phytochemistry, and Pharmacological, Biomedical and Therapeutic AttributesDocument35 pagesBetelvine (Piper Betle L.) - A Comprehensive Insight Into Its Ethnopharmacology, Phytochemistry, and Pharmacological, Biomedical and Therapeutic AttributesMuh AqwilNo ratings yet
- Jurnal Rupture Perineum 2Document9 pagesJurnal Rupture Perineum 2Muh AqwilNo ratings yet
- Jurnal Rupture Perineum 1Document11 pagesJurnal Rupture Perineum 1Muh AqwilNo ratings yet
- Betelvine (Piper Betle L.) - A Comprehensive Insight Into Its Ethnopharmacology, Phytochemistry, and Pharmacological, Biomedical and Therapeutic AttributesDocument37 pagesBetelvine (Piper Betle L.) - A Comprehensive Insight Into Its Ethnopharmacology, Phytochemistry, and Pharmacological, Biomedical and Therapeutic AttributesMuh AqwilNo ratings yet
- Ijstd 42 38Document8 pagesIjstd 42 38Muh AqwilNo ratings yet
- Jurnal Rupture Perineum 3Document6 pagesJurnal Rupture Perineum 3Muh AqwilNo ratings yet
- Jurnal Rupture Perineum 5Document5 pagesJurnal Rupture Perineum 5Muh AqwilNo ratings yet
- EJPS Accepted VersionDocument17 pagesEJPS Accepted VersionMuh AqwilNo ratings yet
- Hirschsprung Disease Beyond Infancy: Casey M. Calkins, MDDocument10 pagesHirschsprung Disease Beyond Infancy: Casey M. Calkins, MDMuh AqwilNo ratings yet
- Anal Trauma JournalDocument8 pagesAnal Trauma JournalMelia Bogari 李梅华No ratings yet
- Valid RRR Application 2013 - 2017 PDFDocument22,467 pagesValid RRR Application 2013 - 2017 PDFAyub NaveedNo ratings yet
- Effect of Human Papilloma Virus in HIV Infected Person: A Mini ReviewDocument7 pagesEffect of Human Papilloma Virus in HIV Infected Person: A Mini ReviewKIH 20162017No ratings yet
- Assessment of PersonalityDocument3 pagesAssessment of PersonalityRahman ButtNo ratings yet
- Neurobic Excersise Impact On Cognative FunctionDocument8 pagesNeurobic Excersise Impact On Cognative FunctionZalinah Mohd YusofNo ratings yet
- KP Astrology Rules of PredictionDocument4 pagesKP Astrology Rules of PredictionRajeshNo ratings yet
- Window Cleaning Safety GuidelineDocument4 pagesWindow Cleaning Safety Guidelinejhunvalencia1203No ratings yet
- Allan ALH105 Week 3Document5 pagesAllan ALH105 Week 3alvin mwizNo ratings yet
- Presentation On PDSDocument14 pagesPresentation On PDSShiva TantiNo ratings yet
- Prevalence of High Risk Pregnancy in Rural DharwadDocument4 pagesPrevalence of High Risk Pregnancy in Rural DharwadIOSRjournalNo ratings yet
- A Handbook of Dementia Care: Edited byDocument15 pagesA Handbook of Dementia Care: Edited byJovana Ognenovska Bakalovska100% (1)
- Tranumpreet Kaur 0064 Letter-Of-AcceptanceDocument3 pagesTranumpreet Kaur 0064 Letter-Of-AcceptanceTranum Kandiara (Tannu)No ratings yet
- Art Comparison Essay ExampleDocument5 pagesArt Comparison Essay Exampleflrzcpaeg100% (2)
- ZR53 MSDSDocument5 pagesZR53 MSDSAnonymous PinM7iNo ratings yet
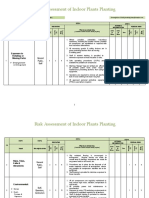
- Risk Assessment of Indoor Plants PlantingDocument5 pagesRisk Assessment of Indoor Plants Plantingطارق رضوانNo ratings yet
- Notes On Critical Areas in Labor Law Part IiDocument66 pagesNotes On Critical Areas in Labor Law Part IipaulNo ratings yet
- Primary Eye Care-A Manual For Health WorkersDocument76 pagesPrimary Eye Care-A Manual For Health WorkersRHU LOOCNo ratings yet
- Direct Black 22Document4 pagesDirect Black 22DHRUVNo ratings yet
- Jawad Et Al - 2021 - Implications of Armed Conflict For Maternal and Child HealthDocument18 pagesJawad Et Al - 2021 - Implications of Armed Conflict For Maternal and Child HealthIvan OliveiraNo ratings yet
- Microbial Limits Tests: The Difference Between "Absence of Objectionable Microorganisms" and "Absence of Specified Microorganisms"Document7 pagesMicrobial Limits Tests: The Difference Between "Absence of Objectionable Microorganisms" and "Absence of Specified Microorganisms"Jai MurugeshNo ratings yet
- Rickets - A Brief View With Homoeopathic ApproachDocument32 pagesRickets - A Brief View With Homoeopathic ApproachDr. Sandeep Anwane100% (1)
- Data Legacy InsuranceCos SourceRSDocument48 pagesData Legacy InsuranceCos SourceRSrishu1527No ratings yet
- PMDC Community Medicine Mcqs PDFDocument280 pagesPMDC Community Medicine Mcqs PDFJay KNo ratings yet
- Cases HBSDocument40 pagesCases HBStoluene_bomb33% (9)
- DodgeballDocument5 pagesDodgeballapi-514548596No ratings yet
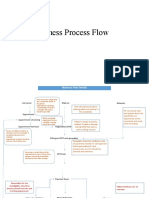
- Business Process FlowDocument12 pagesBusiness Process FlowKumar BalramNo ratings yet
- Levels of PreventionDocument23 pagesLevels of Preventionkuruvagadda sagar100% (1)
- Transdiagnostic TreatmentDocument9 pagesTransdiagnostic Treatmentvalentina chistrugaNo ratings yet
- Muhanga District Development Plan 2013-2018-1 01Document116 pagesMuhanga District Development Plan 2013-2018-1 01Joseph Tuseku Officiel100% (1)