You might also like
- Motovario MaintenanceDocument72 pagesMotovario Maintenancearachman297988No ratings yet
- 24in Pipeline Buoyancy CalculationDocument1 page24in Pipeline Buoyancy CalculationAdaghara67% (3)
- 05 Aphakia and PseudophakiaDocument15 pages05 Aphakia and PseudophakiaMwanja Moses100% (1)
- Aspheric IOLs Fact vs MythDocument8 pagesAspheric IOLs Fact vs MythAnonymous h0DxuJTNo ratings yet
- Comparative Effects of Various Types of Toric Intraocular Lenses On Astigmatism CorrectionDocument9 pagesComparative Effects of Various Types of Toric Intraocular Lenses On Astigmatism CorrectionAndrés QueupumilNo ratings yet
- Comparison of The Optical Behaviour of Five Different Multifocal Diffractive Intraocular Lenses in A Model EyeDocument12 pagesComparison of The Optical Behaviour of Five Different Multifocal Diffractive Intraocular Lenses in A Model Eye7zhm9d9dbpNo ratings yet
- 10 1111@aos 12521Document7 pages10 1111@aos 12521Mariana Luzardo bravoNo ratings yet
- Retinal Image Contrast Obtained by A Model Eye With Combined Correction of Chromatic and Spherical AberrationsDocument9 pagesRetinal Image Contrast Obtained by A Model Eye With Combined Correction of Chromatic and Spherical AberrationsTjundewo LawuNo ratings yet
- IndianJOphthalmol624461-9214366 023334Document3 pagesIndianJOphthalmol624461-9214366 023334secret_sunsetNo ratings yet
- Intraindividual Comparison of Aspherical and Spherical Intraocular Lenses of Same Material and PlatformDocument6 pagesIntraindividual Comparison of Aspherical and Spherical Intraocular Lenses of Same Material and PlatformAkhilesh KumarNo ratings yet
- Jurnal KuDocument6 pagesJurnal KuTamsilNo ratings yet
- IOL Power Calculation, Correction of Defocus - CH 4Document18 pagesIOL Power Calculation, Correction of Defocus - CH 4riveliNo ratings yet
- Extended Depth of Focus Iols The Next Chapter in Refractive TechnologyDocument4 pagesExtended Depth of Focus Iols The Next Chapter in Refractive TechnologyCDloperNo ratings yet
- ArtIOLs - Biblio 2Document16 pagesArtIOLs - Biblio 2blazquezjoseignacioNo ratings yet
- Evaluation_of_impact_of_posterior_phakic_IOL3_240221_093036Document6 pagesEvaluation_of_impact_of_posterior_phakic_IOL3_240221_093036kimie PazNo ratings yet
- Clinical Differences Between Toric Intraocular LenDocument8 pagesClinical Differences Between Toric Intraocular LenonderonderNo ratings yet
- Rotational Stability of Toric Intraocular - 2022 - Medical Journal Armed ForcesDocument6 pagesRotational Stability of Toric Intraocular - 2022 - Medical Journal Armed ForcesAnisha RanaNo ratings yet
- SocivoDocument16 pagesSocivoSlobodan MilovanovicNo ratings yet
- Acta Ophthalmologica - 2020 - Ota - Subjective and Objective Refractions in Eyes With Extended Depth of Focus IntraocularDocument7 pagesActa Ophthalmologica - 2020 - Ota - Subjective and Objective Refractions in Eyes With Extended Depth of Focus IntraocularFachry RahmanNo ratings yet
- Ray-tracing analysis accurately determines true IOL powerDocument7 pagesRay-tracing analysis accurately determines true IOL powerCamila GuerraNo ratings yet
- Bifocal Contact Lenses PDFDocument10 pagesBifocal Contact Lenses PDFLauw Dwi AndrikNo ratings yet
- Aberraciones Modelo de Ojo 2342Document11 pagesAberraciones Modelo de Ojo 2342pacaNo ratings yet
- Jurnal MataDocument7 pagesJurnal Matahelmi luthfiNo ratings yet
- The Optical Design of The Human Eye: A Critical ReviewDocument16 pagesThe Optical Design of The Human Eye: A Critical ReviewAna LabeNo ratings yet
- Hydrophobic Acrylic IOL Materials and DesignsDocument6 pagesHydrophobic Acrylic IOL Materials and DesignsArif MohammadNo ratings yet
- J Jcrs 2015 10 050Document8 pagesJ Jcrs 2015 10 050FrancescFranquesaNo ratings yet
- High Myopiaypartial Reduction Ortho-K: A 2-Year Randomized StudyDocument10 pagesHigh Myopiaypartial Reduction Ortho-K: A 2-Year Randomized StudykarakuraNo ratings yet
- Influence of Postoperative Astigmatism On Uncorrected Near Visual Acuity in PseudophakiaDocument7 pagesInfluence of Postoperative Astigmatism On Uncorrected Near Visual Acuity in PseudophakiaIJAR JOURNALNo ratings yet
- Accuracy of Intraocular Lens Power Calculation inDocument7 pagesAccuracy of Intraocular Lens Power Calculation inHerryantoThomassawaNo ratings yet
- Thesis Topics in Ophthalmology in AiimsDocument5 pagesThesis Topics in Ophthalmology in AiimsBuyCollegePaperOnlineUK100% (1)
- Accurate Optical Biometry Using IOL MasterDocument5 pagesAccurate Optical Biometry Using IOL Mastermuzicka9No ratings yet
- Retinal Image Quality of A Human Eye Model - OSLO LT SoftwareDocument11 pagesRetinal Image Quality of A Human Eye Model - OSLO LT SoftwareRadu BabauNo ratings yet
- Biometry by Suryakant Jha and Wangchuk Doma PDFDocument5 pagesBiometry by Suryakant Jha and Wangchuk Doma PDFJavier Andrés Pinochet SantoroNo ratings yet
- Toric ICLDocument8 pagesToric ICLjbahalkehNo ratings yet
- Our Experience With AcrySof Toric IOL DR Suresh K Pandey, SuVi Eye Institute Kota Rajasthan IndiaDocument51 pagesOur Experience With AcrySof Toric IOL DR Suresh K Pandey, SuVi Eye Institute Kota Rajasthan IndiaDr Suresh K Pandey100% (1)
- Optimized Singlet Lens DesignDocument6 pagesOptimized Singlet Lens Designffb.boy.30No ratings yet
- Calculation of Toric Intraocular Lenses Using Multivariate RegressionDocument9 pagesCalculation of Toric Intraocular Lenses Using Multivariate RegressionRonald PuchaNo ratings yet
- Kruger 2000Document5 pagesKruger 2000Magista NugrahaNo ratings yet
- The Human Eye Is An Example of Robust Optical Design: Pablo Artal Antonio Benito Juan TaberneroDocument7 pagesThe Human Eye Is An Example of Robust Optical Design: Pablo Artal Antonio Benito Juan TaberneroRaúl Plasencia SaliniNo ratings yet
- Presbyopia Correcting Iols For Phakic & Pseudophakic Eyes: Eps Technology: A Special Concept With Multiple ApplicationsDocument8 pagesPresbyopia Correcting Iols For Phakic & Pseudophakic Eyes: Eps Technology: A Special Concept With Multiple ApplicationsAbhijit PatilNo ratings yet
- Opth 14 815Document8 pagesOpth 14 815Andrés QueupumilNo ratings yet
- Multifocal Intraocular Lenses: Roberto BellucciDocument5 pagesMultifocal Intraocular Lenses: Roberto BellucciMaria ArNo ratings yet
- Five_generations_of_intraocular_lens_power_calculaDocument22 pagesFive_generations_of_intraocular_lens_power_calculaApps OmNo ratings yet
- Phakic Intraocular Lenses SurveyDocument40 pagesPhakic Intraocular Lenses SurveyAlexNo ratings yet
- Implantation of Refractive Multifocal Intraocular Lens With A Surface-Embedded Near Section For Cataract Eyes Complicated With A Coexisting Ocular PathologyDocument7 pagesImplantation of Refractive Multifocal Intraocular Lens With A Surface-Embedded Near Section For Cataract Eyes Complicated With A Coexisting Ocular PathologyAndrew MNo ratings yet
- JSD 2 56Document5 pagesJSD 2 56Swapnil RastogiNo ratings yet
- Cataract surgery accuracy with wavefront technologyDocument3 pagesCataract surgery accuracy with wavefront technologyR Andres Plaza ZNo ratings yet
- Using The Pentacam™ Calculation: For IOL PowerDocument4 pagesUsing The Pentacam™ Calculation: For IOL PowerGerardo Felipe Mora ZepedaNo ratings yet
- Intraoperative Aberrometry With The ORA™ System - P US ORA 2000019Document28 pagesIntraoperative Aberrometry With The ORA™ System - P US ORA 2000019antoniopbnetoNo ratings yet
- IOL Pitting - Mathews 2023Document2 pagesIOL Pitting - Mathews 2023Sangeeta MataniNo ratings yet
- Clinical Study: Aspheric Intraocular Lenses Implantation For Cataract Patients With Extreme MyopiaDocument6 pagesClinical Study: Aspheric Intraocular Lenses Implantation For Cataract Patients With Extreme MyopiaKevin ArdiansyahNo ratings yet
- DRL The Most Comprehensive System in ORTHO-K PRECILENSDocument4 pagesDRL The Most Comprehensive System in ORTHO-K PRECILENSwangging liNo ratings yet
- Toric Intraocular Lenses in Cataract Surgery: Nienke Visser, Noël J.C. Bauer and Rudy M.M.A. NuijtsDocument27 pagesToric Intraocular Lenses in Cataract Surgery: Nienke Visser, Noël J.C. Bauer and Rudy M.M.A. NuijtsArif MohammadNo ratings yet
- Kjo Jurnal MataDocument7 pagesKjo Jurnal Matanurul hidayati sNo ratings yet
- 1 s2.0 S2451993617300890 Main PDFDocument4 pages1 s2.0 S2451993617300890 Main PDFPutri Rahmadhani Ngakpaniklage AsdsNo ratings yet
- HamidDocument2 pagesHamidostebeNo ratings yet
- PIIS0002939422003841Document6 pagesPIIS0002939422003841Anca Florina GaceaNo ratings yet
- The Analysis of AC/A Ratio in Nonrefractive Accommodative Esotropia Treated With Bifocal GlassesDocument6 pagesThe Analysis of AC/A Ratio in Nonrefractive Accommodative Esotropia Treated With Bifocal GlassesTimbul SianturiNo ratings yet
- Intraocular Lens Power Calculation in Eyes With Previous Corneal Refractive SurgeryDocument10 pagesIntraocular Lens Power Calculation in Eyes With Previous Corneal Refractive Surgerymoni7777No ratings yet
- Contact Lens & Anterior EyeDocument4 pagesContact Lens & Anterior EyePin Han NaNo ratings yet
- s12886 022 02600 XDocument8 pagess12886 022 02600 XHariom ShuklaNo ratings yet
- Cyber Kit Motors enDocument8 pagesCyber Kit Motors enmakkihassanNo ratings yet
- Membrane Filtration Processes ExplainedDocument93 pagesMembrane Filtration Processes ExplainedMilind MatangNo ratings yet
- IFE Level 4 Certificate in Fire Science and Fire SafetyDocument8 pagesIFE Level 4 Certificate in Fire Science and Fire SafetyDebayanbasu.juNo ratings yet
- Family Orion Vertical 2018-12-11Document2 pagesFamily Orion Vertical 2018-12-11BobNo ratings yet
- JKM525 545M 72HL4 BDVP F3.1 enDocument2 pagesJKM525 545M 72HL4 BDVP F3.1 enluis starkNo ratings yet
- Vibratory Compactor With Hammtronic: C M Y CM MY Cy Cmy KDocument2 pagesVibratory Compactor With Hammtronic: C M Y CM MY Cy Cmy KCopemaq CopemaqNo ratings yet
- Tedom CHP UnitsDocument2 pagesTedom CHP UnitsMadhav RathourNo ratings yet
- Project ReportDocument40 pagesProject ReportSuresh SuriNo ratings yet
- Maths 1 Mark QuestionsDocument27 pagesMaths 1 Mark QuestionsSpandan NNo ratings yet
- Coulomb's LawDocument4 pagesCoulomb's LawPeterCiezczakNo ratings yet
- PHET Rates of Reaction SimDocument5 pagesPHET Rates of Reaction SimflickerNo ratings yet
- Lecture Nine: Best Vision Sphere (BVS) and Stenopaeic SlitDocument24 pagesLecture Nine: Best Vision Sphere (BVS) and Stenopaeic Slithenok birukNo ratings yet
- Unit 12 Pages From 0625 - s16 - QP - 43Document2 pagesUnit 12 Pages From 0625 - s16 - QP - 43Nicole NicoleNo ratings yet
- Shore Hardness Tester Ld0550 d44Document2 pagesShore Hardness Tester Ld0550 d44JohnNo ratings yet
- IQTI Vision DocumentDocument33 pagesIQTI Vision Documentabi sathwikNo ratings yet
- Agilent 1200 Series Binary PumpDocument136 pagesAgilent 1200 Series Binary PumpYu Han-HallettNo ratings yet
- E-Content #03 (RSR) Thesis and Research Paper Writing - A BriefDocument2 pagesE-Content #03 (RSR) Thesis and Research Paper Writing - A Briefaravind mouryaNo ratings yet
- Material Science and MetallurgyDocument43 pagesMaterial Science and MetallurgySanjay Kumar SinghNo ratings yet
- A Level Physics Flying Start GuideDocument9 pagesA Level Physics Flying Start GuideNiall QuadrosNo ratings yet
- Assignment - Chapter 1 - DHRUVKUMAR PATELDocument4 pagesAssignment - Chapter 1 - DHRUVKUMAR PATELDhruv PatelNo ratings yet
- Biology Processes and StructuresDocument157 pagesBiology Processes and StructuresOmar SedkeyNo ratings yet
- 2850 L3u308 Handout 16Document5 pages2850 L3u308 Handout 16Icee Sanie TibraNo ratings yet
- General Navigation Lesson Flow GuideDocument2 pagesGeneral Navigation Lesson Flow GuidehananeNo ratings yet
- Ch31&32 Electromagnetism SlidesDocument38 pagesCh31&32 Electromagnetism SlidesVent101No ratings yet
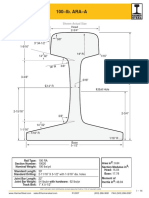
- 100 Lb-Yd ARA-ADocument1 page100 Lb-Yd ARA-ADario Bravo BordaNo ratings yet
- Riyadh Ductwork Project Pressure Loss CalculationsDocument1 pageRiyadh Ductwork Project Pressure Loss CalculationsFahad NaveedNo ratings yet
- Uncracked Concrete Anchor Plate DesignDocument8 pagesUncracked Concrete Anchor Plate DesignPhan TamNo ratings yet