You might also like
- Endocrine System (Pathophysiology)Document18 pagesEndocrine System (Pathophysiology)roselle legson100% (1)
- Nbme 11 ExplainationDocument55 pagesNbme 11 Explainationazankhan9960% (10)
- Adrenal and Pitutary Disoreders Adigrat LecDocument144 pagesAdrenal and Pitutary Disoreders Adigrat Lecbereket gashuNo ratings yet
- MRCP 2-Practice Questions-Book.2 PDFDocument161 pagesMRCP 2-Practice Questions-Book.2 PDFibanNo ratings yet
- OBGYN NotesDocument29 pagesOBGYN NotesavavNo ratings yet
- Test Bank For The Human Body in Health and Disease 6th EditionDocument20 pagesTest Bank For The Human Body in Health and Disease 6th Editionstephaniemendozagamobckjqf100% (18)
- Cushing's DiseaseDocument1 pageCushing's DiseaseAdeline N. OmeneNo ratings yet
- Im Testing For Endocrine DisordersDocument7 pagesIm Testing For Endocrine DisordersChristine MendozaNo ratings yet
- Cushing Syndrome - JAMA. 2023Document12 pagesCushing Syndrome - JAMA. 2023Teresa OrtizNo ratings yet
- Cushing Syndrome 2Document16 pagesCushing Syndrome 2ClarestaNo ratings yet
- Cushing's SyndromeDocument9 pagesCushing's Syndromemuzamiljoyia07No ratings yet
- Ep171905 CRDocument6 pagesEp171905 CRTantri SyahtiraNo ratings yet
- Cushing Syndrome 3Document5 pagesCushing Syndrome 3ClarestaNo ratings yet
- Pathophysiology of Endogenous Cushings SyndromeDocument1 pagePathophysiology of Endogenous Cushings SyndromeMcRo UndiNo ratings yet
- Unexpected Immunohistochemical Surprise of A Cushings Disease Macroadenoma Co-Expressing Acth and Prolactin: A Case ReportDocument5 pagesUnexpected Immunohistochemical Surprise of A Cushings Disease Macroadenoma Co-Expressing Acth and Prolactin: A Case ReportIJAR JOURNALNo ratings yet
- Singh2011 HIPERTENSIDocument5 pagesSingh2011 HIPERTENSILina RamadhaniNo ratings yet
- 4 EctDocument9 pages4 EctFebri Dwi HaryonoNo ratings yet
- SC Pediatrics and Review 2014Document5 pagesSC Pediatrics and Review 2014sheyla alegreNo ratings yet
- Cushing 'S Disease: Review Open AccessDocument9 pagesCushing 'S Disease: Review Open Accessmawarni siahaanNo ratings yet
- ACTH Treatment For Management of Nephrotic SyndromeDocument16 pagesACTH Treatment For Management of Nephrotic SyndromeCalvin Tanuwijaya Stick BolaNo ratings yet
- Cushing SyndromDocument12 pagesCushing SyndromIka AnisaNo ratings yet
- 299 309 PDFDocument11 pages299 309 PDFRovanNo ratings yet
- Congenital Adrenal Hyperplasia New Biomarkers and Adult TreatmentsDocument9 pagesCongenital Adrenal Hyperplasia New Biomarkers and Adult Treatmentsmiguel saba sabaNo ratings yet
- Diagnosis and Management of HemoptysisDocument11 pagesDiagnosis and Management of HemoptysisMita CantikayantiNo ratings yet
- Cushing Oxford 2022Document13 pagesCushing Oxford 2022mehidimed1889No ratings yet
- Cushing SyndromeDocument6 pagesCushing SyndromeSeren100% (1)
- CusingDocument7 pagesCusingmariahelenaneiNo ratings yet
- NIH Public Access: Author ManuscriptDocument13 pagesNIH Public Access: Author ManuscriptRohmantuah_Tra_1826No ratings yet
- Cushing TH 4Document13 pagesCushing TH 4syaymaNo ratings yet
- Hormonal Therapies in Septic Shock: Review ArticleDocument8 pagesHormonal Therapies in Septic Shock: Review ArticleJhon3xNo ratings yet
- Causes and Pathophysiology of Cushing Syndrome - UpToDateDocument18 pagesCauses and Pathophysiology of Cushing Syndrome - UpToDatecuentaparatrabajosdelau10No ratings yet
- Hipopituitarismo Lectura Motivadora1)Document13 pagesHipopituitarismo Lectura Motivadora1)Daniela Romero RiosNo ratings yet
- Cyclic Cushing 'S Syndrome - A Diagnostic ChallengeDocument7 pagesCyclic Cushing 'S Syndrome - A Diagnostic ChallengeAndri AffandiNo ratings yet
- The Pathophysiology and Treatment of Hypertension in Patients With Cushing's SyndromeDocument9 pagesThe Pathophysiology and Treatment of Hypertension in Patients With Cushing's Syndromedesak indryNo ratings yet
- Causes and Pathophysiology of Cushing's SyndromeDocument22 pagesCauses and Pathophysiology of Cushing's SyndromeGuardito PequeñoNo ratings yet
- Tanpa JudulDocument14 pagesTanpa JudulAsrapia HubaisyingNo ratings yet
- Management of Cushing Syndrome in Children and Adolescents Experience of A Single Tertiary CentreDocument10 pagesManagement of Cushing Syndrome in Children and Adolescents Experience of A Single Tertiary CentreTriratna FauziahNo ratings yet
- МС сист воспалениеDocument19 pagesМС сист воспалениеYulianaNo ratings yet
- Httpsinnovareacademics Injournalsindex Phpijppsarticledownload2221213586Document3 pagesHttpsinnovareacademics Injournalsindex Phpijppsarticledownload2221213586Gusti Ayu Sattwika PramitaNo ratings yet
- CT and MRI of Adrenal Gland PathologiesDocument23 pagesCT and MRI of Adrenal Gland PathologiesClaudia IrimieNo ratings yet
- Ectopic and Abnormal Hormonal Receptors in Adrenal Cushings SyndromeDocument36 pagesEctopic and Abnormal Hormonal Receptors in Adrenal Cushings SyndromePranitha PaidiNo ratings yet
- Cushing Síndrome - Old and New GenesDocument12 pagesCushing Síndrome - Old and New GenesDrasmNo ratings yet
- Cushings SyndromeDocument18 pagesCushings SyndromeBijay SharmaNo ratings yet
- SDL 10 BMS16091064Document5 pagesSDL 10 BMS16091064Jonathan YeohNo ratings yet
- Best Practice & Research Clinical Endocrinology & MetabolismDocument15 pagesBest Practice & Research Clinical Endocrinology & MetabolismFernanda M. SoberonNo ratings yet
- Week 5 Endokrin WO - Michael GeraldilDocument5 pagesWeek 5 Endokrin WO - Michael GeraldilMichael GNo ratings yet
- Pituitary Apoplexy Pathophysiology Diagnosis and MDocument6 pagesPituitary Apoplexy Pathophysiology Diagnosis and MlathifatulNo ratings yet
- Inflammatory Signaling in Hypertension: Regulation of Adrenal Catecholamine BiosynthesisDocument25 pagesInflammatory Signaling in Hypertension: Regulation of Adrenal Catecholamine Biosynthesisfaisal amirNo ratings yet
- Pasireotide ScihubDocument12 pagesPasireotide ScihubFelicia SanduțaNo ratings yet
- Best Practice & Research Clinical Endocrinology & MetabolismDocument13 pagesBest Practice & Research Clinical Endocrinology & MetabolismAhmad Harissul IbadNo ratings yet
- Adrenal Function: Adrenocorticotropic HormoneDocument11 pagesAdrenal Function: Adrenocorticotropic HormonehansenNo ratings yet
- Absolute Proof of Marijuana's Critical Medical Value in The Treatment of Conn's SyndromeDocument6 pagesAbsolute Proof of Marijuana's Critical Medical Value in The Treatment of Conn's Syndrome420infoNo ratings yet
- Dermatology: RoundsDocument6 pagesDermatology: RoundsPin Wijaya100% (1)
- Coexistence of Cushing Disease With A Solitary Adrenocor - 2022 - AACE ClinicalDocument4 pagesCoexistence of Cushing Disease With A Solitary Adrenocor - 2022 - AACE ClinicalMohammed Shuaib AhmedNo ratings yet
- Cushing SyndromeDocument1 pageCushing SyndromeAk62442No ratings yet
- Sindrome de CushingDocument15 pagesSindrome de CushingJakeline Salcedo MarquezNo ratings yet
- Cushing's Syndrome: A Structured Short-And Long-Term Management Plan For Patients in RemissionDocument14 pagesCushing's Syndrome: A Structured Short-And Long-Term Management Plan For Patients in RemissionmariahelenaneiNo ratings yet
- Literature AbdoDocument20 pagesLiterature AbdothestaffforpediatricptNo ratings yet
- Epidemiology and Clinical Manifestations of Cushing Syndrome - UpToDateDocument34 pagesEpidemiology and Clinical Manifestations of Cushing Syndrome - UpToDatemanudelvalleramirez021No ratings yet
- Newell Price2006Document13 pagesNewell Price2006fkia2013No ratings yet
- 1 s2.0 S1752928X23000483 MainDocument6 pages1 s2.0 S1752928X23000483 MainHtet AhkarNo ratings yet
- Cyclic Cushing'sDocument8 pagesCyclic Cushing'sMaryONo ratings yet
- Ectopic Production of Anti Diuretic HormoneDocument2 pagesEctopic Production of Anti Diuretic HormoneSurya Michael ChanceNo ratings yet
- Fast Facts: Blastic Plasmacytoid Dendritic Cell Neoplasm: Shedding light on a rare diseaseFrom EverandFast Facts: Blastic Plasmacytoid Dendritic Cell Neoplasm: Shedding light on a rare diseaseNo ratings yet
- ANZ Journal of Surgery - 2001 - Rankin - Costs of Accessing Surgical Specialists by Rural and Remote ResidentsDocument4 pagesANZ Journal of Surgery - 2001 - Rankin - Costs of Accessing Surgical Specialists by Rural and Remote ResidentsJeff CrocombeNo ratings yet
- Medical Journal of Australia - 2024 - Paynter - The Provision of General Surgery in Rural Australia A Narrative ReviewDocument6 pagesMedical Journal of Australia - 2024 - Paynter - The Provision of General Surgery in Rural Australia A Narrative ReviewJeff CrocombeNo ratings yet
- 8 PaediatricsDocument74 pages8 PaediatricsJeff CrocombeNo ratings yet
- Pboenix - Moral InjuryDocument28 pagesPboenix - Moral InjuryJeff CrocombeNo ratings yet
- COPD Stepwise DigitalDocument1 pageCOPD Stepwise DigitalJeff CrocombeNo ratings yet
- Congenital Adrenal Hyperplasia Due To Steroid 21-Hydroxylase Deficiency: An Endocrine Society Clinical Practice GuidelineDocument28 pagesCongenital Adrenal Hyperplasia Due To Steroid 21-Hydroxylase Deficiency: An Endocrine Society Clinical Practice GuidelineJeff CrocombeNo ratings yet
- Congenital Adrenal Hyperplasia-Current Insights in Pathophysiology, Diagnostics, and ManagementDocument69 pagesCongenital Adrenal Hyperplasia-Current Insights in Pathophysiology, Diagnostics, and ManagementJeff CrocombeNo ratings yet
- ACS Guidelines Long Presentation 2016 v2 1Document33 pagesACS Guidelines Long Presentation 2016 v2 1Jeff CrocombeNo ratings yet
- Effective Communication in HealthcareDocument1 pageEffective Communication in HealthcareJeff CrocombeNo ratings yet
- Congenital Adrenal HyperplasiaDocument17 pagesCongenital Adrenal HyperplasiaJeff CrocombeNo ratings yet
- ACRRM Social Media GuidelinesDocument16 pagesACRRM Social Media GuidelinesJeff CrocombeNo ratings yet
- AMA Conflict of Interest PolicyDocument4 pagesAMA Conflict of Interest PolicyJeff CrocombeNo ratings yet
- Designing Safer Health CareDocument4 pagesDesigning Safer Health CareJeff CrocombeNo ratings yet
- Soal Ujian EndokrineDocument5 pagesSoal Ujian EndokrineRivaldi0% (1)
- Endo Lect-Ant Pituitary GlandDocument18 pagesEndo Lect-Ant Pituitary GlanddoctorrfarrukhNo ratings yet
- Chap 31 HWDocument12 pagesChap 31 HWizabelaNo ratings yet
- Hemorragic CystDocument14 pagesHemorragic CystNyoman TapayanaNo ratings yet
- Occupational Health Status of Workers Exposed To Female Hormones in A Pharmaceutical PlantDocument6 pagesOccupational Health Status of Workers Exposed To Female Hormones in A Pharmaceutical Plantprom80117No ratings yet
- Family Planning and ContraceptionDocument11 pagesFamily Planning and ContraceptionJose Emmanuel Ribaya RuivivarNo ratings yet
- Science 10 A2.2 Pituitary and Hypothalamus The Bodys Control CentersDocument40 pagesScience 10 A2.2 Pituitary and Hypothalamus The Bodys Control CentersKhobie PabilicoNo ratings yet
- Investigatii ParacliniceDocument3 pagesInvestigatii ParaclinicebobcristibobNo ratings yet
- Unit 7 Diabetes Student ResourcesDocument7 pagesUnit 7 Diabetes Student ResourcesScribdNo ratings yet
- SynthroidDocument1 pageSynthroidCassieNo ratings yet
- Family Planning Personal NotesDocument4 pagesFamily Planning Personal NotesOB-GYNE DEPARTMENTNo ratings yet
- Dr. House-General Surgery QsDocument15 pagesDr. House-General Surgery QsYoussef Refaat RaoofNo ratings yet
- Cronic Kidney Disease: Prof. Dr. Agus Tessy SP - PD KGH Systema UrologiDocument39 pagesCronic Kidney Disease: Prof. Dr. Agus Tessy SP - PD KGH Systema UrologifauziyahabidahNo ratings yet
- Endocrinology - Adult and PediatricDocument17 pagesEndocrinology - Adult and PediatricipkNo ratings yet
- Hyperparathyrodism Hypoparathyrodism: Dr. A. Wahyudi Pababbari, SPPD, FinasimDocument48 pagesHyperparathyrodism Hypoparathyrodism: Dr. A. Wahyudi Pababbari, SPPD, FinasimKahfiyahNo ratings yet
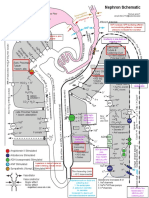
- Chronic Kidney Disease: A. Pathophysiology A. Schematic DiagramDocument3 pagesChronic Kidney Disease: A. Pathophysiology A. Schematic DiagramDaniel GeduquioNo ratings yet
- Endocrine SystemDocument24 pagesEndocrine Systemapi-290318217No ratings yet
- Performance Task 7 CCHMDocument3 pagesPerformance Task 7 CCHMHANNA CASANDRA GARCIANo ratings yet
- Coreection Du TD D'anglais 21-22Document13 pagesCoreection Du TD D'anglais 21-22Issouf BertheNo ratings yet
- Group 3 - PCOS and SD Written OutputDocument25 pagesGroup 3 - PCOS and SD Written OutputJolly S. SendinNo ratings yet
- @medicalbook - Store 2020reDocument203 pages@medicalbook - Store 2020reAhmad FitriawanNo ratings yet
- GlycosuriaDocument3 pagesGlycosuriaPavithra GurumurthyNo ratings yet
- NephronMap Copy2Document1 pageNephronMap Copy2Anonymous KxwaMDhANo ratings yet
- Trivia About The Human Reproductive SystemDocument13 pagesTrivia About The Human Reproductive SystemJohn Paul IloNo ratings yet
- PEX 09 06kkDocument4 pagesPEX 09 06kkRhirin Jiehh100% (2)