You might also like
- Your 2024 Social Security Cost of Living IncreaseDocument4 pagesYour 2024 Social Security Cost of Living IncreasenazoyaqNo ratings yet
- SANDOVAL 8030228962 Loan EstimateDocument3 pagesSANDOVAL 8030228962 Loan EstimateRic PerezNo ratings yet
- Eligibility Results NoticeDocument11 pagesEligibility Results NoticeAlex LawroskyNo ratings yet
- View Notice ServletDocument4 pagesView Notice ServletDianca MaxeyNo ratings yet
- Notice of Case Action: Food AssistanceDocument4 pagesNotice of Case Action: Food AssistanceWill ShawNo ratings yet
- OMB Control No. 2900-0086 Respondent Burden: 15 MinutesDocument2 pagesOMB Control No. 2900-0086 Respondent Burden: 15 MinutesPatrickCharlesNo ratings yet
- Central Aspen Scanning Area P.O. BOX 830 Bernalillo NM 87004 January 30, 2021Document4 pagesCentral Aspen Scanning Area P.O. BOX 830 Bernalillo NM 87004 January 30, 2021Wilma HubbardNo ratings yet
- Immunization Record FormDocument4 pagesImmunization Record FormLeonardo Zikri ArmandaNo ratings yet
- Federal Direct Stafford/Ford Loan Federal Direct Unsubsidized Stafford/Ford Loan Master Promissory Note William D. Ford Federal Direct Loan ProgramDocument10 pagesFederal Direct Stafford/Ford Loan Federal Direct Unsubsidized Stafford/Ford Loan Master Promissory Note William D. Ford Federal Direct Loan ProgramLoriNo ratings yet
- MPN8 18 2010Document8 pagesMPN8 18 2010minieldridgeNo ratings yet
- Postpaid Monthly Statement: This Month's SummaryDocument4 pagesPostpaid Monthly Statement: This Month's SummaryAzure DevOpsNo ratings yet
- Important Information About Your Unemployment Insurance ClaimDocument3 pagesImportant Information About Your Unemployment Insurance ClaimSolomonNo ratings yet
- Generate-Params HKS6/42whICe/ioG99BR/NHOzO3Df 4vYi19pvCHT0fJ0Xx46GcW89vPhHXXJm73KXSQCEYz PDFDocument27 pagesGenerate-Params HKS6/42whICe/ioG99BR/NHOzO3Df 4vYi19pvCHT0fJ0Xx46GcW89vPhHXXJm73KXSQCEYz PDFJohn AustinNo ratings yet
- LTC Renewal PDFDocument12 pagesLTC Renewal PDFVashisth SoniNo ratings yet
- 34 Wihh 504331 H 0714320240524151104202Document3 pages34 Wihh 504331 H 0714320240524151104202jamelmhunt22No ratings yet
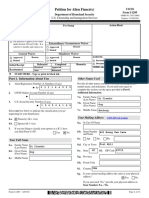
- Petition For Alien Fiancé (E) : Uscis Form I-129FDocument13 pagesPetition For Alien Fiancé (E) : Uscis Form I-129FеленаNo ratings yet
- Norma 2021Document13 pagesNorma 2021Norma MichelNo ratings yet
- Base Builder - New Hire PaperworkDocument10 pagesBase Builder - New Hire Paperworkelhard shalloNo ratings yet
- Credit ApplicationDocument3 pagesCredit Applicationenergizr96No ratings yet
- Changed Circumstance Detail Form: Melissa Marie JonesDocument11 pagesChanged Circumstance Detail Form: Melissa Marie JonesMelissa JonesNo ratings yet
- Affidavit of Support: Part 1. Information About YouDocument8 pagesAffidavit of Support: Part 1. Information About YouPopescu GeorgeNo ratings yet
- Notice 10379458091 PDFDocument9 pagesNotice 10379458091 PDFRenee VasquezNo ratings yet
- Notice of Case Action: Medicaid For Unborn BabiesDocument6 pagesNotice of Case Action: Medicaid For Unborn Babiestb99bwk5cqNo ratings yet
- Personal Loan Application Form Borang Permohonan Pinjaman PeribadiDocument6 pagesPersonal Loan Application Form Borang Permohonan Pinjaman PeribadiMohd AzhariNo ratings yet
- 1481546265426Document3 pages1481546265426api-370784582No ratings yet
- Compass Application 2.14Document11 pagesCompass Application 2.14Matthew SweeneyNo ratings yet
- View Notice Serv LetDocument4 pagesView Notice Serv LetRonald FarrisNo ratings yet
- Imprimeeeeee PDFDocument52 pagesImprimeeeeee PDFKarina BarrientosNo ratings yet
- To Find Out If You Can Get or Keep Getting Benefits, We Need More Facts From YouDocument6 pagesTo Find Out If You Can Get or Keep Getting Benefits, We Need More Facts From YouDont HavnoideaNo ratings yet
- Amanda K Scott 3535 W Cambridge AVE Fresno, CA 93722-6561Document6 pagesAmanda K Scott 3535 W Cambridge AVE Fresno, CA 93722-6561Amanda Scott100% (1)
- About Your Benefits: State of WisconsinDocument6 pagesAbout Your Benefits: State of WisconsinJanelle GarrisonNo ratings yet
- Form 1099GDocument2 pagesForm 1099GMarcus KreseNo ratings yet
- Bank Statement - Feb.2020Document5 pagesBank Statement - Feb.2020TRIVEDI ANILNo ratings yet
- Repayment Application DocumentDocument10 pagesRepayment Application DocumentPratham TiwariNo ratings yet
- Fed Paper PDFDocument83 pagesFed Paper PDFWHRNo ratings yet
- Sample Renewal PDFDocument10 pagesSample Renewal PDFforStorylineNo ratings yet
- When To Use This Form: Servicesaustralia - Gov.au/centrelinkuploaddocsDocument10 pagesWhen To Use This Form: Servicesaustralia - Gov.au/centrelinkuploaddocsLyley YAYNo ratings yet
- Foodstamp LetterDocument6 pagesFoodstamp LetterTemisha BrownNo ratings yet
- Federal Direct Stafford/Ford Loan Federal Direct Unsubsidized Stafford/Ford Loan Master Promissory Note William D. Ford Federal Direct Loan ProgramDocument10 pagesFederal Direct Stafford/Ford Loan Federal Direct Unsubsidized Stafford/Ford Loan Master Promissory Note William D. Ford Federal Direct Loan ProgramPratham TiwariNo ratings yet
- GenerateDocument8 pagesGenerateAaron DeloachNo ratings yet
- BenefitVerificationLetter July August 2015Document1 pageBenefitVerificationLetter July August 2015Steven SchoferNo ratings yet
- Application 97586 PDFDocument3 pagesApplication 97586 PDFAnnie LamNo ratings yet
- Monetary Determination: Department of Labor and Human ResourcesDocument3 pagesMonetary Determination: Department of Labor and Human ResourcesBradley KirtsNo ratings yet
- Notice of Case ActionDocument4 pagesNotice of Case ActionOptical RecoveryNo ratings yet
- Financial Information Form WordDocument1 pageFinancial Information Form WordAfshin SarbazNo ratings yet
- Disaster Recovery Allowance: NSW Bushfires - September 2019Document16 pagesDisaster Recovery Allowance: NSW Bushfires - September 2019Scott FullerNo ratings yet
- KUTAI MCCB Circuit Breaker Transfer Switch With Remote Monitoring OptionsDocument11 pagesKUTAI MCCB Circuit Breaker Transfer Switch With Remote Monitoring OptionsJanice LuNo ratings yet
- View Notice ServletDocument8 pagesView Notice ServletLay Con100% (1)
- EligibilityResultsNotice 4Document11 pagesEligibilityResultsNotice 4Jeremy L. BellerNo ratings yet
- Local Training Companies DBDocument8 pagesLocal Training Companies DBMohammad MuhannaNo ratings yet
- Disclosure StatementDocument3 pagesDisclosure StatementWhoNo ratings yet
- Tsys Mpa With Logo 1Document6 pagesTsys Mpa With Logo 1api-503333470No ratings yet
- Application Summary: Wells Fargo Home Mortgage Rate Reduction ProgramDocument3 pagesApplication Summary: Wells Fargo Home Mortgage Rate Reduction Programpiehay7577No ratings yet
- Justin TranscriptDocument1 pageJustin Transcriptapi-360936757No ratings yet
- MS Birth Cert. AppDocument2 pagesMS Birth Cert. AppJonathanKiehlNo ratings yet
- Formsoppsapplication Illinois Birth Record 2018Document2 pagesFormsoppsapplication Illinois Birth Record 2018CynthiaNo ratings yet
- Electric BillDocument3 pagesElectric BillsatishkNo ratings yet
- 9701 DHS FIA CARES Application For Assistance Revised 2.2020 FINAL 15Document17 pages9701 DHS FIA CARES Application For Assistance Revised 2.2020 FINAL 15Ameer Tariq Shango ElNo ratings yet
- Affidavit of Support Under Section 213A of The INADocument10 pagesAffidavit of Support Under Section 213A of The INAIsamar BTNo ratings yet
- Direct Deposit AdviceDocument4 pagesDirect Deposit AdviceBel Leara0% (1)
- Background Form PDFDocument1 pageBackground Form PDFMiloNo ratings yet
- Generate 1Document6 pagesGenerate 1angeloaiden08No ratings yet
- GenerateDocument6 pagesGenerateAdriana SanchezNo ratings yet
- ReDocument3 pagesReSyahid FarhanNo ratings yet
- Tutorial 3Document2 pagesTutorial 3AmrinaAkmal0% (1)
- WS Soln 2 6A RationalFunctionsDocument6 pagesWS Soln 2 6A RationalFunctionsSiddhant ShahNo ratings yet
- UNIT V WearableDocument102 pagesUNIT V WearableajithaNo ratings yet
- Security+ Guide To Network Security Fundamentals, Fifth EditionDocument52 pagesSecurity+ Guide To Network Security Fundamentals, Fifth EditionVitæ ÆgisNo ratings yet
- LogisticsDocument5 pagesLogisticsHương LýNo ratings yet
- Fisher C1 Series Pneumatic Controllers and TransmittersDocument12 pagesFisher C1 Series Pneumatic Controllers and TransmittersAnderson KundeNo ratings yet
- Fridge Zanussi ZK2411VT5 ManualDocument14 pagesFridge Zanussi ZK2411VT5 ManualDragos MoscuNo ratings yet
- Transmission Line4 PDFDocument46 pagesTransmission Line4 PDFRevathi PrasadNo ratings yet
- ValuenetAnewbusinessmodelforthefoodindustry PDFDocument23 pagesValuenetAnewbusinessmodelforthefoodindustry PDFneera mailNo ratings yet
- Caso Contra Ángel Pérez: Respuesta de La Fiscalía A Moción de La Defensa Sobre Uso de FotosDocument8 pagesCaso Contra Ángel Pérez: Respuesta de La Fiscalía A Moción de La Defensa Sobre Uso de FotosEl Nuevo DíaNo ratings yet
- 7 - 8 CSS - WK 3 Ergonomic Guidelines For Computer Workstations - Jesucrtina NimenzoDocument6 pages7 - 8 CSS - WK 3 Ergonomic Guidelines For Computer Workstations - Jesucrtina NimenzoEdelmar BenosaNo ratings yet
- Jsa Camp Engine Service 350 HRSDocument1 pageJsa Camp Engine Service 350 HRSAdel AlKhedawyNo ratings yet
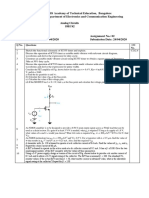
- Q No. Questions CO No.: C C W That Results in GDocument2 pagesQ No. Questions CO No.: C C W That Results in GSamarth SamaNo ratings yet
- LECTURE 11-Microalgal Biotechnology-Biofuels N BioproductsDocument16 pagesLECTURE 11-Microalgal Biotechnology-Biofuels N BioproductsIntan Lestari DewiNo ratings yet
- 12 Things You Must Know To Win A Full Scholarship in SwedenDocument51 pages12 Things You Must Know To Win A Full Scholarship in SwedenEmmanuel GeraldNo ratings yet
- Purchase Invoicing Guide AuDocument17 pagesPurchase Invoicing Guide AuYash VasudevaNo ratings yet
- Consumer Behaviour-Kiran GDocument9 pagesConsumer Behaviour-Kiran GVaibhav KhandelwalNo ratings yet
- The Object-Z Specification Language: Software Verification Research Centre University of QueenslandDocument155 pagesThe Object-Z Specification Language: Software Verification Research Centre University of QueenslandJulian Garcia TalanconNo ratings yet
- Class 1Document19 pagesClass 1Rahul BharadwajNo ratings yet
- Service Manual: Super Audio CD/DVD ReceiverDocument88 pagesService Manual: Super Audio CD/DVD Receiveralvhann_1No ratings yet
- Novtang (Int'l Wed)Document3 pagesNovtang (Int'l Wed)raymondsuwsNo ratings yet
- NURS FPX 6218 Assessment 4 Advocating For Lasting ChangeDocument8 pagesNURS FPX 6218 Assessment 4 Advocating For Lasting Changefarwaamjad771No ratings yet
- Promax Reference PDFDocument32 pagesPromax Reference PDFfarkli88No ratings yet
- Crop Insurance Proposal 31.07.2023 (CLN) PCPMD Inputs Rev SCIDocument14 pagesCrop Insurance Proposal 31.07.2023 (CLN) PCPMD Inputs Rev SCIĐỗ ThăngNo ratings yet
- A Study On Flywheel Energy Recovery From Aircraft BrakesDocument5 pagesA Study On Flywheel Energy Recovery From Aircraft BrakesRaniero FalzonNo ratings yet
- ZF SI 6hp Family Tree enDocument2 pagesZF SI 6hp Family Tree enfercho573No ratings yet