You might also like
- Assignment 9Document2 pagesAssignment 9Nuo XuNo ratings yet
- Non-Isothermal Reactor DesignDocument5 pagesNon-Isothermal Reactor Designnorpius7754No ratings yet
- KPO COKE OVEN PHASE-1 LT CABLE SIZING CALCULATION-BPP AREADocument12 pagesKPO COKE OVEN PHASE-1 LT CABLE SIZING CALCULATION-BPP AREAmustangNo ratings yet
- Physics Y1 ReviewDocument5 pagesPhysics Y1 ReviewRakeem McFarlaneNo ratings yet
- Test restDocument2 pagesTest restf7qzztkkksNo ratings yet
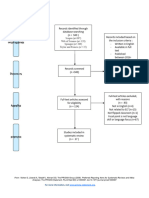
- 2.1.3_-_PRISMA_2009_Flow_Diagram_FillableDocument1 page2.1.3_-_PRISMA_2009_Flow_Diagram_FillablenisasharomNo ratings yet
- Linearity BrochureDocument8 pagesLinearity Brochuremurpy91No ratings yet
- Hoja de Daros Lab9-1Document2 pagesHoja de Daros Lab9-1Angel DikekNo ratings yet
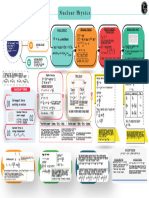
- Nuclear Physics - Mind Map - Lakshya NEET 2024Document1 pageNuclear Physics - Mind Map - Lakshya NEET 2024aanyakaurchonaNo ratings yet
- Acc-406 NoteDocument1 pageAcc-406 Notehanhvy04No ratings yet
- CHEMICAL KINETICS: KEY CONCEPTSDocument1 pageCHEMICAL KINETICS: KEY CONCEPTSeliyachrisNo ratings yet
- Est FormulasDocument15 pagesEst FormulasAira GarciaNo ratings yet
- Pet2Aryf: TransmittedDocument5 pagesPet2Aryf: TransmittedMatthew ListroNo ratings yet
- Assignment 4Document19 pagesAssignment 4Radhe JhaNo ratings yet
- VectorDocument17 pagesVectorPrisha ShailyNo ratings yet
- Scale 1491: "Mela Namanarayani": Also Known As: Raga Narmada, Pratapa, Harsh Major-MinorDocument1 pageScale 1491: "Mela Namanarayani": Also Known As: Raga Narmada, Pratapa, Harsh Major-MinorIan RingNo ratings yet
- Upd C11 Phy EngDocument23 pagesUpd C11 Phy EngArinjoy Mervyn GomesNo ratings yet
- Relation Between Voltage and Output Speed of A DC Motor-1Document8 pagesRelation Between Voltage and Output Speed of A DC Motor-1Abdul RehmanNo ratings yet
- Gaddam, Ikshwak: ResultDocument1 pageGaddam, Ikshwak: Resultpraveen kumarNo ratings yet
- STR DEX CON INT WIS CHA: Operative LVL: 3 Human OutlawDocument3 pagesSTR DEX CON INT WIS CHA: Operative LVL: 3 Human OutlawFacundo GomezNo ratings yet
- Nuclei - Mind Maps - Yakeen 2.0 2024 (Legend)Document1 pageNuclei - Mind Maps - Yakeen 2.0 2024 (Legend)npmishra9818No ratings yet
- Lecture 8 - Chemical Energy and Equilibria IIDocument2 pagesLecture 8 - Chemical Energy and Equilibria IIRaphi S.No ratings yet
- Metodos IntegralesDocument31 pagesMetodos IntegralesJosé Arturo FerreraNo ratings yet
- The Algebra of Block PermutationsDocument1 pageThe Algebra of Block PermutationsM. TanveerNo ratings yet
- 2017-2018 Actors - in - World - Politics - 181217 PDFDocument72 pages2017-2018 Actors - in - World - Politics - 181217 PDFFrancesco RagazziNo ratings yet
- Ac History Matrix - Year 8 Ferris 2017Document1 pageAc History Matrix - Year 8 Ferris 2017api-263403037No ratings yet
- Lund Emily Boyd f17Document4 pagesLund Emily Boyd f17api-456588986No ratings yet
- DC Motors FormulasDocument3 pagesDC Motors FormulasSaabierah SalieNo ratings yet
- Hybrid Blade Element and Lifting Line For Propeller or Propfan PerformanceDocument11 pagesHybrid Blade Element and Lifting Line For Propeller or Propfan PerformancewharNo ratings yet
- 胡 線代 3Document1 page胡 線代 3ljiezhi90No ratings yet
- FIN 703 Learning Curves Lecture Examples Widget Manufacturers (Pty) LimitedDocument1 pageFIN 703 Learning Curves Lecture Examples Widget Manufacturers (Pty) LimitedOfentse MekwaNo ratings yet
- L16, L17, L18 RL, RC, RLC & Parallel CircuitDocument20 pagesL16, L17, L18 RL, RC, RLC & Parallel CircuitdhruvNo ratings yet
- Chemical Kinetics Class - 7 (Notes)Document26 pagesChemical Kinetics Class - 7 (Notes)ᴜsʜɴᴇᴇᴋNo ratings yet
- DissertationDocument1 pageDissertationManar AbdulrahmanNo ratings yet
- CFA Level II Formula Sheet CFA Level II Formula Sheet: Finance (Harvard University) Finance (Harvard University)Document5 pagesCFA Level II Formula Sheet CFA Level II Formula Sheet: Finance (Harvard University) Finance (Harvard University)smith100% (1)
- Cheat SheetDocument1 pageCheat SheetFrancis TanNo ratings yet
- Remaining ProblemsDocument4 pagesRemaining ProblemsKyokyo TokimiNo ratings yet
- Assignment 2 SolutionsDocument13 pagesAssignment 2 SolutionsP34Akshay ChoudharyNo ratings yet
- Lecture01Document7 pagesLecture01guanlin HeNo ratings yet
- Ln3.Fm# - Fcoulomb 4Tfeo&Z: BalmerDocument3 pagesLn3.Fm# - Fcoulomb 4Tfeo&Z: BalmerJayNo ratings yet
- MathDocument3 pagesMathpia guiretNo ratings yet
- Project Management Professional PMP FormulasDocument4 pagesProject Management Professional PMP FormulassachingandhiNo ratings yet
- Protection Settings For 11Kv Bus TieDocument5 pagesProtection Settings For 11Kv Bus Tiemarcelo_santNo ratings yet
- Active Components Part 1Document3 pagesActive Components Part 1Dhiraj PatilNo ratings yet
- Example A Language Report Appendix BDocument5 pagesExample A Language Report Appendix BJershon YongNo ratings yet
- Group Activity - AssignmentDocument1 pageGroup Activity - AssignmentkarmaudeNo ratings yet
- Analysis of voltage and current values over timeDocument1 pageAnalysis of voltage and current values over timeEdward Llanqui RodriguesNo ratings yet
- VolteDocument1 pageVoltemohamed100% (1)
- (Charge RL Avec L 0.1) : Vs FFDocument1 page(Charge RL Avec L 0.1) : Vs FFDiaa Eddine BoudiafNo ratings yet
- AtomsDocument1 pageAtomsmathrooparamNo ratings yet
- Variable MSA 4th Edition Blank TemplateDocument1 pageVariable MSA 4th Edition Blank TemplateSachin RamdurgNo ratings yet
- 400+ Excel Formulas List - Excel Shortcut Keys PDF - Download Here - FilesDocument73 pages400+ Excel Formulas List - Excel Shortcut Keys PDF - Download Here - FilesNoor Ahmad NooriNo ratings yet
- Introduction to Linear Regression AnalysisDocument3 pagesIntroduction to Linear Regression AnalysisDarlene CorderoNo ratings yet
- Extended functions manual for VARMECA 30 variable speed driveDocument108 pagesExtended functions manual for VARMECA 30 variable speed driveCsaba VargaNo ratings yet
- P2 CapacitorDocument1 pageP2 CapacitorAadya BajpaiNo ratings yet
- EST formulas audio power modulation noiseDocument15 pagesEST formulas audio power modulation noiseJNo ratings yet
- Feketes Course NotesDocument192 pagesFeketes Course NotesketatniNo ratings yet
- SANAD II ValproateDocument12 pagesSANAD II ValproateveerrajuNo ratings yet
- Neurologic Differential Diagnosis - A Case-Based Approach (PDFDrive)Document1,678 pagesNeurologic Differential Diagnosis - A Case-Based Approach (PDFDrive)veerrajuNo ratings yet
- Pediatric Concussion Clinical Practice Guidelines (CDC, 2018) PDFDocument1 pagePediatric Concussion Clinical Practice Guidelines (CDC, 2018) PDFveerrajuNo ratings yet
- Research Paper: NeuropsychiatryDocument11 pagesResearch Paper: NeuropsychiatryveerrajuNo ratings yet
- Neurology Clinical Practice Guidelines 2018 Midyear Review PDFDocument14 pagesNeurology Clinical Practice Guidelines 2018 Midyear Review PDFveerrajuNo ratings yet
- Disorders of Consciousness Clinical Practice Guidelines (2018) PDFDocument2 pagesDisorders of Consciousness Clinical Practice Guidelines (2018) PDFveerrajuNo ratings yet
- Pediatric Traumatic Brain Injury Guidelines 2019 PDFDocument2 pagesPediatric Traumatic Brain Injury Guidelines 2019 PDFveerrajuNo ratings yet
- CNS Leukemia Treatment Clinical Practice Guidelines (2018) PDFDocument2 pagesCNS Leukemia Treatment Clinical Practice Guidelines (2018) PDFveerrajuNo ratings yet
- Progressive Ataxia Guidelines 2019 PDFDocument4 pagesProgressive Ataxia Guidelines 2019 PDFveerrajuNo ratings yet
- Atrial Fibrillation Clinical Practice Guidelines (2019) PDFDocument3 pagesAtrial Fibrillation Clinical Practice Guidelines (2019) PDFveerrajuNo ratings yet
- Optimal Use of Polymyxin Antibiotics Clinical Practice Guidelines (2019) PDFDocument3 pagesOptimal Use of Polymyxin Antibiotics Clinical Practice Guidelines (2019) PDFveerrajuNo ratings yet
- Neuropsychiatric Symptoms of Huntington's Disease Clinical Practice Guidelines (2019) PDFDocument2 pagesNeuropsychiatric Symptoms of Huntington's Disease Clinical Practice Guidelines (2019) PDFveerrajuNo ratings yet
- Internal Medicine Clinical Practice Guidelines 2018 Midyear Review PDFDocument17 pagesInternal Medicine Clinical Practice Guidelines 2018 Midyear Review PDFveerrajuNo ratings yet
- Neurocysticercosis Clinical Practice Guidelines (2018) PDFDocument2 pagesNeurocysticercosis Clinical Practice Guidelines (2018) PDFveerrajuNo ratings yet
- Care of Adult Patients in The ICU Clinical Practice Guidelines (2018) PDFDocument2 pagesCare of Adult Patients in The ICU Clinical Practice Guidelines (2018) PDFveerrajuNo ratings yet
- Ketamine Infusions For Chronic Pain Clinical Practice Guidelines (2018) PDFDocument2 pagesKetamine Infusions For Chronic Pain Clinical Practice Guidelines (2018) PDFveerrajuNo ratings yet
- Palliative Care Clinical Practice Guidelines (2018) PDFDocument3 pagesPalliative Care Clinical Practice Guidelines (2018) PDFveerrajuNo ratings yet
- Management of Common Infections With Antimicrobials Guidance Clinical Practice Guidelines (2019) PDFDocument4 pagesManagement of Common Infections With Antimicrobials Guidance Clinical Practice Guidelines (2019) PDFveerrajuNo ratings yet
- Multiple Sclerosis Clinical Practice Guidelines (2018) PDFDocument2 pagesMultiple Sclerosis Clinical Practice Guidelines (2018) PDFveerrajuNo ratings yet
- Mechanical Thromboctomy in Acute Ischemic Stroke Guidelines 2019 PDFDocument1 pageMechanical Thromboctomy in Acute Ischemic Stroke Guidelines 2019 PDFveerrajuNo ratings yet
- Migraine Treatment Guidelines (2019) PDFDocument2 pagesMigraine Treatment Guidelines (2019) PDFveerrajuNo ratings yet
- Alzheimer's Disease Clinical Practice Guidelines (2018)Document1 pageAlzheimer's Disease Clinical Practice Guidelines (2018)veerrajuNo ratings yet
- ComaDocument13 pagesComaMamoon J. MehdiNo ratings yet
- Placental AbnormalitiesDocument3 pagesPlacental AbnormalitiesThakoon TtsNo ratings yet
- Management of Multiple PregnancyDocument17 pagesManagement of Multiple Pregnancyapi-3705046100% (1)
- ResearchDocument6 pagesResearchhaerul ikhsanNo ratings yet
- Guidelines For Multiple Choice Questions MCQ S 4426Document19 pagesGuidelines For Multiple Choice Questions MCQ S 4426R RatheeshNo ratings yet
- (Helveston) Surgical Management of StrabismusDocument518 pages(Helveston) Surgical Management of StrabismusMarianaNo ratings yet
- File - 20190927 - 153306 - Drugs Reaction 2019Document410 pagesFile - 20190927 - 153306 - Drugs Reaction 2019ntnquynhpro100% (1)
- OCD Children AdolescentsDocument8 pagesOCD Children AdolescentsCésar CorveraNo ratings yet
- Upper Midline CorrectionDocument5 pagesUpper Midline CorrectionmutansNo ratings yet
- International Ayurvedic Medical Journal explores Madhuyashti and yogaDocument7 pagesInternational Ayurvedic Medical Journal explores Madhuyashti and yogaVatsas JoshiNo ratings yet
- Diacan Pro BBRAUNDocument4 pagesDiacan Pro BBRAUNJairo AlvaradoNo ratings yet
- Drug StudyDocument7 pagesDrug StudyLA GomezNo ratings yet
- Oncology Work Plan For Students 2022-2023Document34 pagesOncology Work Plan For Students 2022-2023Ahmed SaeedNo ratings yet
- 1 Dental Caries PDFDocument38 pages1 Dental Caries PDFmayang putriNo ratings yet
- GENES ROLE IN CVD (Genomics)Document4 pagesGENES ROLE IN CVD (Genomics)bashirkinza679No ratings yet
- NonCytotoxic Dibenzyl and Also Difluoroborate Capmatinibxlsxoid Fluorophores Permit Visual Image Involving Nucleus or Even Cytoplasm Inside Bioimagingixvwj PDFDocument1 pageNonCytotoxic Dibenzyl and Also Difluoroborate Capmatinibxlsxoid Fluorophores Permit Visual Image Involving Nucleus or Even Cytoplasm Inside Bioimagingixvwj PDFtubweed4No ratings yet
- Old Canalicular Laceration Repair A Retrospective Study ofDocument6 pagesOld Canalicular Laceration Repair A Retrospective Study ofMuh Syarifullah ANo ratings yet
- Treatment of Vaginitis and Vulvitis PDFDocument3 pagesTreatment of Vaginitis and Vulvitis PDFrendyNo ratings yet
- BSC (Hons) HNDDocument2 pagesBSC (Hons) HNDAli AzanNo ratings yet
- NCM106-Cellular Aberrations-Module1-Lesson 4Document10 pagesNCM106-Cellular Aberrations-Module1-Lesson 4Esmareldah Henry SirueNo ratings yet
- Preventing Anemia in AdolescentsDocument7 pagesPreventing Anemia in AdolescentsSagiraju SrinuNo ratings yet
- COVID 19 Ayurveda Project Concept Paper DR Palitha SerasingheDocument8 pagesCOVID 19 Ayurveda Project Concept Paper DR Palitha SerasingheRajeshwari JadhavNo ratings yet
- Nature of Drug AbuseDocument2 pagesNature of Drug AbuseColin GosbertNo ratings yet
- Scedosporium Apiospermum Keratomycosis in A DogDocument4 pagesScedosporium Apiospermum Keratomycosis in A DogDavid Argüelles AndradeNo ratings yet
- Enfermedades Proyecto InglesDocument3 pagesEnfermedades Proyecto Inglesyanis7116No ratings yet
- Cholesteatoma ExplainedDocument28 pagesCholesteatoma ExplainedazadutNo ratings yet
- Morse Fall Scale AssessmentDocument5 pagesMorse Fall Scale AssessmentQueen ShNo ratings yet
- Fenotipos de BronquiolitisDocument14 pagesFenotipos de BronquiolitisJohann MuñozNo ratings yet
- ABG BASICS YvonneDocument48 pagesABG BASICS Yvonneนีล ไบรอันNo ratings yet
- Epidemiology, Risk Factors, Pathogenesis, and Natural History of Thoracic Aortic AneurysmDocument5 pagesEpidemiology, Risk Factors, Pathogenesis, and Natural History of Thoracic Aortic AneurysmNathaliazuosNo ratings yet