You might also like
- MEP IPC StatusDocument12 pagesMEP IPC StatusMARIO ALEXIS SANCHEZ ORTEGANo ratings yet
- Westside/ Health Center: To: Agnes & Port To: Port & TarltonDocument2 pagesWestside/ Health Center: To: Agnes & Port To: Port & Tarltonrcoffey_3No ratings yet
- LNL Iklcqd /: Page 1 of 6Document6 pagesLNL Iklcqd /: Page 1 of 6asmohanraj46No ratings yet
- Chart20230305184923 2Document2 pagesChart20230305184923 2samar jeetNo ratings yet
- DSSHD27938070000010004 NewDocument3 pagesDSSHD27938070000010004 NewDarren Joseph VivekNo ratings yet
- DSSHD2381399000001 NewDocument4 pagesDSSHD2381399000001 Newombir sainiNo ratings yet
- PUKOL01039700000010188 NewDocument5 pagesPUKOL01039700000010188 NewUnique ComputersNo ratings yet
- Cahflow (27-02-24)Document1 pageCahflow (27-02-24)eiohatNo ratings yet
- LNL Iklcqd /: Page 1 of 9Document9 pagesLNL Iklcqd /: Page 1 of 9ARVINDNo ratings yet
- BS-20 Seniority List 01-01-2022Document7 pagesBS-20 Seniority List 01-01-2022Fayaz KhanNo ratings yet
- BRPAT27888470000010042 NewDocument3 pagesBRPAT27888470000010042 NewSapna KumariNo ratings yet
- TNAMB00674380000020125 NewDocument3 pagesTNAMB00674380000020125 NewSM CreationNo ratings yet
- Top Sheet Refill - June-2020Document1 pageTop Sheet Refill - June-2020aktaruzzaman bethuNo ratings yet
- Service Bill StatusDocument2 pagesService Bill StatusKR RamanNo ratings yet
- j21 Oct - Web PDFDocument16 pagesj21 Oct - Web PDFSiddarth JainNo ratings yet
- Transfer TA BillDocument7 pagesTransfer TA BillHrshiya SharmaNo ratings yet
- Mahatma Gandhi National Rural Employment Guarantee Act Muster Roll (For Unskilled Labourer)Document3 pagesMahatma Gandhi National Rural Employment Guarantee Act Muster Roll (For Unskilled Labourer)deepak dashNo ratings yet
- PST UploadDocument125 pagesPST UploadRahid KhanNo ratings yet
- THVSH13559170000088947 NewDocument4 pagesTHVSH13559170000088947 NewVIVEK PNo ratings yet
- O&M 21-22 Adilabad Div Estimate - 10.05.2021 - Final (After Modification) @ 17.7.2021Document71 pagesO&M 21-22 Adilabad Div Estimate - 10.05.2021 - Final (After Modification) @ 17.7.2021Mahesh ChetpelliNo ratings yet
- MRNOI16338680000010199 NewDocument7 pagesMRNOI16338680000010199 NewGirish kumar kushwahaNo ratings yet
- Semest./Yr Semest./Yr Semest./Yr Semest./YrDocument1 pageSemest./Yr Semest./Yr Semest./Yr Semest./Yrhaiderrubab319No ratings yet
- GPS 134Document1 pageGPS 134NSO CADNo ratings yet
- Format Laporan MTBS 2019 EDITDocument14 pagesFormat Laporan MTBS 2019 EDITwabah bencana paserNo ratings yet
- GJAHD00519220000015865 NewDocument4 pagesGJAHD00519220000015865 NewVidya SagarNo ratings yet
- CR GST DetailsDocument2 pagesCR GST DetailsSRO BALANGIR STG BALANGIRNo ratings yet
- THTHA00993110000084433 NewDocument5 pagesTHTHA00993110000084433 NewSanket JadhavNo ratings yet
- Piggy Maths 2022fooie-1Document6 pagesPiggy Maths 2022fooie-1diradingwetebogoNo ratings yet
- Outlocation FormatDocument20 pagesOutlocation Formatnirajnishad1432No ratings yet
- December 15 - December 24Document7 pagesDecember 15 - December 24April NNo ratings yet
- Monthly Expense JULY 2020 04-08-20 PDFDocument3 pagesMonthly Expense JULY 2020 04-08-20 PDFBATRA INFOTECNo ratings yet
- Monthly Report of Disbursements: For The Month of January 2020 FAR No. 4Document11 pagesMonthly Report of Disbursements: For The Month of January 2020 FAR No. 4Dante TablateNo ratings yet
- PYBOM00341770000097943 NewDocument5 pagesPYBOM00341770000097943 NewCA Snehil PeriwalNo ratings yet
- Sunbeam School None GSTDocument1 pageSunbeam School None GSTRishoo SinhaNo ratings yet
- 37 March 2020Document2 pages37 March 2020rcoffey_3No ratings yet
- Detailed Contingent (DC) Bill FormatDocument2 pagesDetailed Contingent (DC) Bill FormatSaif AnsariNo ratings yet
- SPP 20/016 & SPP 20/015 H.V Cable / Transition Joint Replacement ProjectDocument38 pagesSPP 20/016 & SPP 20/015 H.V Cable / Transition Joint Replacement ProjectMohammed MisbahNo ratings yet
- Upbly00258470000000082 2016Document1 pageUpbly00258470000000082 2016Chowkidar Dhirendra Pratap SinghNo ratings yet
- Knmys20986860000010049 2021 2022Document5 pagesKnmys20986860000010049 2021 2022Yashwanth MSNo ratings yet
- PVC As Per Circular PDFDocument3 pagesPVC As Per Circular PDFVikas SainiNo ratings yet
- KNMYS20986860000010049 NewDocument5 pagesKNMYS20986860000010049 NewYashwanth MSNo ratings yet
- Billing Status NTDCDocument1 pageBilling Status NTDCMuhammad BilalNo ratings yet
- Claim Sheet Format1Document5 pagesClaim Sheet Format1sravan reddyNo ratings yet
- 1,172 Units: Zubair S/O A.AzizDocument2 pages1,172 Units: Zubair S/O A.AzizMuhammad KaleemNo ratings yet
- BisaDocument1 pageBisacybot43No ratings yet
- 1-My ProjectsDocument20 pages1-My ProjectsGurumoorthy RajavijayanNo ratings yet
- Print Muster Roll R Sa 02Document1 pagePrint Muster Roll R Sa 02AYUSHNo ratings yet
- MmssDocument1 pageMmssNafees ShaikNo ratings yet
- Punjab Public Service CommissionDocument33 pagesPunjab Public Service CommissionRanaFaizanNo ratings yet
- Ward 9 - Kulo - Meghram KoDocument5 pagesWard 9 - Kulo - Meghram KoPMEP Kapilvastu MunicipalityNo ratings yet
- Lista Cheltuieli NoiembrieDocument1 pageLista Cheltuieli NoiembrieBecheru GabrielNo ratings yet
- Sar (PVT) LTD Sar (PVT) LTD: Delivery Note Delivery NoteDocument1 pageSar (PVT) LTD Sar (PVT) LTD: Delivery Note Delivery NoteMelusi ShanziNo ratings yet
- CTC Pt. Sgi - 2018Document9 pagesCTC Pt. Sgi - 2018Rama Triwardana PolaniNo ratings yet
- 267 Units: Mrs Qamar Un NisaDocument2 pages267 Units: Mrs Qamar Un NisaWasimullah KhanNo ratings yet
- Construction ProgrammeDocument11 pagesConstruction Programmeniranjanchou100% (1)
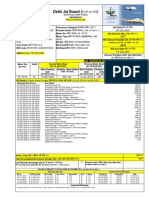
- Delhi Jal Board (: New Connection BillDocument3 pagesDelhi Jal Board (: New Connection BillAjit Pratap Singh ShakyaNo ratings yet
- TDE CX Overall Schedule 19-06-23Document3 pagesTDE CX Overall Schedule 19-06-23Vivi Alfiana UtamiNo ratings yet
- In-House Worker: Total Hrs Total Hrs Total Hrs Total Hrs Total Hrs Total HrsDocument1 pageIn-House Worker: Total Hrs Total Hrs Total Hrs Total Hrs Total Hrs Total HrsGenrey ConstructionNo ratings yet
- ORBBS00158130000010251 NewDocument3 pagesORBBS00158130000010251 NewRashmi RanjanNo ratings yet
- Typeform Invoice BTLWMgTYQCPq91RjvDocument1 pageTypeform Invoice BTLWMgTYQCPq91RjvAakash vermaNo ratings yet
- NIPT PLUS - DummyDocument4 pagesNIPT PLUS - DummyAakash vermaNo ratings yet
- Sanger Dummy ReportDocument3 pagesSanger Dummy ReportAakash vermaNo ratings yet
- Unit 1 NetworkingDocument29 pagesUnit 1 NetworkingVanshika SharmaNo ratings yet
- MLPA Dummy ReportDocument3 pagesMLPA Dummy ReportAakash verma100% (1)
- Check List For Design Program of A Parish ChurchDocument11 pagesCheck List For Design Program of A Parish ChurchQuinn HarloweNo ratings yet
- p1632 eDocument4 pagesp1632 ejohn saenzNo ratings yet
- Hydrogen ReviewDocument53 pagesHydrogen Reviewjuric98No ratings yet
- Sbi Afi 2012Document48 pagesSbi Afi 2012Moneylife FoundationNo ratings yet
- Review Systems of Linear Equations All MethodsDocument4 pagesReview Systems of Linear Equations All Methodsapi-265647260No ratings yet
- Bubble SortDocument6 pagesBubble SortRollin RevieNo ratings yet
- Game On Series BibleDocument28 pagesGame On Series Bibleapi-513832615No ratings yet
- Family School Project Lesson Plan AstrologyDocument3 pagesFamily School Project Lesson Plan Astrologyapi-529488210No ratings yet
- The Impact of Social Networking Sites To The Academic Performance of The College Students of Lyceum of The Philippines - LagunaDocument15 pagesThe Impact of Social Networking Sites To The Academic Performance of The College Students of Lyceum of The Philippines - LagunaAasvogel Felodese Carnivora64% (14)
- Episode Transcript: Episode 34 - Chinese Han Lacquer CupDocument2 pagesEpisode Transcript: Episode 34 - Chinese Han Lacquer CupParvathy SubramanianNo ratings yet
- AC7140 Rev CDocument73 pagesAC7140 Rev CRanga100% (1)
- Caterpillar Sis (01.2014) MultilanguageDocument10 pagesCaterpillar Sis (01.2014) MultilanguageTemmy Candra Wijaya100% (1)
- VRF Mv6R: Heat Recovery Outdoor UnitsDocument10 pagesVRF Mv6R: Heat Recovery Outdoor UnitsTony NguyenNo ratings yet
- Imcp - RocketbookDocument11 pagesImcp - Rocketbookapi-690398026No ratings yet
- Practice Quiz Reflection Project Initiation and Key ComponentsDocument3 pagesPractice Quiz Reflection Project Initiation and Key ComponentsFalastin Tanani67% (3)
- Practical CS ProcessingDocument483 pagesPractical CS ProcessinganAMUstudent100% (2)
- Kitchen Equipment Handling and Maintaining Standard Procedure and PoliciesDocument2 pagesKitchen Equipment Handling and Maintaining Standard Procedure and PoliciesChef Chef75% (4)
- Why Do Kashmiris Need Self-Determination?: UncategorizedDocument16 pagesWhy Do Kashmiris Need Self-Determination?: UncategorizedFarooq SiddiqiNo ratings yet
- Definition Nature and Scope of Urban GeographyDocument4 pagesDefinition Nature and Scope of Urban Geographysamim akhtarNo ratings yet
- Market Challengers StrategiesDocument19 pagesMarket Challengers Strategiestobbob007100% (20)
- Castle CrashesDocument21 pagesCastle Crasheswicked wolfNo ratings yet
- Preliminary Voters ListDocument86 pagesPreliminary Voters Listمحمد منيب عبادNo ratings yet
- EPA NCP Technical Notebook PDFDocument191 pagesEPA NCP Technical Notebook PDFlavrikNo ratings yet
- SM-G900F Esquematico Completo Anibal Garcia IrepairDocument2 pagesSM-G900F Esquematico Completo Anibal Garcia Irepairfix marketNo ratings yet
- Damask: by ChenoneDocument17 pagesDamask: by ChenoneYasir IjazNo ratings yet
- Quizlet Table 7Document1 pageQuizlet Table 7JosielynNo ratings yet
- Claudio MonteverdiDocument2 pagesClaudio MonteverdiBrendan LynchNo ratings yet
- SLHT Grade 7 CSS Week 5 Without Answer KeyDocument6 pagesSLHT Grade 7 CSS Week 5 Without Answer KeyprinceyahweNo ratings yet
- Professional Development Objectives Related To Modalities Specific TopicsDocument3 pagesProfessional Development Objectives Related To Modalities Specific TopicsCris100% (1)
- Lecture 08Document32 pagesLecture 08SusovanNo ratings yet