You might also like
- Alternative & Complementary Therapy in LabourDocument14 pagesAlternative & Complementary Therapy in Labourhiral mistry86% (14)
- Alternative-Complementary-Therapy-in-Labour SUBMISSIONDocument18 pagesAlternative-Complementary-Therapy-in-Labour SUBMISSIONSavita HanamsagarNo ratings yet
- Non-Pharmacological Pain Relief Measures for Labor and DeliveryDocument14 pagesNon-Pharmacological Pain Relief Measures for Labor and DeliveryStudent NurseNo ratings yet
- Ward ClassDocument28 pagesWard ClassJah AcabNo ratings yet
- NCM 107 Lesson 10Document6 pagesNCM 107 Lesson 10eirelav0902No ratings yet
- Danger Signs During Labor and Delivery and Pain Relief During ChildbirthDocument4 pagesDanger Signs During Labor and Delivery and Pain Relief During ChildbirthKaye Niale BaleteNo ratings yet
- Alternative AND Complementary Therapies in Labor: Ancy AbrahamDocument54 pagesAlternative AND Complementary Therapies in Labor: Ancy AbrahamAnn Merlin JobinNo ratings yet
- Alternative Therapies in LabourDocument65 pagesAlternative Therapies in Labourhiral mistryNo ratings yet
- Seminar Presentation: Presented By: D.Kaviya Final YearDocument36 pagesSeminar Presentation: Presented By: D.Kaviya Final YearhebzibaNo ratings yet
- Pain During Labour??!!?? Hypno-Birthing Can Handle This!!!!: Share4Document5 pagesPain During Labour??!!?? Hypno-Birthing Can Handle This!!!!: Share4annisaNo ratings yet
- Preparation For Childbirth and ParentingDocument10 pagesPreparation For Childbirth and ParentingRaquel MonsalveNo ratings yet
- FDocument8 pagesFNanda AgustinNo ratings yet
- Labor and Delivery - Study GuideDocument9 pagesLabor and Delivery - Study GuideRara SorayaNo ratings yet
- Pain Management During Labor & Second Stage of LaborDocument97 pagesPain Management During Labor & Second Stage of LaborTheMothershipNo ratings yet
- Bahasa InggrisDocument10 pagesBahasa InggrisauliaNo ratings yet
- REVIEWERDocument3 pagesREVIEWERRazell Jean ArazaNo ratings yet
- Updated NCM 107 Lecture Week 8Document46 pagesUpdated NCM 107 Lecture Week 8Quencee CalaycayNo ratings yet
- CBL 2 Group 1Document26 pagesCBL 2 Group 1Muhammad Jefri LukmanNo ratings yet
- PainDocument3 pagesPainMabesNo ratings yet
- 641 1769 1 PBDocument8 pages641 1769 1 PBHira DamayantiNo ratings yet
- The Effect of Acupressure and Effleurage On Pain Relief in The Active Phase of The First Stage of Labor in The Community Health Center of Kawunganten, Cilacap, IndonesiaDocument7 pagesThe Effect of Acupressure and Effleurage On Pain Relief in The Active Phase of The First Stage of Labor in The Community Health Center of Kawunganten, Cilacap, IndonesiaSyahlu DamayantiiNo ratings yet
- 4 - 2 - 2a Educational Childbirth PreparationDocument44 pages4 - 2 - 2a Educational Childbirth Preparationnery.nerissNo ratings yet
- 582-Article Text-1143-1-10-20211214Document16 pages582-Article Text-1143-1-10-20211214Chatrine MutiaraNo ratings yet
- Health Talk Om Antenatal ExerciseDocument10 pagesHealth Talk Om Antenatal ExerciseDeepika PatidarNo ratings yet
- Unit 4 - Srivarshini SDocument30 pagesUnit 4 - Srivarshini Ssania.mustafa0123No ratings yet
- MODULE 4 - 1st Part INTRAPARTAL CAREDocument15 pagesMODULE 4 - 1st Part INTRAPARTAL CARECaithlyn KirthleyNo ratings yet
- "A Strong Intention, A Relaxed Body and An Open Mind Are The Main Ingredients For An Active Birth" - Janet BalaskasDocument139 pages"A Strong Intention, A Relaxed Body and An Open Mind Are The Main Ingredients For An Active Birth" - Janet BalaskascherenjanaNo ratings yet
- Pain During Labor and Delivery: ExerciseDocument9 pagesPain During Labor and Delivery: ExerciseLhara Vhaneza CuetoNo ratings yet
- m4 MCN - m4Document140 pagesm4 MCN - m4Kristine KimNo ratings yet
- Yoga ExercisesDocument12 pagesYoga ExercisesMusdalifa Tenri UddaniNo ratings yet
- Yoga During Pregnancy Reduces Labor Pain And Shortens DeliveryDocument11 pagesYoga During Pregnancy Reduces Labor Pain And Shortens DeliveryFarhana AbirNo ratings yet
- Pain Management Guide for NursesDocument14 pagesPain Management Guide for NurseskeyonaNo ratings yet
- Penerapan Prosedur Terapi Effleurage Massage Pada Ibu Dengan Ketidaknyamanan Pasca Partum: Literature ReviewDocument5 pagesPenerapan Prosedur Terapi Effleurage Massage Pada Ibu Dengan Ketidaknyamanan Pasca Partum: Literature ReviewNovianda Ghina NANo ratings yet
- Efektivitas Senam Hamil Sebagai Pelayanan Prenatal Dalam Menurunkan Kecemasan Menghadapi Persalinan Pertama-With-Cover-Page-V2Document11 pagesEfektivitas Senam Hamil Sebagai Pelayanan Prenatal Dalam Menurunkan Kecemasan Menghadapi Persalinan Pertama-With-Cover-Page-V2Alfeus NuruNo ratings yet
- PENGARUH PIJAT PERINEUM TERHADAP TINGKAT KECEMASANDocument5 pagesPENGARUH PIJAT PERINEUM TERHADAP TINGKAT KECEMASANsekarwidya putriNo ratings yet
- AIP Chap17 Pain ReliefDocument4 pagesAIP Chap17 Pain ReliefVrunda AppannagariNo ratings yet
- Effect of Therapeutic Massage On Relieving Pregnancy DiscomfortsDocument8 pagesEffect of Therapeutic Massage On Relieving Pregnancy DiscomfortsDerison MarsinovaNo ratings yet
- NHGFFDocument9 pagesNHGFFRingga HerlambangNo ratings yet
- Plimentary and Alternative TherapiesDocument17 pagesPlimentary and Alternative TherapiesVeena DalmeidaNo ratings yet
- Plimentary and Alternative TherapiesDocument17 pagesPlimentary and Alternative TherapiesVeena DalmeidaNo ratings yet
- CAM FinalecDocument62 pagesCAM FinalecmaridelleNo ratings yet
- Antenatal Care Guide for Pregnant WomenDocument6 pagesAntenatal Care Guide for Pregnant WomenRabecca Beluta AmbaritaNo ratings yet
- Pain Relief & Comfort in Labour (Lecture)Document6 pagesPain Relief & Comfort in Labour (Lecture)Akamnoor BrarNo ratings yet
- Sleep Rest Comfort 2013Document80 pagesSleep Rest Comfort 2013Stacy LieutierNo ratings yet
- 2011 Apr 35Document18 pages2011 Apr 35Edogawa RakhmanNo ratings yet
- Non-Pharmacological Pain Relief Methods for ChildbirthDocument7 pagesNon-Pharmacological Pain Relief Methods for ChildbirthMohammad JupriNo ratings yet
- Pain Management Options During ChildbirthDocument9 pagesPain Management Options During ChildbirthSheena Felicia-WillisNo ratings yet
- Efek Metode Non Farmakologik Terhadap Intensitas Nyeri Ibu Bersalin Kala IDocument7 pagesEfek Metode Non Farmakologik Terhadap Intensitas Nyeri Ibu Bersalin Kala IWaluh BejarangNo ratings yet
- Childbirth EducationDocument2 pagesChildbirth EducationJuvy Rose Tinga YeeNo ratings yet
- Rupinder Thesis Final-2Document74 pagesRupinder Thesis Final-2Rupinder GorayaNo ratings yet
- Article Information: Dessyhar Ista@gmail. ComDocument5 pagesArticle Information: Dessyhar Ista@gmail. ComNurul Gita SafitriNo ratings yet
- NCP-PAIN-1Document6 pagesNCP-PAIN-1goodemonz15No ratings yet
- Mrs. Hannah Rajsekhar P. Sumalatha: BackgroundDocument6 pagesMrs. Hannah Rajsekhar P. Sumalatha: BackgroundKinjal SharmaNo ratings yet
- Pregnancy & Birth: Coping With Labor Pain: Epidurals and SpinalsDocument4 pagesPregnancy & Birth: Coping With Labor Pain: Epidurals and SpinalsRichard Deo R. AlaveNo ratings yet
- Abdominal PainDocument3 pagesAbdominal PainReiciel Joy Gombio100% (2)
- Back Pain & Pregnancy: What You Should KnowDocument4 pagesBack Pain & Pregnancy: What You Should KnowGonçalo TrafariaNo ratings yet
- 4 Pain Management, Theories of Labor Onset, Signs of LaborDocument31 pages4 Pain Management, Theories of Labor Onset, Signs of Labormamsh KlangNo ratings yet
- Fetal AssessmentDocument44 pagesFetal AssessmentmariallenNo ratings yet
- Nursing Care Plan HOPE THIS HELPS ALONG THE WAYDocument5 pagesNursing Care Plan HOPE THIS HELPS ALONG THE WAYRye AnchNo ratings yet
- Lore PracticeDocument1 pageLore PracticeAlexis Alyn CanoyNo ratings yet
- AQW FarmingDocument1 pageAQW FarmingAlexis Alyn CanoyNo ratings yet
- NCM103 Medication&hygiene NotesDocument4 pagesNCM103 Medication&hygiene NotesAlexis Alyn CanoyNo ratings yet
- Nursing Pharmacology Ch. 4 Part 2: Seizure Disorders & AnticonvulsantsDocument2 pagesNursing Pharmacology Ch. 4 Part 2: Seizure Disorders & AnticonvulsantsAlexis Alyn CanoyNo ratings yet
- Sept 20 2022 RetdemDocument1 pageSept 20 2022 RetdemAlexis Alyn CanoyNo ratings yet
- Singapore nursing roles and scopesDocument4 pagesSingapore nursing roles and scopesdianaNo ratings yet
- 118 RLE Infection Control PDFDocument15 pages118 RLE Infection Control PDFclaire yowsNo ratings yet
- Form To Be Filled by The Principal Investigator (PI) For Submission To Institutional Ethics Committee (IEC), Shoolini University, SolanDocument5 pagesForm To Be Filled by The Principal Investigator (PI) For Submission To Institutional Ethics Committee (IEC), Shoolini University, Solanv123t456No ratings yet
- Fitness of The Urban Middle Class and Wellness .3Document3 pagesFitness of The Urban Middle Class and Wellness .3iraklije83No ratings yet
- KOMET Study Levetiracetam Vs DepakineDocument4 pagesKOMET Study Levetiracetam Vs DepakineveerrajuNo ratings yet
- Lesson 1.1: Historical Perspectives of Nursing InformaticsDocument33 pagesLesson 1.1: Historical Perspectives of Nursing InformaticsJustine Jean GuillermoNo ratings yet
- Dhikr Therapy For Reducing Anxiety in Cancer PatientDocument6 pagesDhikr Therapy For Reducing Anxiety in Cancer PatientRisfialdo Lily WidiatamaNo ratings yet
- SF8 (Nutritional Status Galupo) AutomatedDocument5 pagesSF8 (Nutritional Status Galupo) AutomatedShen-Chen Cabuyao Dela PuertaNo ratings yet
- Chapter 10 Upper Extremity Interventions PDFDocument208 pagesChapter 10 Upper Extremity Interventions PDFRonny Méndez VasconcellosNo ratings yet
- IV Therapy Article For ExamDocument10 pagesIV Therapy Article For ExamHui HuangNo ratings yet
- Kern Ricular MethodDocument30 pagesKern Ricular MethodPrincy FernandoNo ratings yet
- Hospital Pharmacy Q. P. Code 2863 Chapter 1: Hospital-Its Organization and FunctionsDocument7 pagesHospital Pharmacy Q. P. Code 2863 Chapter 1: Hospital-Its Organization and FunctionsAnoop TandurNo ratings yet
- Simulation-Based Interprofessional Education Guided by Kolb's Experiential Learning TheoryDocument7 pagesSimulation-Based Interprofessional Education Guided by Kolb's Experiential Learning TheoryAi Indah NazriahNo ratings yet
- Principles of Full Mouth RehabilitationDocument7 pagesPrinciples of Full Mouth RehabilitationvarunNo ratings yet
- Interpersonal Relationships - EditedDocument4 pagesInterpersonal Relationships - EditedMAKOKHA BONFACENo ratings yet
- CHOLECYSTECTOMYDocument9 pagesCHOLECYSTECTOMYGuenever Tesoro100% (1)
- Fundamentals of Treatment PlanningDocument310 pagesFundamentals of Treatment PlanningLekic Jelena100% (4)
- A Textbook of General Practice A Textboo PDFDocument343 pagesA Textbook of General Practice A Textboo PDFThierry Uhawenimana100% (3)
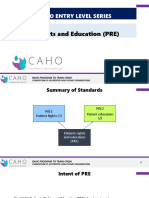
- NABH Series4 PREDocument50 pagesNABH Series4 PREPallavi Deepak DongreNo ratings yet
- Healthcare Quality HandbookDocument7 pagesHealthcare Quality HandbooknomankhanNo ratings yet
- QVASDocument1 pageQVASAnjaswati Farida AdyanaNo ratings yet
- Statement of Purpose HDocument2 pagesStatement of Purpose HSamuel John IyanuoluwaNo ratings yet
- Ug DPD Advising SheetDocument2 pagesUg DPD Advising Sheetapi-251486092No ratings yet
- Fundamentals: From Taylor's Video Guide To Clinical Nursing SkillsDocument8 pagesFundamentals: From Taylor's Video Guide To Clinical Nursing SkillsMary Ann Lumbay PayeNo ratings yet
- Disaster Behavioral Health Response PlanDocument26 pagesDisaster Behavioral Health Response Planapi-438654076No ratings yet
- Case Presentation: Go ToDocument2 pagesCase Presentation: Go ToHafidh KhanNo ratings yet
- Suggestions To Improve The Health SectorDocument5 pagesSuggestions To Improve The Health SectorRana Sami100% (1)
- Cannabis-Induced Psychosis May Lead to SchizophreniaDocument7 pagesCannabis-Induced Psychosis May Lead to SchizophreniaBartolomé Pérez GálvezNo ratings yet
- NTP Referral FormDocument2 pagesNTP Referral FormCarl RamosNo ratings yet
- BP405T Sessional Question Paper-4th Sem.B.PharmDocument2 pagesBP405T Sessional Question Paper-4th Sem.B.PharmSajid khanNo ratings yet