You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Ground Power Unit: GA ModelDocument17 pagesGround Power Unit: GA ModelAngelica Nava0% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Littelfuse EVI EV Charging Infrastructure Presentation PDFDocument19 pagesLittelfuse EVI EV Charging Infrastructure Presentation PDFRaka Pratindy100% (1)
- Basic SCBA: Self-Contained Breathing ApparatusDocument51 pagesBasic SCBA: Self-Contained Breathing ApparatusPaoloFregonaraNo ratings yet
- Sarmatian Swords 2 - ROMECDocument12 pagesSarmatian Swords 2 - ROMECkulcsarv100% (2)
- Evaluation of Pain Medicine CourseDocument2 pagesEvaluation of Pain Medicine CourseMoustafa MohamedNo ratings yet
- Top Ten Pearls For Successful Hip ArthrosDocument10 pagesTop Ten Pearls For Successful Hip ArthrosMoustafa MohamedNo ratings yet
- Proximal Anterolateral Accessory Portal Use Improves Peripheral Compartment Access and Capsular Management With T-CapsulotomyDocument5 pagesProximal Anterolateral Accessory Portal Use Improves Peripheral Compartment Access and Capsular Management With T-CapsulotomyMoustafa MohamedNo ratings yet
- Arthroscopic Synovectomy of The Hip Joint: The Regional Surgical TechniqueDocument7 pagesArthroscopic Synovectomy of The Hip Joint: The Regional Surgical TechniqueMoustafa MohamedNo ratings yet
- Outside-In Capsulotomy of The Hip For Arthroscopic Pincer ResectionDocument6 pagesOutside-In Capsulotomy of The Hip For Arthroscopic Pincer ResectionMoustafa MohamedNo ratings yet
- Arthroscopic Elbow Debridement Using Anterocentral Transbrachialis PortalDocument6 pagesArthroscopic Elbow Debridement Using Anterocentral Transbrachialis PortalMoustafa MohamedNo ratings yet
- Line of Image in Elbow ArthrosDocument3 pagesLine of Image in Elbow ArthrosMoustafa MohamedNo ratings yet
- Arthroscopic "Panorama" View of The Subacromial Space Via Deltoid Fascia ReleaseDocument5 pagesArthroscopic "Panorama" View of The Subacromial Space Via Deltoid Fascia ReleaseMoustafa MohamedNo ratings yet
- Arthroscopic Arthrolysis of Stiff ElbowDocument5 pagesArthroscopic Arthrolysis of Stiff ElbowMoustafa MohamedNo ratings yet
- Anatomical Arthroscopic Graft Reconstruction of The Anterior Tibiofibular Ligament For Chronic Disruption of The Distal SyndesmosisDocument5 pagesAnatomical Arthroscopic Graft Reconstruction of The Anterior Tibiofibular Ligament For Chronic Disruption of The Distal SyndesmosisMoustafa MohamedNo ratings yet
- Equipment: MR 51 / MR 51V42 - Handy Power MR 56 / MR 56V42 - Strong PowerDocument4 pagesEquipment: MR 51 / MR 51V42 - Handy Power MR 56 / MR 56V42 - Strong PowerIsmailBelguithNo ratings yet
- Poisson, Poisson-Gamma and Zero-Inflated Regression ModelsDocument43 pagesPoisson, Poisson-Gamma and Zero-Inflated Regression ModelszohrehNo ratings yet
- Herpes Simplex KeratitisDocument20 pagesHerpes Simplex KeratitisriskhapangestikaNo ratings yet
- Jotafloor: Traffic Deck SystemDocument12 pagesJotafloor: Traffic Deck SystemUnited Construction Est. TechnicalNo ratings yet
- Class XL (The Portrait of A Lady)Document7 pagesClass XL (The Portrait of A Lady)tmoNo ratings yet
- Temba KauDocument50 pagesTemba KaufauzanNo ratings yet
- 1cobalt Is An Element in Period 4 of The Periodic TableDocument3 pages1cobalt Is An Element in Period 4 of The Periodic TableZigla MooreNo ratings yet
- International StandardDocument8 pagesInternational Standardnazrul islamNo ratings yet
- Business, Government & Society: Pawan Kumar N K 12301005Document8 pagesBusiness, Government & Society: Pawan Kumar N K 12301005Pawan NkNo ratings yet
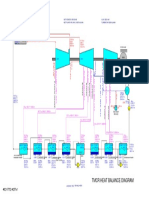
- 01 TMCR Heat Balance DiagramDocument1 page01 TMCR Heat Balance DiagramPrescila PalacioNo ratings yet
- Lecture-I Introduction To Concrete TechnologyDocument102 pagesLecture-I Introduction To Concrete Technologyjs kalyana rama100% (4)
- Idioms & PhrasesDocument4 pagesIdioms & PhrasesHimadri Prosad RoyNo ratings yet
- Freight ForwardingDocument43 pagesFreight ForwardingEuroline NtombouNo ratings yet
- Training Matrix Competency 4 Organic ConcoctionsDocument3 pagesTraining Matrix Competency 4 Organic ConcoctionsST. ISIDORE THE FARMERNo ratings yet
- Group 3 Aia ReportDocument26 pagesGroup 3 Aia ReportNAVAS E VNo ratings yet
- Spring Diameter of Spring Coil/cm Elastic Limit/n Spring Constant/nm-1 MaterialDocument4 pagesSpring Diameter of Spring Coil/cm Elastic Limit/n Spring Constant/nm-1 MaterialZahari Bin BakriNo ratings yet
- 300+ TOP Production and Operation Management MCQs & AnswersDocument14 pages300+ TOP Production and Operation Management MCQs & AnswersPranoy SarkarNo ratings yet
- 8000series Tech Datasheet 2018Document3 pages8000series Tech Datasheet 2018lucky414No ratings yet
- S800 SCL SR - 2CCC413009B0201 PDFDocument16 pagesS800 SCL SR - 2CCC413009B0201 PDFBalan PalaniappanNo ratings yet
- Ste FannyDocument17 pagesSte FannyElmer DE LA CruzNo ratings yet
- F5 BIG IP LTM 301A 301B Key Notes Feb 2023 1677506622Document63 pagesF5 BIG IP LTM 301A 301B Key Notes Feb 2023 1677506622MuhammadAbidHameedNo ratings yet
- Keeling 1960 PDFDocument4 pagesKeeling 1960 PDFErick AmâncioNo ratings yet
- MSC in Subsea Engineering - Flexible Pipe Analysis Lecture JP 2023Document67 pagesMSC in Subsea Engineering - Flexible Pipe Analysis Lecture JP 2023Fakey LaazNo ratings yet
- Recognizing and Classifying Daily Human Activities: Group-22Document23 pagesRecognizing and Classifying Daily Human Activities: Group-22Divyam GuptaNo ratings yet
- ER2 Manual 125kg 5t - 04Document144 pagesER2 Manual 125kg 5t - 04Muhammed ShamseerNo ratings yet
- Ecs C42iix Rev C Vit m2400 1Document36 pagesEcs C42iix Rev C Vit m2400 1Victor Pic100% (1)