You might also like
- 2005-2010 Tacoma Bed Extender PT329-35050 Rev. A - PT329-35050Document8 pages2005-2010 Tacoma Bed Extender PT329-35050 Rev. A - PT329-35050kylemac123No ratings yet
- ESRDDocument37 pagesESRDVecky TolentinoNo ratings yet
- Composite Metal Deck Slab Design As Per EC4Document86 pagesComposite Metal Deck Slab Design As Per EC4asubhash110% (1)
- Anemia Unspecified FinalDocument47 pagesAnemia Unspecified FinalMaria Paula BungayNo ratings yet
- Uterine Fibroids Case StudyDocument38 pagesUterine Fibroids Case StudyFiona Cheryl Amsterdam80% (5)
- Hemophilia PathophysiologyDocument79 pagesHemophilia Pathophysiologyjeba100% (8)
- CHF Case Study on Congestive Heart FailureDocument40 pagesCHF Case Study on Congestive Heart Failurelyndzy100% (1)
- Case Study NSTEMIDocument26 pagesCase Study NSTEMIHomework Ping100% (1)
- Ugib Case StudyDocument33 pagesUgib Case StudyRosemarie Cunanan Grifoni100% (1)
- EndocarditisDocument6 pagesEndocarditisMerry Joy DeliñaNo ratings yet
- Tribology and Dynamics of Engine and Powertrain Fundamentals Applications and Future TrendsDocument13 pagesTribology and Dynamics of Engine and Powertrain Fundamentals Applications and Future Trendskumar_yogesh2238810% (2)
- Dont Think About A ZebraDocument2 pagesDont Think About A ZebraD2WNo ratings yet
- AnaemiaDocument43 pagesAnaemiaMy NameNo ratings yet
- Case Presentation of AnemiaDocument71 pagesCase Presentation of AnemiaJessica Esther Canlas100% (2)
- Managing Diabetes with Lifestyle Changes and MedicationDocument9 pagesManaging Diabetes with Lifestyle Changes and MedicationCalingalan Hussin CaluangNo ratings yet
- AnemiaDocument13 pagesAnemiaguptaavni0000No ratings yet
- NEONATAL ANEMIA GUIDEDocument32 pagesNEONATAL ANEMIA GUIDETria100% (1)
- Abnormal Uterine Bleeding Iron Deficiency Anemia Secondary Case StudyDocument133 pagesAbnormal Uterine Bleeding Iron Deficiency Anemia Secondary Case StudyZhyrraRamirezGarcia100% (1)
- Case English 1 - NDI Edit 220419Document24 pagesCase English 1 - NDI Edit 220419syongebobNo ratings yet
- A Very Pale Three-Year-Old: Case 2 Diagnosis: Transient Erythroblastopenia of ChildhoodDocument3 pagesA Very Pale Three-Year-Old: Case 2 Diagnosis: Transient Erythroblastopenia of ChildhoodYukii Triby-a AnniimesztNo ratings yet
- Aplastic AnemiaDocument26 pagesAplastic AnemiaMark Anthony S. Castillo100% (1)
- Exposure To Toxic SubstancesDocument21 pagesExposure To Toxic SubstancesDavid VillanuevaNo ratings yet
- Hypochromic Microcytic Anemia: Presented By: Frisca Angreni 02-032Document96 pagesHypochromic Microcytic Anemia: Presented By: Frisca Angreni 02-032Margaretha MonikaNo ratings yet
- Etiology: Abruptio Placenta Nursing Care Plan and ManagementDocument37 pagesEtiology: Abruptio Placenta Nursing Care Plan and ManagementKeia Chiara DiazNo ratings yet
- Case Study Labour RoomDocument21 pagesCase Study Labour RoomMohd HarizNo ratings yet
- MCN CaseDocument114 pagesMCN CaseMae Arra Lecobu-anNo ratings yet
- Cyclic VomitingDocument3 pagesCyclic VomitingHitesh BansalNo ratings yet
- Exposure To Toxic SubstancesDocument21 pagesExposure To Toxic SubstancesDavid VillanuevaNo ratings yet
- Exposure To Toxic SubstancesDocument21 pagesExposure To Toxic SubstancesDavid VillanuevaNo ratings yet
- Hereditary SpherocytosisDocument39 pagesHereditary SpherocytosisjoannaNo ratings yet
- Chapter 44: Nursing Care of The Client With An Hematologic DisordersDocument18 pagesChapter 44: Nursing Care of The Client With An Hematologic DisordersfLOR_ZIANE_MAENo ratings yet
- Introduction To The CaseDocument6 pagesIntroduction To The CaseTrixia AlmendralNo ratings yet
- Case Study On Pregnancy Induced Hypertension (PIH) : University of Northern Philippines College of NursingDocument42 pagesCase Study On Pregnancy Induced Hypertension (PIH) : University of Northern Philippines College of Nursing3B NOVIDA, ALEYA G.No ratings yet
- 8BBK Lec8 - HDN MQA 2019-09-26 08 - 14 - 44Document32 pages8BBK Lec8 - HDN MQA 2019-09-26 08 - 14 - 44gothai sivapragasamNo ratings yet
- Approach To PallorDocument25 pagesApproach To PallorlaibaNo ratings yet
- Group e Polycythemia Verapinakafinal 2Document75 pagesGroup e Polycythemia Verapinakafinal 2deserieroseonateNo ratings yet
- POSTNATAL CAREDocument33 pagesPOSTNATAL CAREAmala George100% (2)
- Case Study 1Document8 pagesCase Study 1inspire.nacNo ratings yet
- Hydatidiform Mole Diagnosis in 38-Year-Old WomanDocument23 pagesHydatidiform Mole Diagnosis in 38-Year-Old WomanMikko ArriesgoddessNo ratings yet
- BM18110019 Shrley Chee See Yin (R2 Obstetric Cwu)Document12 pagesBM18110019 Shrley Chee See Yin (R2 Obstetric Cwu)RUDOLF YUSON BM20110052No ratings yet
- Anaemia in PregnancyDocument28 pagesAnaemia in PregnancyUsman G. HingoroNo ratings yet
- Pat2 Med Surg 2Document19 pagesPat2 Med Surg 2api-339132978No ratings yet
- Precocious Puberty With Primary Hypothyroidism Due To Autoimmune ThyroiditisDocument3 pagesPrecocious Puberty With Primary Hypothyroidism Due To Autoimmune ThyroiditisShohel RanaNo ratings yet
- Module 12 Hematology and Oncology Hevinkumar PatelDocument24 pagesModule 12 Hematology and Oncology Hevinkumar PatelhevinpatelNo ratings yet
- Hematuria in PregnancyDocument3 pagesHematuria in PregnancyMax StevanusNo ratings yet
- The Patient With Rhabdomyolysis: Have You Considered Quail Poisoning?Document2 pagesThe Patient With Rhabdomyolysis: Have You Considered Quail Poisoning?andriopaNo ratings yet
- Nursing Practice ExamDocument9 pagesNursing Practice ExamMeray Snggcl SnglnganNo ratings yet
- Azazim 2012 PDFDocument27 pagesAzazim 2012 PDFShowmik PaulNo ratings yet
- GDM Gestational Diabetes Mellitus.: Sultanate of Oman Ministry of Health Maternal Health Nursing (Practicum)Document21 pagesGDM Gestational Diabetes Mellitus.: Sultanate of Oman Ministry of Health Maternal Health Nursing (Practicum)safa AlsaidiNo ratings yet
- Anemia PregnancyDocument122 pagesAnemia PregnancySenthil NathNo ratings yet
- A Case Study Presentation On: Chronic Kidney DiseaseDocument63 pagesA Case Study Presentation On: Chronic Kidney DiseaseFayeann Vedor LoriegaNo ratings yet
- Patient'S ProfileDocument6 pagesPatient'S ProfileMichelle Danica Vicente PaswickNo ratings yet
- Casestudy Makato 2nd Pre EclampsiaDocument7 pagesCasestudy Makato 2nd Pre EclampsiaRainier IbarretaNo ratings yet
- Long Case Rama FixDocument13 pagesLong Case Rama FixRamaNo ratings yet
- BAIAE in Pregnancy.Document6 pagesBAIAE in Pregnancy.Mark Arthur MartinezNo ratings yet
- MaeDocument9 pagesMaeCharmaigne Mae Padilla Sotelo100% (1)
- Case Study Uro FinalDocument44 pagesCase Study Uro FinalDan Ataniel EnsaladaNo ratings yet
- Acute Glomerulonephritis GCDocument70 pagesAcute Glomerulonephritis GCMary Cruz100% (2)
- EGA-IUGR Tampil PDFDocument18 pagesEGA-IUGR Tampil PDFtrianggonoNo ratings yet
- Hypoglycemia in Diabetes: Pathophysiology, Prevalence, and PreventionFrom EverandHypoglycemia in Diabetes: Pathophysiology, Prevalence, and PreventionNo ratings yet
- Semi Finals Examination 2Document4 pagesSemi Finals Examination 2Annie Lou AbrahamNo ratings yet
- LeukemiaDocument34 pagesLeukemiaAnnie Lou AbrahamNo ratings yet
- Annie's Social Media Security TipsDocument1 pageAnnie's Social Media Security TipsAnnie Lou AbrahamNo ratings yet
- Heart STCH 2 - PNG: Cross Stitch ChartDocument25 pagesHeart STCH 2 - PNG: Cross Stitch ChartAnnie Lou AbrahamNo ratings yet
- Scenario No.3 BubosabrahamDocument4 pagesScenario No.3 BubosabrahamAnnie Lou AbrahamNo ratings yet
- LAB EXERCISES PRELIM - Abraham BSN1ADocument19 pagesLAB EXERCISES PRELIM - Abraham BSN1AAnnie Lou AbrahamNo ratings yet
- Blank QuizDocument19 pagesBlank QuizAnnie Lou AbrahamNo ratings yet
- LM 2 (Summative Assessment)Document1 pageLM 2 (Summative Assessment)Annie Lou AbrahamNo ratings yet
- LAB EXERCISES FINAL - Anatomy - Abraham BSN1ADocument18 pagesLAB EXERCISES FINAL - Anatomy - Abraham BSN1AAnnie Lou AbrahamNo ratings yet
- Respiratory Quiz - FINAL - Abraham BSN 1ADocument2 pagesRespiratory Quiz - FINAL - Abraham BSN 1AAnnie Lou AbrahamNo ratings yet
- LAB EXERCISES MIDTERMS - Abraham BSN1ADocument19 pagesLAB EXERCISES MIDTERMS - Abraham BSN1AAnnie Lou AbrahamNo ratings yet
- LAB EXERCISES SEMIFINAL - Abraham BSN1ADocument10 pagesLAB EXERCISES SEMIFINAL - Abraham BSN1AAnnie Lou AbrahamNo ratings yet
- MidtermsDocument7 pagesMidtermsAnnie Lou AbrahamNo ratings yet
- Health Entrep LessonDocument11 pagesHealth Entrep LessonAnnie Lou AbrahamNo ratings yet
- UntitledDocument1 pageUntitledAnnie Lou AbrahamNo ratings yet
- Vernacular ArchitectureDocument16 pagesVernacular ArchitectureHasita KrovvidiNo ratings yet
- 500daysofsummerphilosopy Reflection DraftDocument3 pages500daysofsummerphilosopy Reflection DraftAiralyn SaceNo ratings yet
- Steel Code Check Theory EnuDocument341 pagesSteel Code Check Theory Enupopaciprian27No ratings yet
- La Villa Fact Sheet 2021-2022-UpdatedDocument4 pagesLa Villa Fact Sheet 2021-2022-Updatedsweta suresh ganvirNo ratings yet
- Island of The Blue Dolphins: Before You Read The ChaptersDocument12 pagesIsland of The Blue Dolphins: Before You Read The ChaptersCostea CibanuNo ratings yet
- Akanānuru - Some Poems (2012 - 10 - 29 02 - 55 - 25 UTC)Document9 pagesAkanānuru - Some Poems (2012 - 10 - 29 02 - 55 - 25 UTC)Ravi SoniNo ratings yet
- TestDocument3 pagesTestIonescu Cristina-LucianaNo ratings yet
- Prota - Stiffness FactorDocument7 pagesProta - Stiffness FactorA K100% (1)
- Cossh Risk Assessment: Carried Out By: Department: Date: Substance Name: CRA NumberDocument4 pagesCossh Risk Assessment: Carried Out By: Department: Date: Substance Name: CRA NumberRocky BisNo ratings yet
- MEK 10103 ELECTRIC DRIVES AND APPLICATIONSDocument23 pagesMEK 10103 ELECTRIC DRIVES AND APPLICATIONSNazrul KocyNo ratings yet
- 986.33 Mesofilos Aerobios-PetrifilmDocument1 page986.33 Mesofilos Aerobios-PetrifilmBleidy NieblesNo ratings yet
- Sehr I Time 2012 DelhiDocument1 pageSehr I Time 2012 DelhiVaibhav VermaNo ratings yet
- Python Programming For Mechanical EngineersDocument93 pagesPython Programming For Mechanical EngineerslucianoprocopioNo ratings yet
- Catalogo RobinsonDocument8 pagesCatalogo RobinsonclerigonsaNo ratings yet
- Cambridge IGCSE™: Geography 0460/41 October/November 2020Document9 pagesCambridge IGCSE™: Geography 0460/41 October/November 2020RutendoNo ratings yet
- Taller de Calor EstDocument2 pagesTaller de Calor EstDiegoMuñozNo ratings yet
- BMW Inyeccion 320i-325i Motronic M31 PDFDocument2 pagesBMW Inyeccion 320i-325i Motronic M31 PDFIvoo ooNo ratings yet
- Geotechnical Module: Powerful Software Featuring Intuitive WorkflowDocument4 pagesGeotechnical Module: Powerful Software Featuring Intuitive WorkflowMuhammadAviCennaNo ratings yet
- Prospectus PDFDocument40 pagesProspectus PDFSony ManojNo ratings yet
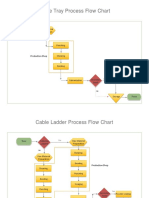
- Process Flow ChartDocument4 pagesProcess Flow Chartchacko chiramalNo ratings yet
- Zoom Basic Functions - FinalDocument31 pagesZoom Basic Functions - FinalWenshy LavadorNo ratings yet
- Braithwaite 2017 Complexity Science in Healthcare A White PaperDocument129 pagesBraithwaite 2017 Complexity Science in Healthcare A White PaperFinga Hitam ManiesNo ratings yet
- Concepts of ProbabilityDocument32 pagesConcepts of ProbabilityRushina SinghiNo ratings yet
- Sumalinog Teodoro Jr. LPDocument5 pagesSumalinog Teodoro Jr. LPDAITO CHRISTIAN DHARELNo ratings yet
- History of Nano FiltrationDocument42 pagesHistory of Nano FiltrationKieran Sexton100% (2)
- ACS Sainsbury and Asda Merger Leaner 82Document26 pagesACS Sainsbury and Asda Merger Leaner 82FlareGBANo ratings yet