You might also like
- OCR A Level Biology Content Year 2 Checklist 2016Document11 pagesOCR A Level Biology Content Year 2 Checklist 2016Billy thorntonNo ratings yet
- Harrison MCQ NephrologyDocument7 pagesHarrison MCQ Nephrologydrtpk80% (15)
- Nephrotic Nephritic SyndromeDocument15 pagesNephrotic Nephritic Syndromeshefalika mandremNo ratings yet
- Nephrotic and Nephritic SyndromeDocument52 pagesNephrotic and Nephritic SyndromeJessa MeaNo ratings yet
- Glomerulonephritis Medical Student Lecture 2Document67 pagesGlomerulonephritis Medical Student Lecture 2ibnbasheer100% (12)
- GLomerulus DiseaseDocument5 pagesGLomerulus DiseaseMEDS easyNo ratings yet
- Renal Block Lecture Four & Five Key Points on Nephrotic and Nephritic SyndromesDocument27 pagesRenal Block Lecture Four & Five Key Points on Nephrotic and Nephritic Syndromesafaq alismailiNo ratings yet
- Editing File: Recognizing Major Renal Glomerular SyndromesDocument22 pagesEditing File: Recognizing Major Renal Glomerular SyndromesmariapaulaguerrerocNo ratings yet
- PATH - Nephrotic SyndromeDocument11 pagesPATH - Nephrotic SyndromeTeshale TekleNo ratings yet
- 14 Kidney Diseases PDFDocument128 pages14 Kidney Diseases PDFMayur WakchaureNo ratings yet
- Amharic ConversationDocument94 pagesAmharic Conversationtsehay asratNo ratings yet
- Renal SystemDocument43 pagesRenal SystemYash SoniNo ratings yet
- PATHO Glomerular and Tubulointerstitial DiseaseDocument43 pagesPATHO Glomerular and Tubulointerstitial DiseaseHananya ManroeNo ratings yet
- Granuloma Is Defined As A Circumscribed, Tiny Lesion, About 1 MM in Diameter, Composed PredominantlyDocument6 pagesGranuloma Is Defined As A Circumscribed, Tiny Lesion, About 1 MM in Diameter, Composed PredominantlyIsak ShatikaNo ratings yet
- Understanding Glomerular Diseases: Nephritic vs Nephrotic SyndromesDocument127 pagesUnderstanding Glomerular Diseases: Nephritic vs Nephrotic SyndromesCoy NuñezNo ratings yet
- L20 - Glomerular DiseasesDocument34 pagesL20 - Glomerular Diseasesabdideba6No ratings yet
- Glomerular Diseases: Ass - Prof. Rihab Al-Mudhaffer Kufa University Department of Pathology and Forensic MedicineDocument37 pagesGlomerular Diseases: Ass - Prof. Rihab Al-Mudhaffer Kufa University Department of Pathology and Forensic MedicineAli HusseinNo ratings yet
- Pathology of Urinary SystemDocument384 pagesPathology of Urinary SystemNzau MuangeNo ratings yet
- 3.leprosy 2Document119 pages3.leprosy 2Manuhe TsegaNo ratings yet
- Leprosy Internal MEDDocument11 pagesLeprosy Internal MEDAhmed Gh Al-zechrawiNo ratings yet
- Glomerular Diseases My NotesDocument5 pagesGlomerular Diseases My Notesmalar_km43No ratings yet
- Patologi GinjalDocument94 pagesPatologi GinjalDenoNo ratings yet
- Renal pathology-1 (Glomerulonephritis)-2021 (1)Document15 pagesRenal pathology-1 (Glomerulonephritis)-2021 (1)oziad4518No ratings yet
- Centro Escolar University: School of Medicine SY 2018-2019 Urinary Tract - Glomerulus October 28, 2018Document78 pagesCentro Escolar University: School of Medicine SY 2018-2019 Urinary Tract - Glomerulus October 28, 2018Kim RamosNo ratings yet
- Imunosupresan For Treatment of Nephrotic Syndrome DR Harnavi HarunDocument27 pagesImunosupresan For Treatment of Nephrotic Syndrome DR Harnavi HarunM Ivan Pratama ZebuaNo ratings yet
- 3&4 Glomerular Diseases and Nephrotic SyndromeDocument46 pages3&4 Glomerular Diseases and Nephrotic SyndromeTor Koang ThorNo ratings yet
- Topic 3Document17 pagesTopic 3Jacqueline Tungcul DonatoNo ratings yet
- UTI Dan Glomerular DiseaseDocument58 pagesUTI Dan Glomerular DiseaseLiana Ika SuwandyNo ratings yet
- Aubf RenaallllllllDocument7 pagesAubf RenaallllllllMarienel PingolNo ratings yet
- Leprosy: DR L F WentzelDocument5 pagesLeprosy: DR L F WentzelCitie VillaNo ratings yet
- Glomerular Diseases: Membrano Proliferative Glomerulonephritis (MPGN) - in This LectureDocument12 pagesGlomerular Diseases: Membrano Proliferative Glomerulonephritis (MPGN) - in This LectureWalaa abo foolNo ratings yet
- Glomerulonephritis Guide for International StudentsDocument43 pagesGlomerulonephritis Guide for International StudentsNosirova ManijaNo ratings yet
- NEPHROTIC SYNDROME - HamidDocument20 pagesNEPHROTIC SYNDROME - HamidAbdul Hamid OmarNo ratings yet
- Leprosy 2023Document55 pagesLeprosy 2023Obatoye SeyiNo ratings yet
- Renal Biopsy Pathology 2011Document10 pagesRenal Biopsy Pathology 2011AnamNo ratings yet
- 2 Glomerular DiseasesDocument48 pages2 Glomerular DiseasesDammaqsaa W BiyyanaaNo ratings yet
- Renal Diseases IDocument17 pagesRenal Diseases IPoojaNo ratings yet
- Circulating KineticsDocument82 pagesCirculating KineticsJilycamae COSMODNo ratings yet
- Glomerular Diseases-Part 1Document68 pagesGlomerular Diseases-Part 1hrg79qzwc2No ratings yet
- III. Irreversible Cell Injury (Cell Death)Document42 pagesIII. Irreversible Cell Injury (Cell Death)Manal ElnemrNo ratings yet
- Glomerulonephritis: Prof DR DR Haerani Rasyid, Mkes, SPPD, KGH, SPGK Tim Ginjal Hipertensi Unhas 2019Document68 pagesGlomerulonephritis: Prof DR DR Haerani Rasyid, Mkes, SPPD, KGH, SPGK Tim Ginjal Hipertensi Unhas 2019uzan100% (1)
- Kidney Biopsy Guide to Glomerular PathologyDocument78 pagesKidney Biopsy Guide to Glomerular PathologyGalih AryyagunawanNo ratings yet
- Nephrotic synd (2)Document21 pagesNephrotic synd (2)238439904No ratings yet
- Nephrotic Syndrome in Adults Role of RituximabDocument50 pagesNephrotic Syndrome in Adults Role of RituximabJoel KennedyNo ratings yet
- WBC Anomalies GuideDocument20 pagesWBC Anomalies GuideJosephine Piedad100% (1)
- @acute Nephritic SyndromeDocument3 pages@acute Nephritic SyndromeMazlia FarzanaNo ratings yet
- AMYLOIDOSISDocument16 pagesAMYLOIDOSISSourav NathNo ratings yet
- Patho 5Document8 pagesPatho 5ambiliNo ratings yet
- Chapter 18 Urinary System (2nd Edition)Document55 pagesChapter 18 Urinary System (2nd Edition)Abhi KarmakarNo ratings yet
- Glomerular DiseasesDocument92 pagesGlomerular Diseasesfrankozed1No ratings yet
- Renal Injury Patterns: Clinical Syndromes and Structural AbnormalitiesDocument93 pagesRenal Injury Patterns: Clinical Syndromes and Structural AbnormalitiesMarga KouryNo ratings yet
- PATH - Nephritic SyndromeDocument14 pagesPATH - Nephritic SyndromeMuhamad Zul ImanNo ratings yet
- Renal Diseases - BSMLS OLFUDocument15 pagesRenal Diseases - BSMLS OLFUMitch IbayNo ratings yet
- Medical KidneyDocument13 pagesMedical KidneyJose SirittNo ratings yet
- Glomdis - GanlinDocument118 pagesGlomdis - GanlinMEDS easyNo ratings yet
- Morpho - Pathology Final Summary: Chapter 1: Cellular Reactions To AggressionDocument21 pagesMorpho - Pathology Final Summary: Chapter 1: Cellular Reactions To Aggressiondjxela89No ratings yet
- Miscellaneous Renal DiseaseDocument12 pagesMiscellaneous Renal DiseaseMusfian AgungNo ratings yet
- Presentation 1Document38 pagesPresentation 1Asty ModheNo ratings yet
- Granulomatous Lesions of Oral CavityDocument120 pagesGranulomatous Lesions of Oral CavityMadhura ShekatkarNo ratings yet
- Glomerular DiseaseDocument24 pagesGlomerular DiseasemadhuNo ratings yet
- Miscellaneous Conditions: Granulomatous Liver Disease Description and CausesDocument23 pagesMiscellaneous Conditions: Granulomatous Liver Disease Description and Causesputri riszaNo ratings yet
- Multiple Sclerosis, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandMultiple Sclerosis, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Hypoxic Ischaemic Encephalopathy HIE AsphyxiaDocument6 pagesHypoxic Ischaemic Encephalopathy HIE AsphyxiaCaity YoungNo ratings yet
- Rhumatologie-Pediatrique FRDocument4 pagesRhumatologie-Pediatrique FRCaity YoungNo ratings yet
- Fluid Calculator DKADocument3 pagesFluid Calculator DKACaity YoungNo ratings yet
- Afoem Sample Paper Stage B Written Exam Paper 7Document46 pagesAfoem Sample Paper Stage B Written Exam Paper 7Caity YoungNo ratings yet
- Afoem Sample Paper Stage B Written Exam Paper 7Document46 pagesAfoem Sample Paper Stage B Written Exam Paper 7Caity YoungNo ratings yet
- Afoem Sample Paper Stage B Written Exam Paper 7Document43 pagesAfoem Sample Paper Stage B Written Exam Paper 7Caity YoungNo ratings yet
- A I - E M: Drenal Nsufficiency Mergency AnagementDocument12 pagesA I - E M: Drenal Nsufficiency Mergency AnagementCaity YoungNo ratings yet
- SSHADESS HandoutDocument1 pageSSHADESS HandoutCaity YoungNo ratings yet
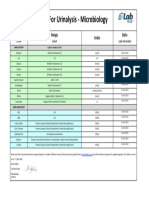
- Reference Ranges For Urinalysis - Microbiology: Test Range Units DateDocument1 pageReference Ranges For Urinalysis - Microbiology: Test Range Units DateCaity YoungNo ratings yet
- 2 - McDonald - Examples - of - Unhelpful - ThoughtsDocument2 pages2 - McDonald - Examples - of - Unhelpful - ThoughtsCaity YoungNo ratings yet
- Correspondence: Classifi Cation of CFTR Mutation ClassesDocument2 pagesCorrespondence: Classifi Cation of CFTR Mutation ClassesCaity YoungNo ratings yet
- 2014 A Health Professionals Guide To Using The ChartsDocument14 pages2014 A Health Professionals Guide To Using The ChartsCaity YoungNo ratings yet
- Tic Disorder LeafletDocument2 pagesTic Disorder LeafletAndreia SilvaNo ratings yet
- Applied Knowledge in Paediatrics - MRCPCH Mastercourse Cardiology - ClinicalKeyDocument8 pagesApplied Knowledge in Paediatrics - MRCPCH Mastercourse Cardiology - ClinicalKeyCaity YoungNo ratings yet
- Part 2: Male Reproductive System: Normal Physiology and StructureDocument30 pagesPart 2: Male Reproductive System: Normal Physiology and StructureCaity YoungNo ratings yet
- Genetic Basis For Congenital Heart Disease: Revisited: CirculationDocument59 pagesGenetic Basis For Congenital Heart Disease: Revisited: CirculationCaity YoungNo ratings yet
- ToF ScriptDocument6 pagesToF ScriptCaity YoungNo ratings yet
- Sore Throat: Navigating The Differential DiagnosisDocument7 pagesSore Throat: Navigating The Differential DiagnosisCaity YoungNo ratings yet
- Dink in 2014Document24 pagesDink in 2014Okta Kurniawan SaputraNo ratings yet
- IsbelDocument7 pagesIsbelCaity YoungNo ratings yet
- Urine Formation: Joanna I. Alafag Adv. Animal Physiology Feb. 13, 2020Document64 pagesUrine Formation: Joanna I. Alafag Adv. Animal Physiology Feb. 13, 2020Tyron Cadiz LopezNo ratings yet
- Renal Cell CarcinomaDocument9 pagesRenal Cell CarcinomaSahirNo ratings yet
- Singapore Ichlsr ProceedingsDocument23 pagesSingapore Ichlsr ProceedingsGlobal Research and Development ServicesNo ratings yet
- IVMS Cell Biology and Pathology Flash Facts 2Document3,980 pagesIVMS Cell Biology and Pathology Flash Facts 2Marc Imhotep Cray, M.D.No ratings yet
- Rowatinex®: Gastro-Resistant Capsules, SoftDocument3 pagesRowatinex®: Gastro-Resistant Capsules, SoftAbdirisak Aar ChannelNo ratings yet
- Chapter 7. The Excretory System: Short QuestionsDocument23 pagesChapter 7. The Excretory System: Short QuestionsAshwieen Kumar PradhanNo ratings yet
- Tanveer Notes Revised 1st ED (Uploaded by Hanan)Document102 pagesTanveer Notes Revised 1st ED (Uploaded by Hanan)jawad100% (4)
- Lab Physiology Urine 1Document13 pagesLab Physiology Urine 1Abdullah AzadzoyNo ratings yet
- Metabolic Wastes and Excretion in the Urinary SystemDocument20 pagesMetabolic Wastes and Excretion in the Urinary SystemQazi QaziNo ratings yet
- 9th Biology Lesson PlanDocument40 pages9th Biology Lesson PlanMudassir HussainNo ratings yet
- MCNP Integrated Concepts NP 4Document11 pagesMCNP Integrated Concepts NP 4Karen Mae Santiago AlcantaraNo ratings yet
- Urea 501Document5 pagesUrea 501hairiNo ratings yet
- Revisiting Diuretic Choice in Chronic Kidney.4Document8 pagesRevisiting Diuretic Choice in Chronic Kidney.4FABIO JAVIER BRAVO SALDARRIAGANo ratings yet
- #1 Anatomi Fisiologi Urogenital SystemDocument4 pages#1 Anatomi Fisiologi Urogenital SystemNur azriyati PutriNo ratings yet
- Urologic Stone Disease 2005Document51 pagesUrologic Stone Disease 2005jamilNo ratings yet
- Acute Poststreptococcal Glomerulonephritis (Apsgn) in ChildrenDocument22 pagesAcute Poststreptococcal Glomerulonephritis (Apsgn) in ChildrenOlivia PutriNo ratings yet
- HYPOKALEMIA) ReportDocument72 pagesHYPOKALEMIA) ReportFairoz Macud AdapNo ratings yet
- Drug InteractionDocument27 pagesDrug InteractionRida Nur RafidahNo ratings yet
- Nursing Test 3 (NP Ii)Document16 pagesNursing Test 3 (NP Ii)Yuxin LiuNo ratings yet
- Evaluating Proteinuria and HematuriaDocument74 pagesEvaluating Proteinuria and HematuriaElRealManicheWemayNo ratings yet
- Case Study On Bilateral NephrolithiasisDocument84 pagesCase Study On Bilateral NephrolithiasisSteph BulanNo ratings yet
- Basic Concepts of Fluid and Electrolyte TherapyDocument136 pagesBasic Concepts of Fluid and Electrolyte Therapymuhammad ajiNo ratings yet
- Geriatric SVHADocument15 pagesGeriatric SVHACassie ValderramaNo ratings yet
- Case Study-Acute PyelonephritisDocument11 pagesCase Study-Acute PyelonephritisMary France GonzagaNo ratings yet
- Physiology Past SAQsDocument29 pagesPhysiology Past SAQsMatthew HoNo ratings yet
- Bishnu Pahari - LinkedInDocument3 pagesBishnu Pahari - LinkedInGautamNo ratings yet
- Paediatric Nursing (GNM) : Hrs. 70 Course DescriptionDocument6 pagesPaediatric Nursing (GNM) : Hrs. 70 Course DescriptionLovely SarangiNo ratings yet
- AAMA - Anatomy and Physiology QuestionsDocument11 pagesAAMA - Anatomy and Physiology QuestionsHUAWEI HUAWEINo ratings yet