You might also like
- Critical Appraisal On Systematic ReviewsDocument22 pagesCritical Appraisal On Systematic ReviewsDesiree MejicaNo ratings yet
- Effectiveness of relaxation therapy on stress and anxiety among caregiversDocument91 pagesEffectiveness of relaxation therapy on stress and anxiety among caregiverskalanidhi.RNo ratings yet
- Knowledge Attitudes and Barriers Towards Evidence Ba - 2017 - Hong Kong PhysioDocument9 pagesKnowledge Attitudes and Barriers Towards Evidence Ba - 2017 - Hong Kong PhysioAnuj ShandilyaNo ratings yet
- Does Simulation Booster Impact Retention of Resuscitation Procedural Skills and Teamwork?Document5 pagesDoes Simulation Booster Impact Retention of Resuscitation Procedural Skills and Teamwork?Choga Ilham ArlandoNo ratings yet
- Lecture 1 - IntroductionDocument58 pagesLecture 1 - IntroductionJames LittleNo ratings yet
- A, E. C. S. Maaruti College of Nursing: Role of Evidence Based Nursing Practice - Best PracticeDocument17 pagesA, E. C. S. Maaruti College of Nursing: Role of Evidence Based Nursing Practice - Best PracticeAnitha sujithNo ratings yet
- 5 HaniberniaDocument6 pages5 HaniberniaAnitha NoronhaNo ratings yet
- Evidence-Based Practice: Joslin John Assistant Professor Caritas College of NursingDocument30 pagesEvidence-Based Practice: Joslin John Assistant Professor Caritas College of NursingJOSLINNo ratings yet
- Role of Skill Laboratory Training in Medical Education - Students' PerspectiveDocument4 pagesRole of Skill Laboratory Training in Medical Education - Students' PerspectiveZuhalJanuarNo ratings yet
- 280 1361 2 PBDocument10 pages280 1361 2 PBAlejandroNo ratings yet
- Implementation and Evaluation of A Critical Care Nurse Fellowship ProgramDocument16 pagesImplementation and Evaluation of A Critical Care Nurse Fellowship ProgramMarc Andreo MalalaNo ratings yet
- He Clinical Integrative Puzzle For Teaching and Assessing Clinical Reasoning Preliminary Feasibility, Reliability, and Validity EvidenceDocument7 pagesHe Clinical Integrative Puzzle For Teaching and Assessing Clinical Reasoning Preliminary Feasibility, Reliability, and Validity EvidenceFrederico PóvoaNo ratings yet
- SAS 6 - Abapo, Aquea B.Document5 pagesSAS 6 - Abapo, Aquea B.Aquea Bernardo AbapoNo ratings yet
- Keyword:-Antenatal Examination, Skills, StudentsDocument3 pagesKeyword:-Antenatal Examination, Skills, StudentsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Research Strategy PDFDocument177 pagesResearch Strategy PDFpatientsafetyNo ratings yet
- Evidence Based Medicine Series: Part 3. Appraising The Evidence Are The Results Valid and Clinically Important?Document6 pagesEvidence Based Medicine Series: Part 3. Appraising The Evidence Are The Results Valid and Clinically Important?Ice Bear JJNo ratings yet
- Act 1 Research - GMDocument3 pagesAct 1 Research - GMBLACKPINK blink88No ratings yet
- Bringing research evidence into practiceDocument19 pagesBringing research evidence into practiceINdri Nur SutantiNo ratings yet
- The Effect of Clinical Skills Practice Modules on Nursing Students' Ability in Chest Physical ExaminationDocument6 pagesThe Effect of Clinical Skills Practice Modules on Nursing Students' Ability in Chest Physical ExaminationNanang FadliNo ratings yet
- Methodology - 2: Critical AppraisalDocument24 pagesMethodology - 2: Critical AppraisalrizqinapermatasariNo ratings yet
- Validity of Direct Ophthalmoscopy Skill Evaluation With Ocular Fundus Examination SimulatorsDocument5 pagesValidity of Direct Ophthalmoscopy Skill Evaluation With Ocular Fundus Examination SimulatorsWalisson BarbosaNo ratings yet
- Evidence-Based Review of Stroke RehabilitationDocument59 pagesEvidence-Based Review of Stroke RehabilitationJose Luis Miño CubillosNo ratings yet
- Lab Manual Psy 312l Group 3Document83 pagesLab Manual Psy 312l Group 3JAIRUS CAMBRONERO100% (1)
- Lab Manual - Psy 312l Group 3Document83 pagesLab Manual - Psy 312l Group 3JAIRUS CAMBRONERONo ratings yet
- Chapter 59 - Evidence Based Practi - 2016 - Hand and Upper Extremity RehabilitatDocument4 pagesChapter 59 - Evidence Based Practi - 2016 - Hand and Upper Extremity Rehabilitatjessica hongNo ratings yet
- Final Manuscript Group 1Document95 pagesFinal Manuscript Group 1Abby Shane FernandoNo ratings yet
- NMND 5103 Assignment 2Document49 pagesNMND 5103 Assignment 2Sithara JayatungaNo ratings yet
- Randomized Controlled TrialsDocument4 pagesRandomized Controlled TrialsIkromi SecondNo ratings yet
- Nurs702 Critique Final2Document9 pagesNurs702 Critique Final2natalie nodayNo ratings yet
- Christiana DissertationDocument36 pagesChristiana DissertationHezekiah AyubaNo ratings yet
- Pass MRCPCH with EBMDocument3 pagesPass MRCPCH with EBMHassan MohdNo ratings yet
- What Does Critical Appraisal MeanDocument32 pagesWhat Does Critical Appraisal Meanrahmat feryadiNo ratings yet
- 254-Article Text-822-1-10-20191016Document6 pages254-Article Text-822-1-10-20191016Aye Chan KyawNo ratings yet
- Evidence Based Practice - AllDocument81 pagesEvidence Based Practice - AllthestaffforpediatricptNo ratings yet
- Knowledge, Attitude and Barrier To Evidence-Based Practice Among Physiotherapists in Selected Districts of NepalDocument7 pagesKnowledge, Attitude and Barrier To Evidence-Based Practice Among Physiotherapists in Selected Districts of NepalfaizasaleemsameNo ratings yet
- Mosoiu Et Al 2023 Core Palliative Care Research Competencies Framework For Palliative Care CliniciansDocument10 pagesMosoiu Et Al 2023 Core Palliative Care Research Competencies Framework For Palliative Care CliniciansAmbaNo ratings yet
- Presentation 1Document22 pagesPresentation 1endahNo ratings yet
- Critical Appraisal TeachingDocument21 pagesCritical Appraisal TeachingAtika MusfirahNo ratings yet
- Syllabus For Courses Affiliated To The Kerala University of Health SciencesDocument124 pagesSyllabus For Courses Affiliated To The Kerala University of Health SciencesgoldaNo ratings yet
- Icm Course Syllabus PDFDocument8 pagesIcm Course Syllabus PDFZoya Morani100% (1)
- Module 2 Cardiopulmo PT Pulmonary Conditions and Pumonary PT AssessmentDocument6 pagesModule 2 Cardiopulmo PT Pulmonary Conditions and Pumonary PT AssessmentMichelle MatthewNo ratings yet
- International Journal of Nursing Studies: Rujun Hu, Huiming Gao, Yansheng Ye, Zhihong Ni, Ning Jiang, Xiaolian JiangDocument10 pagesInternational Journal of Nursing Studies: Rujun Hu, Huiming Gao, Yansheng Ye, Zhihong Ni, Ning Jiang, Xiaolian Jiangputu juniNo ratings yet
- Kerala University PB B.Sc Nursing SyllabusDocument123 pagesKerala University PB B.Sc Nursing SyllabusSwapna josephNo ratings yet
- Methods and Evaluation in Clinical and Counseling Psychology: Pergamon General Psychology SeriesFrom EverandMethods and Evaluation in Clinical and Counseling Psychology: Pergamon General Psychology SeriesRating: 4 out of 5 stars4/5 (1)
- Burger Allen Exercises pdf1Document133 pagesBurger Allen Exercises pdf1lucky 116No ratings yet
- Evidence Analysis Library Review of Best Practices For Performing Indirect Calorimetry in Healthy and NoneCritically Ill IndividualsDocument32 pagesEvidence Analysis Library Review of Best Practices For Performing Indirect Calorimetry in Healthy and NoneCritically Ill IndividualsNutricion Deportiva NutrainerNo ratings yet
- Paper Adulto MayorDocument6 pagesPaper Adulto MayorIgnacio Ibarra TorresNo ratings yet
- Mcqs TheraputicDocument1 pageMcqs TheraputicWasiq ChughtaiNo ratings yet
- Students' Perception About Small Group Teaching Techniques: Role Play Method and Case Based Learning in PharmacologyDocument6 pagesStudents' Perception About Small Group Teaching Techniques: Role Play Method and Case Based Learning in PharmacologyNurul Hikmatul QowiNo ratings yet
- Influence of Pranayama On Respiratory Function of Middle Age WomenDocument4 pagesInfluence of Pranayama On Respiratory Function of Middle Age WomenInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Tau Edu Gy MDDocument10 pagesTau Edu Gy MDkkanish1109No ratings yet
- SkyeDocument20 pagesSkyeapi-534884871No ratings yet
- Kabir ThesisDocument29 pagesKabir ThesisIHSAN ULLAHNo ratings yet
- K7 - Critical AppraisalDocument40 pagesK7 - Critical AppraisalFiqih IbrahimNo ratings yet
- Articlecritique Nreed Nurs531Document6 pagesArticlecritique Nreed Nurs531api-215994182No ratings yet
- Internship Report (747) 5Document32 pagesInternship Report (747) 5indian meme templatesNo ratings yet
- Keywords: - Anxiety, Relaxation Therapy, Epilepsy: PatientsDocument6 pagesKeywords: - Anxiety, Relaxation Therapy, Epilepsy: PatientsAnonymous izrFWiQNo ratings yet
- Clinical Sciences Diagnosis Laboratory Manual July 2008Document145 pagesClinical Sciences Diagnosis Laboratory Manual July 2008Michael KoontzNo ratings yet
- INACSLSOBPPast Present FutureDocument7 pagesINACSLSOBPPast Present FutureVictoriano MendezNo ratings yet
- Bienstock Simulation BasedTraining IJOP N1 2023Document17 pagesBienstock Simulation BasedTraining IJOP N1 2023Victoriano MendezNo ratings yet
- Health Science Students Attitude of Using Educational Simulation in SaudiDocument9 pagesHealth Science Students Attitude of Using Educational Simulation in SaudiVictoriano MendezNo ratings yet
- 1902JEMS Supp5 PDFDocument32 pages1902JEMS Supp5 PDFVictoriano MendezNo ratings yet
- Risk Based PPE Usage - EMS PPE Project PresentationDocument20 pagesRisk Based PPE Usage - EMS PPE Project PresentationVictoriano MendezNo ratings yet
- Jems201803 DLDocument68 pagesJems201803 DLVictoriano MendezNo ratings yet
- ACLS Rhythms For The ACLS Algorithms: AppendixDocument32 pagesACLS Rhythms For The ACLS Algorithms: Appendixyan_ricci19100% (4)
- Explorando La Suspension de La Incredulidad Durante El Aprendizaje Basado en Las SimulacionesDocument7 pagesExplorando La Suspension de La Incredulidad Durante El Aprendizaje Basado en Las SimulacionesVictoriano MendezNo ratings yet
- Stat Reasoning Homework 1 Hw1Document6 pagesStat Reasoning Homework 1 Hw1Victoriano Mendez0% (1)
- ACLS Full Lesson Plans PDFDocument60 pagesACLS Full Lesson Plans PDFVictoriano Mendez100% (1)
- Toc Is 5Document6 pagesToc Is 5Victoriano MendezNo ratings yet
- CASE and Experiential LearningDocument11 pagesCASE and Experiential LearningVictoriano MendezNo ratings yet
- Masking: Janet Holbrook, PHD, MPH Johns Hopkins UniversityDocument11 pagesMasking: Janet Holbrook, PHD, MPH Johns Hopkins UniversityVictoriano MendezNo ratings yet
- Equipment List: Equipment and Supplies Quantity Needed Learning/Testing Station Equipment NeededDocument3 pagesEquipment List: Equipment and Supplies Quantity Needed Learning/Testing Station Equipment NeededVictoriano MendezNo ratings yet
- Sim DictionaryDocument52 pagesSim DictionaryVictoriano MendezNo ratings yet
- Print Story - 6 Questions Medics Should Ask On Every Auto Accident Scene - EMS1Document1 pagePrint Story - 6 Questions Medics Should Ask On Every Auto Accident Scene - EMS1Victoriano MendezNo ratings yet
- Print Story - 6 Questions Medics Should Ask On Every Auto Accident Scene - EMS1Document1 pagePrint Story - 6 Questions Medics Should Ask On Every Auto Accident Scene - EMS1Victoriano MendezNo ratings yet
- Print Story - 5 Things Great EMS Supervisors Do Differently - EMS1Document2 pagesPrint Story - 5 Things Great EMS Supervisors Do Differently - EMS1Victoriano Mendez100% (1)
- Vital Signs: Pulse & Heart Rate: Video 1.1: Basic Heart AnatomyDocument10 pagesVital Signs: Pulse & Heart Rate: Video 1.1: Basic Heart AnatomyVictoriano MendezNo ratings yet
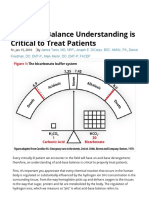
- Acid-Base Balance Understanding Is Critical To Treat Patients - Journal of Emergency Medical ServicesDocument11 pagesAcid-Base Balance Understanding Is Critical To Treat Patients - Journal of Emergency Medical ServicesVictoriano MendezNo ratings yet
- Wma Field ProtocolsDocument11 pagesWma Field ProtocolsVictoriano MendezNo ratings yet
- 101 Things We Should Teach Every New EMT 1) You..Document6 pages101 Things We Should Teach Every New EMT 1) You..Victoriano MendezNo ratings yet
- Print Story - Understanding The NFPA 1917 Ambulance Standard - EMS1Document2 pagesPrint Story - Understanding The NFPA 1917 Ambulance Standard - EMS1Victoriano MendezNo ratings yet
- Pi Is 1080603214001124Document16 pagesPi Is 1080603214001124Victoriano MendezNo ratings yet
- Print Story - Faith in EMS - My Karma Ran Over Your Dogma - EMS1Document2 pagesPrint Story - Faith in EMS - My Karma Ran Over Your Dogma - EMS1Victoriano MendezNo ratings yet
- Multipleintelligences PDFDocument3 pagesMultipleintelligences PDFnitinmisra77No ratings yet
- 02prehospitalcervicalspinalimmobilizationaftertrauma Neurosurgery2013 131114031805 Phpapp01Document13 pages02prehospitalcervicalspinalimmobilizationaftertrauma Neurosurgery2013 131114031805 Phpapp01Victoriano MendezNo ratings yet
- IFRC Yearly Security Report 2008Document16 pagesIFRC Yearly Security Report 2008Victoriano MendezNo ratings yet
- Using Knowledge Checks Throughout TrainingDocument1 pageUsing Knowledge Checks Throughout TrainingVictoriano MendezNo ratings yet
- Lesson 1 - Ielts Reading in GeneralDocument28 pagesLesson 1 - Ielts Reading in GeneralTrangNo ratings yet
- Grade 2 Semester 2 Rubric - TemplateDocument1 pageGrade 2 Semester 2 Rubric - Templatechris reidNo ratings yet
- Gateway A1+ Teacher's Resources UNIT 1 Everyday English Teacher's NotesDocument1 pageGateway A1+ Teacher's Resources UNIT 1 Everyday English Teacher's NotesоксанаNo ratings yet
- ITE 50 Chapter5Document61 pagesITE 50 Chapter5cralemanNo ratings yet
- Mid Year Topic 1 PacketDocument19 pagesMid Year Topic 1 PacketBadria KazimNo ratings yet
- Geometry Honors 2012-2013 Semester Exams Practice Materials Semester 1Document59 pagesGeometry Honors 2012-2013 Semester Exams Practice Materials Semester 1peachcrushNo ratings yet
- Performance Appraisal Study at Wheels IndiaDocument14 pagesPerformance Appraisal Study at Wheels IndiaKalidoss DossNo ratings yet
- Cultural Anthropology (Bonvillain)Document1,980 pagesCultural Anthropology (Bonvillain)Mel NonymusNo ratings yet
- Healthy Lunchbox IdeasDocument4 pagesHealthy Lunchbox IdeasdebbieNo ratings yet
- Gynaecological Surgery D BissonDocument36 pagesGynaecological Surgery D BissondrdeegeeNo ratings yet
- 04 Unit 5. Lesson 5Document11 pages04 Unit 5. Lesson 5barb knezNo ratings yet
- Co-Curricular Performance Verification and Classification FormDocument96 pagesCo-Curricular Performance Verification and Classification FormRobert Jun Serra GregoriosNo ratings yet
- Neighborhood MapDocument2 pagesNeighborhood MapswanniNo ratings yet
- CBSE Marksheet for NEHA RAJPUTDocument1 pageCBSE Marksheet for NEHA RAJPUTNikita RajputNo ratings yet
- Morgans WonderlandDocument4 pagesMorgans Wonderlandapi-533615424No ratings yet
- Final Educ 8Document40 pagesFinal Educ 8Ive EspiaNo ratings yet
- Sinead Marie MohanDocument1 pageSinead Marie Mohanapi-336654016No ratings yet
- Science 7 Structure and Forces - For MergeDocument15 pagesScience 7 Structure and Forces - For Mergeapi-353447897No ratings yet
- ANHS Senior High School Class ProgramDocument4 pagesANHS Senior High School Class Programapi-450904901No ratings yet
- Dny PDFDocument2 pagesDny PDFchetanNo ratings yet
- Table 2 of TMC501 Lesson 3 Go On Holiday (Prepared by Dr. Neo Kian Sen)Document4 pagesTable 2 of TMC501 Lesson 3 Go On Holiday (Prepared by Dr. Neo Kian Sen)Auni Akif AleesaNo ratings yet
- Sociological and Political Literary CriticismDocument48 pagesSociological and Political Literary Criticismmayel_mymnemosyneNo ratings yet
- Communicative Strategies ModuleDocument10 pagesCommunicative Strategies ModuleAgatha Sigrid GonzalesNo ratings yet
- Bugreport Lime - Global QKQ1.200830.002 2021 05 04 22 36 45 Dumpstate - Log 30853Document30 pagesBugreport Lime - Global QKQ1.200830.002 2021 05 04 22 36 45 Dumpstate - Log 30853Blackgouest 1043No ratings yet
- Nurse LifeDocument9 pagesNurse Lifeapi-310647920100% (1)
- Training Design & Matrix-DapsshiDocument11 pagesTraining Design & Matrix-Dapsshimharlit cagaananNo ratings yet
- Training Report FormatDocument8 pagesTraining Report FormatPrem PatelNo ratings yet
- Rubinstein-Taybi Syndrome Readiness For Toilet Training: Charlotte Mawby Independent Paediatric Continence Nurse May 2016Document50 pagesRubinstein-Taybi Syndrome Readiness For Toilet Training: Charlotte Mawby Independent Paediatric Continence Nurse May 2016vinaNo ratings yet
- Proceeding-SENIOR HIGHSCHOOL STUDENTS PROBLEMS IN WRITINGDocument5 pagesProceeding-SENIOR HIGHSCHOOL STUDENTS PROBLEMS IN WRITINGJae RastafuniaNo ratings yet
- DR M Saravanan, Asso Professor & HeadDocument19 pagesDR M Saravanan, Asso Professor & HeadMurugan SaravananNo ratings yet