You might also like
- Anatomy: Veins of The Forearm and Arteries of The Arm.Document36 pagesAnatomy: Veins of The Forearm and Arteries of The Arm.Mercy AdeolaNo ratings yet
- Vessels and Nerves of The Upper Limb: Petr Hájek, MD., PHDDocument43 pagesVessels and Nerves of The Upper Limb: Petr Hájek, MD., PHDTodesengelNo ratings yet
- Vascolarizzazione e Innervazione ArtiDocument11 pagesVascolarizzazione e Innervazione Artiwv4vwhrkpsNo ratings yet
- 14802upper Limb Blood Vessels and LymphaticsDocument21 pages14802upper Limb Blood Vessels and LymphaticsZiad AlaaNo ratings yet
- Blood Vessels of Upper LimbDocument23 pagesBlood Vessels of Upper Limbkhalid_shinasNo ratings yet
- Blood Supply of Upper LimbDocument35 pagesBlood Supply of Upper LimbfdjkvfjvNo ratings yet
- A1lqh xp5flDocument5 pagesA1lqh xp5flblaze zimbaNo ratings yet
- AXILLADocument5 pagesAXILLAfxbukenyaNo ratings yet
- 6.blood Supply of Upper LimbDocument52 pages6.blood Supply of Upper LimbBlessed LoveNo ratings yet
- Arterii Taza I Konechnostey - Ru.enDocument26 pagesArterii Taza I Konechnostey - Ru.enVishal YadavNo ratings yet
- Human Anatomy & Physiology I - Skeletal System 1 Blood Supply to Upper LimbDocument11 pagesHuman Anatomy & Physiology I - Skeletal System 1 Blood Supply to Upper LimbJing Min ChuaNo ratings yet
- Vascularization of Lower and Upper ExtermitesDocument40 pagesVascularization of Lower and Upper Extermiteszainab sawan100% (1)
- SGDDocument7 pagesSGDJanine Vega Calayo100% (1)
- Ana 201 (Axilla N Axillary Artery) - 1Document119 pagesAna 201 (Axilla N Axillary Artery) - 1Favour OnyeaboNo ratings yet
- ANA L8 - Blood Vessels and Lymphatics of Upper LimbDocument55 pagesANA L8 - Blood Vessels and Lymphatics of Upper LimbjexshimadaNo ratings yet
- UL4-armDocument26 pagesUL4-armfaraNo ratings yet
- Document 3Document1 pageDocument 3bomevah614No ratings yet
- Vascular Supply To Upper ExtremityDocument36 pagesVascular Supply To Upper ExtremityFrancis ChegeNo ratings yet
- Axilla Boundaries and ContentDocument47 pagesAxilla Boundaries and Contentchzaheer72No ratings yet
- Anatomy, Shoulder and Upper Limb, Veins - StatPearls - NCBI BookshelfDocument7 pagesAnatomy, Shoulder and Upper Limb, Veins - StatPearls - NCBI BookshelfIsna SalisNo ratings yet
- Cephalic Vein AnatomyDocument25 pagesCephalic Vein AnatomysquidblitzNo ratings yet
- Anterior Compartment of the ArmDocument46 pagesAnterior Compartment of the ArmAuza Moses IbrahimNo ratings yet
- Blood Supply of Upper LimbDocument36 pagesBlood Supply of Upper Limbteklay100% (2)
- Arteries & Veins of The Upper LimbDocument4 pagesArteries & Veins of The Upper LimbPirabakar MahendranNo ratings yet
- The Axilla: Shah Hussain LECTURER (Surgical)Document81 pagesThe Axilla: Shah Hussain LECTURER (Surgical)Ibrar KhanNo ratings yet
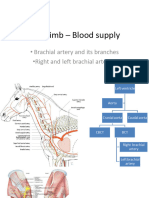
- Fore Limb - Blood SupplyDocument20 pagesFore Limb - Blood SupplyVignesh rajuNo ratings yet
- Subclavian Artery: Related TermsDocument16 pagesSubclavian Artery: Related Termsbella friscaamaliaNo ratings yet
- Anatomy 1Document82 pagesAnatomy 1innyNo ratings yet
- Blood Supply and Nerve Supply of Upper LimbDocument94 pagesBlood Supply and Nerve Supply of Upper LimbthrrishaNo ratings yet
- Brachial Plexus (Compatibility Mode)Document58 pagesBrachial Plexus (Compatibility Mode)Daniel OkakaNo ratings yet
- Axillary ArteryDocument28 pagesAxillary Arteryshrishti shadangiNo ratings yet
- Anatomy of the Upper Limb Vasculature and NervesDocument12 pagesAnatomy of the Upper Limb Vasculature and NervesJasonLiewNo ratings yet
- Lecture 9 Clinical and Functional Anatomy of The VeinsDocument7 pagesLecture 9 Clinical and Functional Anatomy of The Veinssomebody_maNo ratings yet
- Discussion Topics IA1 AnatDocument9 pagesDiscussion Topics IA1 AnatPhysics TutionNo ratings yet
- Arm anatomy and structuresDocument16 pagesArm anatomy and structuresFirst LuckNo ratings yet
- Anorectal Anatomy & Surgical ManagementDocument164 pagesAnorectal Anatomy & Surgical Managementsgod34No ratings yet
- KUMC 18 Vascular Supply To UE StudentDocument36 pagesKUMC 18 Vascular Supply To UE StudentAzwarmuslimHasballahAminNo ratings yet
- Aorta AnatomyDocument41 pagesAorta AnatomySingey LhendupNo ratings yet
- Understanding Peripheral Vascular SystemDocument5 pagesUnderstanding Peripheral Vascular SystemJi CaratNo ratings yet
- Brachial PlexusDocument98 pagesBrachial PlexussandeepNo ratings yet
- DR/ Abd Allah Nazeer. MD.: Radiological Vascular Anatomy of The Upper and Lower LimbsDocument80 pagesDR/ Abd Allah Nazeer. MD.: Radiological Vascular Anatomy of The Upper and Lower LimbsAndra HijratulNo ratings yet
- Membrul Superior MGDocument118 pagesMembrul Superior MGMihai OpreaNo ratings yet
- Operative Surgery and Clinical Anatomy of the Upper and Lower LimbsDocument122 pagesOperative Surgery and Clinical Anatomy of the Upper and Lower LimbsHamidreza RahmaniNo ratings yet
- Rib Anatomy and Extra TuberosityDocument6 pagesRib Anatomy and Extra TuberositylightwhisperNo ratings yet
- Inferior Vena Cava. Portal VeinDocument10 pagesInferior Vena Cava. Portal Veinsangesh kNo ratings yet
- Forearm Note DR SharewDocument8 pagesForearm Note DR SharewsharewdelelegnNo ratings yet
- Human Anatomy Lecture on Peripheral Circulation and StructuresDocument45 pagesHuman Anatomy Lecture on Peripheral Circulation and StructuresPhilip GituriNo ratings yet
- Blood Vessels of Thoracic WallDocument9 pagesBlood Vessels of Thoracic WallShimmering MoonNo ratings yet
- Lower Limb ReviewDocument24 pagesLower Limb ReviewRyan SilberNo ratings yet
- Upper Limb Lecture 1Document45 pagesUpper Limb Lecture 1RAHMADANI SAFITRINo ratings yet
- Axila: Mesole Samuel Bolaji (B.SC M.SC PHD (In-View) ) Course: Anatomy Course Code: Han 3010Document15 pagesAxila: Mesole Samuel Bolaji (B.SC M.SC PHD (In-View) ) Course: Anatomy Course Code: Han 3010Tinotenda KarumeNo ratings yet
- Pelvic organs blood vessels, lymphatic drainage and innervationDocument8 pagesPelvic organs blood vessels, lymphatic drainage and innervationclear mindNo ratings yet
- Upper Limb Lecture 1Document45 pagesUpper Limb Lecture 1KhurshidbuyamayumNo ratings yet
- Muscles and Arteries of the Upper LimbDocument45 pagesMuscles and Arteries of the Upper LimbfdjkvfjvNo ratings yet
- Topography of The Upper Limb: Dr. Muh. Iqbal Basri, M.Kes, SP.SDocument53 pagesTopography of The Upper Limb: Dr. Muh. Iqbal Basri, M.Kes, SP.SFiraNo ratings yet
- Axillary Artery Formation and RelationsDocument16 pagesAxillary Artery Formation and RelationsHarsha MudigoudaNo ratings yet
- 2008 Venous and Lymphatic SystemsDocument63 pages2008 Venous and Lymphatic Systemsprasun_vNo ratings yet
- Physical Ass 2Document5 pagesPhysical Ass 2andreabreeNo ratings yet
- TOXICOLOGY MCQsDocument9 pagesTOXICOLOGY MCQsSanjiv Sharma100% (1)
- Mtap421 ElectrolytesDocument9 pagesMtap421 ElectrolytesNhelomar ManlinconNo ratings yet
- Anatomy Mnemonics 2Document50 pagesAnatomy Mnemonics 2Nourhan JamalNo ratings yet
- 4 Valvular Heart Disease#36f7Document40 pages4 Valvular Heart Disease#36f7Natasha LiberisNo ratings yet
- ACS Algorithm SymptomsDocument1 pageACS Algorithm SymptomsJhon100% (1)
- PFT: Assess Lung Function With Pulmonary Function TestsDocument62 pagesPFT: Assess Lung Function With Pulmonary Function TestsWiz SamNo ratings yet
- Cardiac PhysiologyDocument102 pagesCardiac PhysiologyPeter Larsen100% (1)
- Pocket Card - IV Fluids - September 2021Document6 pagesPocket Card - IV Fluids - September 2021NeweeJoonYowNo ratings yet
- Epidemiological Study Designs MHRDocument94 pagesEpidemiological Study Designs MHRaaminah tariqNo ratings yet
- 1167 1864 1 SMDocument5 pages1167 1864 1 SMMujahid FajrulNo ratings yet
- Surgery Notes SummaryDocument39 pagesSurgery Notes SummaryNishok VSNo ratings yet
- AIIMS NORCET 2021 Shift 1 Memory Based Paper EnglishDocument12 pagesAIIMS NORCET 2021 Shift 1 Memory Based Paper EnglishMata BharatNo ratings yet
- Betarie Anum Almira - RMIK (A) - Praktik KSPK 11Document1 pageBetarie Anum Almira - RMIK (A) - Praktik KSPK 11Betarie Anum AlmiraNo ratings yet
- Sticky Notes Tips Houseman Compilation 389259Document66 pagesSticky Notes Tips Houseman Compilation 389259MuhdZaeed100% (3)
- Drugs For GoutDocument29 pagesDrugs For GoutSsempijja Joshua BuyinzaNo ratings yet
- Nursing Care for a Patient with Acute Myocardial Infarction (AMIDocument11 pagesNursing Care for a Patient with Acute Myocardial Infarction (AMISheda BondNo ratings yet
- (Intravenous Fluids) : Cellular Fluid CompartmentsDocument17 pages(Intravenous Fluids) : Cellular Fluid CompartmentsFatimaNo ratings yet
- Cpliver 1Document4 pagesCpliver 1isahNo ratings yet
- Diabetic Ketoacidosis (DKA) VS. Hyperosmolar Hyperglycemic Syndrome (HHS)Document5 pagesDiabetic Ketoacidosis (DKA) VS. Hyperosmolar Hyperglycemic Syndrome (HHS)MrRightNo ratings yet
- Esrd Ppt. - Alex (Final)Document109 pagesEsrd Ppt. - Alex (Final)Shoixi ⎝⓿⏝⓿⎠No ratings yet
- Antihypertensive Treatments and COVID-19 MortalityDocument9 pagesAntihypertensive Treatments and COVID-19 MortalityDeny Dwi HartantoNo ratings yet
- Pre EclampsiaDocument2 pagesPre EclampsiaDIVINA VINCEE PRESTONo ratings yet
- Gas Exchange Transport and CirculationDocument34 pagesGas Exchange Transport and CirculationRaineir PabiranNo ratings yet
- Staff Training PowerpointDocument12 pagesStaff Training Powerpointapi-282305740No ratings yet
- GERD Gastroesophageal Reflux Disease NCLEX ReviewDocument12 pagesGERD Gastroesophageal Reflux Disease NCLEX ReviewBianca Trish ManlangitNo ratings yet
- DAFTAR PUSTAKA Fix BGTDocument3 pagesDAFTAR PUSTAKA Fix BGTfitrianiNo ratings yet
- 8 - Chronic Kidney Disease Clinical Pathway - Final - Nov.20.2014Document56 pages8 - Chronic Kidney Disease Clinical Pathway - Final - Nov.20.2014As RifahNo ratings yet
- Blank 10Document4 pagesBlank 10Pari SharmaNo ratings yet
- Baking Soda - True Enemy of The Pharmaceutical Industry WoDocument6 pagesBaking Soda - True Enemy of The Pharmaceutical Industry WoAlex VallzNo ratings yet