You might also like
- The Performance Consultant's Fieldbook: Tools and Techniques for Improving Organizations and PeopleFrom EverandThe Performance Consultant's Fieldbook: Tools and Techniques for Improving Organizations and PeopleNo ratings yet
- Grade 7 TLE CUrriculum MapDocument19 pagesGrade 7 TLE CUrriculum MapMjoy Padayao100% (1)
- DTG 90 Days Jump Start ProgrammeDocument3 pagesDTG 90 Days Jump Start Programmeshafik jabbarNo ratings yet
- Reporting AssessmentDocument37 pagesReporting AssessmentWnc WestridgeNo ratings yet
- Monkayo College of Arts, Sciences and Technology A Local Government Unit of Monkayo Owned College Department of Business AdministrationDocument1 pageMonkayo College of Arts, Sciences and Technology A Local Government Unit of Monkayo Owned College Department of Business AdministrationElaineNo ratings yet
- Monthly Accomplishment Report On Learning and Development Interventions January - December 2019Document5 pagesMonthly Accomplishment Report On Learning and Development Interventions January - December 2019milk-bankNo ratings yet
- Mea BRTTH 2008Document1 pageMea BRTTH 2008quinaleNo ratings yet
- Temporary Training Permit For Foreign Medical PractitionerDocument3 pagesTemporary Training Permit For Foreign Medical PractitionerSamuel WibowoNo ratings yet
- IMS PRC 002 Suppliers Health Environmental QuestionnaireDocument2 pagesIMS PRC 002 Suppliers Health Environmental QuestionnaireJazmin Nicole PecundoNo ratings yet
- ERP Link: Erp - Aktu.ac - in (Mandatory)Document4 pagesERP Link: Erp - Aktu.ac - in (Mandatory)ANUJ KUMARNo ratings yet
- Nama Vendor: PT. Wahana Karsa Sinergi Manual and Procedure (Request To Vendor) Not To Be Copied Without Permision Job Order For Vendor OutsourcingDocument4 pagesNama Vendor: PT. Wahana Karsa Sinergi Manual and Procedure (Request To Vendor) Not To Be Copied Without Permision Job Order For Vendor OutsourcingAndre MahardhikaNo ratings yet
- County of Los Angeles Department of Mental HealthDocument1 pageCounty of Los Angeles Department of Mental Healthjeffrey_kingNo ratings yet
- AO - ICV - Forms CorrectedDocument14 pagesAO - ICV - Forms CorrectedFhebie Jevalyn DioayanNo ratings yet
- Sample Form: DNB - CardiologyDocument6 pagesSample Form: DNB - CardiologypradeephdNo ratings yet
- Business Case PepsicoDocument10 pagesBusiness Case PepsicoDaniel Azrael Gutiérrez NavaNo ratings yet
- 1 Template Mobilisation Plan Practice Merger 1Document9 pages1 Template Mobilisation Plan Practice Merger 1Ibrahem OmarNo ratings yet
- 5 PRC Resume of Resource Person Form2Document2 pages5 PRC Resume of Resource Person Form2Tago DinNo ratings yet
- Unit 4 - Lesson 1 SlidesDocument11 pagesUnit 4 - Lesson 1 SlidesNandi MliloNo ratings yet
- Training Requisition FormatDocument1 pageTraining Requisition FormatSGNo ratings yet
- ASM Quick Guide BookletDocument32 pagesASM Quick Guide BookletMoatiz RiazNo ratings yet
- Nepa BCDocument1 pageNepa BCDixit PhuyalNo ratings yet
- PMKVY Skill HubDocument1 pagePMKVY Skill HubAbir SenNo ratings yet
- Leo Cuarte Resume FinalDocument2 pagesLeo Cuarte Resume FinalMary Joy CabelNo ratings yet
- Elem WFP PPMP App Sob MDP Fy 2020Document108 pagesElem WFP PPMP App Sob MDP Fy 2020Phoeza Espinosa VillanuevaNo ratings yet
- Presentation Guidelines: Case Study - Zero Defect Drive by Laxmikant MishraDocument28 pagesPresentation Guidelines: Case Study - Zero Defect Drive by Laxmikant MishrapiyushNo ratings yet
- FORM 10 - Workplace Application Evaluation Tool (Updated)Document4 pagesFORM 10 - Workplace Application Evaluation Tool (Updated)Ahl LaynNo ratings yet
- TRAINING PLAN For MSEDocument58 pagesTRAINING PLAN For MSEMark MarasiganNo ratings yet
- Inquary 1Document1 pageInquary 1ranNo ratings yet
- Business Model Canvas + Innovation One Pager - GROUP 06Document3 pagesBusiness Model Canvas + Innovation One Pager - GROUP 06hathu.newindNo ratings yet
- Par Format For Physiotherapy of NHM OdishaDocument7 pagesPar Format For Physiotherapy of NHM Odishakrishna bptNo ratings yet
- Anen Joy R PTG Course 2 100071Document6 pagesAnen Joy R PTG Course 2 100071K BNo ratings yet
- PNC AA FO 25.9 Student Internship Training Plan For BS Marketing Management 20230320150744Document4 pagesPNC AA FO 25.9 Student Internship Training Plan For BS Marketing Management 20230320150744Alojado Lamuel Jesu ANo ratings yet
- Dce3115 Group 5 Sem 1 20212022Document9 pagesDce3115 Group 5 Sem 1 20212022Amir MuhamadNo ratings yet
- Republic of The Philippines Department of Labor and EmploymentDocument5 pagesRepublic of The Philippines Department of Labor and Employmentrenz naluminNo ratings yet
- Republic of The Philippines Department of Labor and EmploymentDocument5 pagesRepublic of The Philippines Department of Labor and EmploymentChokie BamNo ratings yet
- Unified Work Financial PlanDocument9 pagesUnified Work Financial PlanMarieta Alejo0% (1)
- SCHOOL NAME: - Proposed Date and Venue Materials Needed Budget Source Persons/ Offices Involved Expected OutcomesDocument4 pagesSCHOOL NAME: - Proposed Date and Venue Materials Needed Budget Source Persons/ Offices Involved Expected OutcomesJOLLYBEL GAJWAYENNo ratings yet
- Mar April 2022Document1,425 pagesMar April 2022Shai SdmpNo ratings yet
- Pharmacy Technician January 2023 - FINALDocument7 pagesPharmacy Technician January 2023 - FINALMasoomaIjazNo ratings yet
- Final Principle - 2 - GPHC - Action - PlanDocument5 pagesFinal Principle - 2 - GPHC - Action - Planc.tupakulaNo ratings yet
- RATSDocument3 pagesRATSAngelo Del RosarioNo ratings yet
- A Start Up of An Event Mamagement Firm: (IMBA First Year)Document21 pagesA Start Up of An Event Mamagement Firm: (IMBA First Year)NP's OfficialNo ratings yet
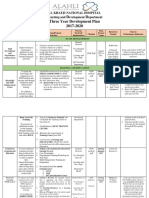
- L D D Three Year Development Plan 2017-2020: Al Khafji National Hospital Earning and Evelopment EpartmentDocument4 pagesL D D Three Year Development Plan 2017-2020: Al Khafji National Hospital Earning and Evelopment Epartmentprinsepejesse100% (3)
- CPD Activity Log Blank Template FinalDocument4 pagesCPD Activity Log Blank Template FinalKiranvarma KakarlapudiNo ratings yet
- Customer Journey MappingDocument117 pagesCustomer Journey Mappingrodger lutaloNo ratings yet
- Customer Journey Mapping: Guide For PractitionersDocument16 pagesCustomer Journey Mapping: Guide For PractitionersAngie Castro VivancoNo ratings yet
- Mereka Bentuk Kanvas Model Perniagaan SosialDocument12 pagesMereka Bentuk Kanvas Model Perniagaan SosialKapten LeeNo ratings yet
- PDP Blank Template FINALDocument4 pagesPDP Blank Template FINALSam NderituNo ratings yet
- PESO QuestionnaireDocument5 pagesPESO QuestionnairePj Norevlis0% (1)
- PGHR 5813 Talent Management Part 3 BCDocument10 pagesPGHR 5813 Talent Management Part 3 BCGlen KhuzwayoNo ratings yet
- Group 7 Homework Chap 7 Introduction To POMDocument8 pagesGroup 7 Homework Chap 7 Introduction To POMLâm NguyễnNo ratings yet
- System Family MSTP Ref: Contract Manager Issue: 01 Issue Date Approved By: M.Shenton Issued By: Iuliana Musat Page 1 of 2Document2 pagesSystem Family MSTP Ref: Contract Manager Issue: 01 Issue Date Approved By: M.Shenton Issued By: Iuliana Musat Page 1 of 2iuliaNo ratings yet
- SUPERVISE RICO 1. Training PlanDocument4 pagesSUPERVISE RICO 1. Training PlanKarlo AsicoNo ratings yet
- Training Needs Analysis Form: Professional Education, Training and Research OfficeDocument1 pageTraining Needs Analysis Form: Professional Education, Training and Research OfficeBGHMC SURGERYNo ratings yet
- Buzibr Ns Positions & Detailed Job Description: Please Refer To Audio Instructions Related To Each PositionDocument5 pagesBuzibr Ns Positions & Detailed Job Description: Please Refer To Audio Instructions Related To Each PositionShikha KumariNo ratings yet
- Pinamalayan Doctors' Hospital: Policies and ProcedureDocument7 pagesPinamalayan Doctors' Hospital: Policies and Procedurefredie rick luceNo ratings yet
- National Accreditation Board For Hospitals & Healthcare Providers (NABH) 4Document1 pageNational Accreditation Board For Hospitals & Healthcare Providers (NABH) 4bsndbh65wcNo ratings yet
- T.I: Número de IdentificaciónDocument1 pageT.I: Número de Identificaciónkaty MinaNo ratings yet
- Good Clinical Practice (GCP) Workshop 2019: Registration InformationDocument2 pagesGood Clinical Practice (GCP) Workshop 2019: Registration InformationAriff RazakNo ratings yet
- Cpdaero2021 01Document8 pagesCpdaero2021 01Renier Joseph Dela RosaNo ratings yet
- CHACHINGDocument6 pagesCHACHINGErika Jean Moyo ManzanillaNo ratings yet
- Lesson PlanDocument6 pagesLesson PlanErika Jean Moyo ManzanillaNo ratings yet
- Contempo Ass 3Document2 pagesContempo Ass 3Erika Jean Moyo ManzanillaNo ratings yet
- 4 21st Century Skills 1Document26 pages4 21st Century Skills 1Erika Jean Moyo ManzanillaNo ratings yet
- BTVTEd Pre Service Teachers Evaluation Sheet 2Document3 pagesBTVTEd Pre Service Teachers Evaluation Sheet 2Erika Jean Moyo ManzanillaNo ratings yet
- Ethics ReportDocument1 pageEthics ReportErika Jean Moyo ManzanillaNo ratings yet
- 5 Thefoundationalprinciple 140811230232 Phpapp01Document44 pages5 Thefoundationalprinciple 140811230232 Phpapp01Erika Jean Moyo ManzanillaNo ratings yet
- HAZARDSDocument3 pagesHAZARDSErika Jean Moyo ManzanillaNo ratings yet
- CG FSM 13 Meal Management 1 1 4Document4 pagesCG FSM 13 Meal Management 1 1 4Erika Jean Moyo ManzanillaNo ratings yet
- The Contemporary World: Katelyn M. Manzanilla Btvted FSM 1DDocument2 pagesThe Contemporary World: Katelyn M. Manzanilla Btvted FSM 1DErika Jean Moyo ManzanillaNo ratings yet
- Tle Household Services LasDocument2 pagesTle Household Services LasErika Jean Moyo ManzanillaNo ratings yet
- Lesson Plan ContingencyDocument6 pagesLesson Plan ContingencyErika Jean Moyo Manzanilla100% (1)
- Lesson Plan PPEDocument3 pagesLesson Plan PPEErika Jean Moyo ManzanillaNo ratings yet
- Erik Erikson's Psycho-Social Theory of DevelopmentDocument19 pagesErik Erikson's Psycho-Social Theory of DevelopmentJANE ESCAMILLAS100% (1)
- Neonatal PeriodDocument12 pagesNeonatal PeriodArsalan AhmedNo ratings yet
- CHCECE005 Theory TasksDocument30 pagesCHCECE005 Theory TasksChristina ChaiNo ratings yet
- Playground Safety Self Inspection ChecklistDocument1 pagePlayground Safety Self Inspection ChecklistYudha MaretaNo ratings yet
- Specific Objectives Learning Content Teaching Learning Activities Time Allotment Resources Evaluation ParametersDocument4 pagesSpecific Objectives Learning Content Teaching Learning Activities Time Allotment Resources Evaluation ParametersFrudz OrjalezaNo ratings yet
- mt3c Script 3 3 22Document4 pagesmt3c Script 3 3 22THIVYAN A/L MOHAN RAJ MoeNo ratings yet
- AU PAIR Interview QuestionsDocument2 pagesAU PAIR Interview QuestionsBeatriz Magno RodriguesNo ratings yet
- Month Questionnaire: Baby's NameDocument6 pagesMonth Questionnaire: Baby's NameKaterina DimovaNo ratings yet
- Internship Reflection Paper - 4 11Document7 pagesInternship Reflection Paper - 4 11api-538934593No ratings yet
- Infant Bathing ProcedureDocument6 pagesInfant Bathing ProcedureClaire RavagoNo ratings yet
- Erik Erikson's Stages of Psychosocial Development: American-German PsychologistDocument3 pagesErik Erikson's Stages of Psychosocial Development: American-German PsychologistMajoy TurcolasNo ratings yet
- Artifact 1 Anjie GbadeboDocument3 pagesArtifact 1 Anjie Gbadeboapi-595116860No ratings yet
- Ergonomics For Children: Designing Products and Places For Toddler To TeensDocument12 pagesErgonomics For Children: Designing Products and Places For Toddler To TeensJatmiko PrawiroNo ratings yet
- Hospitals Usa - ALDocument6 pagesHospitals Usa - ALAnshu ShindeNo ratings yet
- Đề thpt chuyên 2021-2022Document6 pagesĐề thpt chuyên 2021-2022Phương Thảo KimNo ratings yet
- Lesson I: The Child and Adolescent LearnersDocument41 pagesLesson I: The Child and Adolescent LearnersMa. Angelica Guillermo0% (1)
- Female Sexual Abuse: The Untold Story of Society's Last TabooDocument7 pagesFemale Sexual Abuse: The Untold Story of Society's Last TabooTaikoMotorNo ratings yet
- CHAPTER 8 SULLIVAN MyReviewerDocument7 pagesCHAPTER 8 SULLIVAN MyReviewerFrances LouiseNo ratings yet
- BCPCDocument13 pagesBCPCManhaters AtAllNo ratings yet
- Environmental Adaptations Example How/Why Does This Help?Document2 pagesEnvironmental Adaptations Example How/Why Does This Help?api-544801662No ratings yet
- Right Forms of VerbDocument6 pagesRight Forms of VerbMr Double RNo ratings yet
- Speech To Give On Childrens DayDocument2 pagesSpeech To Give On Childrens DayMarupakaNo ratings yet
- Small Children Big Cities Impact Through Design InterventionDocument68 pagesSmall Children Big Cities Impact Through Design InterventionBaabiMedNo ratings yet
- Paddington S Postcards Activity Pack 2022Document6 pagesPaddington S Postcards Activity Pack 2022jananijmiiNo ratings yet
- Socio-Emotional Development of Pre-SchoolerDocument22 pagesSocio-Emotional Development of Pre-SchoolerRichard RamosNo ratings yet
- Sentences Into The Correct and Meaningful ProcedureDocument15 pagesSentences Into The Correct and Meaningful Procedurepelajar bahasaNo ratings yet
- Synthesis Table For Final Project - DRDocument5 pagesSynthesis Table For Final Project - DRapi-533865716No ratings yet
- Erik Erikson'S Stages of Psychosocial Development: Saul McleodDocument7 pagesErik Erikson'S Stages of Psychosocial Development: Saul McleodMario AngNo ratings yet
- Being An Adult Is Not An Easy TaskDocument1 pageBeing An Adult Is Not An Easy Taskhazel100% (2)
- Early Childhood Care and Education in IndiaDocument22 pagesEarly Childhood Care and Education in IndiaMUNIRAH BINTI MADZLANNo ratings yet