You might also like
- Childhood Obesity: Causes and Consequences, Prevention and Management.From EverandChildhood Obesity: Causes and Consequences, Prevention and Management.No ratings yet
- CDC-WHO Growth Charts TrainingDocument20 pagesCDC-WHO Growth Charts TrainingKarjana183No ratings yet
- Identifying Poor Growth in Infants and ToddlersDocument15 pagesIdentifying Poor Growth in Infants and Toddlersriena456No ratings yet
- Growth MonitoringDocument44 pagesGrowth MonitoringPrakash C Raavudi100% (1)
- Guidelines For Completing Well Child Record 2016Document16 pagesGuidelines For Completing Well Child Record 2016drpklalNo ratings yet
- Nutrition Practice Care Guidelines For Preterm Infants in The CommunityDocument55 pagesNutrition Practice Care Guidelines For Preterm Infants in The CommunityReine Salamoun100% (1)
- Comparison of The WHO Child Growth Standards and The CDC 2000 Growth ChartsDocument5 pagesComparison of The WHO Child Growth Standards and The CDC 2000 Growth ChartsDickyNo ratings yet
- Childhood: EndingDocument68 pagesChildhood: EndingGiorgi KordzayaNo ratings yet
- Comparison of The WHO Child Growth Standards and The CDC 2000 Growth ChartsDocument5 pagesComparison of The WHO Child Growth Standards and The CDC 2000 Growth ChartsangelicarodriguezbNo ratings yet
- Endorsement SCNDocument1 pageEndorsement SCNLukman HusniNo ratings yet
- Growth Chart Differences WHO vs CDCDocument9 pagesGrowth Chart Differences WHO vs CDCkhoangmuaNo ratings yet
- Normal Growth Patterns in Infants and Prepubertal ChildrenDocument15 pagesNormal Growth Patterns in Infants and Prepubertal Childrenedu2029No ratings yet
- Jurnal 2 PDFDocument17 pagesJurnal 2 PDFyayu yuliantiNo ratings yet
- ToddlerDocument36 pagesToddlerCharm TanyaNo ratings yet
- Growth MonitoringDocument36 pagesGrowth MonitoringAugustus CaesarNo ratings yet
- Overview of The CDC Growth Charts: CDC: Safer - Healthier - People 1Document25 pagesOverview of The CDC Growth Charts: CDC: Safer - Healthier - People 1Batako HayashiNo ratings yet
- Growth MonitoringDocument77 pagesGrowth MonitoringPriti KhemkaNo ratings yet
- Owth FalteringDocument14 pagesOwth FalteringAdebetris AmigiaNo ratings yet
- A (Anthropometric) PRESENTATIONDocument68 pagesA (Anthropometric) PRESENTATIONNadia AbbasNo ratings yet
- Infant and Child Nutrition: Key PointsDocument4 pagesInfant and Child Nutrition: Key PointsseptiNo ratings yet
- Growth Assessment and Monitoring During Childhood: CommentaryDocument7 pagesGrowth Assessment and Monitoring During Childhood: CommentaryFajar SetiawanNo ratings yet
- ICDS Scheme ExplainedDocument59 pagesICDS Scheme ExplainedRamniwasMahoreNo ratings yet
- Differences in Growth of Canadian Children Compared To The WHO 2006 Child Growth StandardsDocument11 pagesDifferences in Growth of Canadian Children Compared To The WHO 2006 Child Growth StandardsSalsabila Munirah AmirNo ratings yet
- AnthropometryDocument63 pagesAnthropometryCamille GrefaldiaNo ratings yet
- Monitoring Public Health Nutrition Capacity DevelopmentDocument10 pagesMonitoring Public Health Nutrition Capacity DevelopmentGina RestianaNo ratings yet
- Training Module For CDC Growth Charts For Children With Special Health Care NeedsDocument28 pagesTraining Module For CDC Growth Charts For Children With Special Health Care NeedsBRIGITA CHRISTI PETRA KARINA FEBITASARI 1No ratings yet
- Nutrition Assessment and Classification: Helenita Arlene Mendones - MorosDocument26 pagesNutrition Assessment and Classification: Helenita Arlene Mendones - MorosAubrey MitraNo ratings yet
- NNS Updating 2015 Overview ReportDocument391 pagesNNS Updating 2015 Overview ReportKimberly YuNo ratings yet
- Artigo - Gestational Weight Gain ChartsDocument10 pagesArtigo - Gestational Weight Gain ChartsAlan FranciscoNo ratings yet
- Growth Monitoring 1Document56 pagesGrowth Monitoring 1hafeesadetunji01No ratings yet
- Anthropometric Measurements, Plotting and InterpretationDocument31 pagesAnthropometric Measurements, Plotting and Interpretationokwadha simionNo ratings yet
- Growth: Increase in The Physical Size of The Body As Whole or Any of Its PartsDocument4 pagesGrowth: Increase in The Physical Size of The Body As Whole or Any of Its PartsAleenaNo ratings yet
- In Brief: Normal Growth and Revised Growth ChartsDocument5 pagesIn Brief: Normal Growth and Revised Growth Chartsapi-19492580No ratings yet
- DepEd Order No. 39 SBFP GuidelinesDocument39 pagesDepEd Order No. 39 SBFP GuidelinesNiña Kristine AlinsonorinNo ratings yet
- Clinical Evaluation of The Obese Child and Adolescent (UptoDate Mai 013)Document59 pagesClinical Evaluation of The Obese Child and Adolescent (UptoDate Mai 013)jose matosNo ratings yet
- Prep 2016Document864 pagesPrep 2016pkpowerhouse100% (3)
- 121 Short Stature or at Risk of Short StatureDocument3 pages121 Short Stature or at Risk of Short Statureramadhanu100% (1)
- Dietary Guidelines For Americans 2020-2025-2Document10 pagesDietary Guidelines For Americans 2020-2025-2Guillermo ValdèsNo ratings yet
- The Child Health Programs Newborns InfantsDocument78 pagesThe Child Health Programs Newborns InfantsRae Dominick Aquino SalvaNo ratings yet
- BREASTFEEDINGDocument28 pagesBREASTFEEDINGFiona Xandra San JuanNo ratings yet
- Quasi, Rwanda, MHealth, NutritionDocument12 pagesQuasi, Rwanda, MHealth, NutritionMahadevan DNo ratings yet
- Integrated Child Development ServicesDocument18 pagesIntegrated Child Development ServicesarvindNo ratings yet
- Infant and Young Child FeedingDocument5 pagesInfant and Young Child FeedingRinjaya TeguhNo ratings yet
- NUPC 106 MODULE-V-NutritionDocument27 pagesNUPC 106 MODULE-V-NutritionCatherine Sinen ObinqueNo ratings yet
- Neonatalnutrition: Scott C. DenneDocument12 pagesNeonatalnutrition: Scott C. DenneSugiantoNo ratings yet
- Chapter1 UnlockedDocument14 pagesChapter1 UnlockedLe HuyNo ratings yet
- JPaediatrNursSci 3 3 73 761Document4 pagesJPaediatrNursSci 3 3 73 761vaideeswari kumarNo ratings yet
- Eating Well The First Year Enlivened For Web 14 DecDocument128 pagesEating Well The First Year Enlivened For Web 14 DecMargarida CarnotoNo ratings yet
- BTD 16 182 enDocument8 pagesBTD 16 182 enAudhrey BNo ratings yet
- Community Nutrition AssignmentDocument4 pagesCommunity Nutrition AssignmentDeepak DayalNo ratings yet
- Child Growth. Growth Disorders UpdateDocument57 pagesChild Growth. Growth Disorders UpdateShahpoor Ahmad ShirzadaNo ratings yet
- Nutritional StatusDocument4 pagesNutritional StatusROBLE ABDINo ratings yet
- CHN Group 4 Reporting 1Document44 pagesCHN Group 4 Reporting 1RIK HAROLD GATPANDANNo ratings yet
- Acquifer Case 2Document9 pagesAcquifer Case 2Emily SymesNo ratings yet
- Child Health Programs StrategiesDocument7 pagesChild Health Programs StrategiesFRANCES TREESA LOUISE JUMAWANNo ratings yet
- Dojebrnje PDFDocument38 pagesDojebrnje PDFСавић БојаанаNo ratings yet
- Maternal Child AdolescentDocument60 pagesMaternal Child AdolescentBilal NasirNo ratings yet
- Diversificare Copii - de La 6 LuniDocument42 pagesDiversificare Copii - de La 6 LuniDiana Oprean100% (1)
- Afoem Sample Paper Stage B Written Exam Paper 7Document43 pagesAfoem Sample Paper Stage B Written Exam Paper 7Caity YoungNo ratings yet
- Hypoxic Ischaemic Encephalopathy HIE AsphyxiaDocument6 pagesHypoxic Ischaemic Encephalopathy HIE AsphyxiaCaity YoungNo ratings yet
- Rhumatologie-Pediatrique FRDocument4 pagesRhumatologie-Pediatrique FRCaity YoungNo ratings yet
- Afoem Sample Paper Stage B Written Exam Paper 7Document46 pagesAfoem Sample Paper Stage B Written Exam Paper 7Caity YoungNo ratings yet
- Afoem Sample Paper Stage B Written Exam Paper 7Document46 pagesAfoem Sample Paper Stage B Written Exam Paper 7Caity YoungNo ratings yet
- Tic Disorder LeafletDocument2 pagesTic Disorder LeafletAndreia SilvaNo ratings yet
- A I - E M: Drenal Nsufficiency Mergency AnagementDocument12 pagesA I - E M: Drenal Nsufficiency Mergency AnagementCaity YoungNo ratings yet
- Fluid Calculator DKADocument3 pagesFluid Calculator DKACaity YoungNo ratings yet
- SSHADESS HandoutDocument1 pageSSHADESS HandoutCaity YoungNo ratings yet
- Applied Knowledge in Paediatrics - MRCPCH Mastercourse Cardiology - ClinicalKeyDocument8 pagesApplied Knowledge in Paediatrics - MRCPCH Mastercourse Cardiology - ClinicalKeyCaity YoungNo ratings yet
- 2 - McDonald - Examples - of - Unhelpful - ThoughtsDocument2 pages2 - McDonald - Examples - of - Unhelpful - ThoughtsCaity YoungNo ratings yet
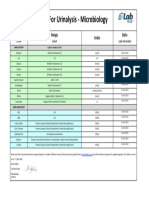
- Reference Ranges For Urinalysis - Microbiology: Test Range Units DateDocument1 pageReference Ranges For Urinalysis - Microbiology: Test Range Units DateCaity YoungNo ratings yet
- Correspondence: Classifi Cation of CFTR Mutation ClassesDocument2 pagesCorrespondence: Classifi Cation of CFTR Mutation ClassesCaity YoungNo ratings yet
- ToF ScriptDocument6 pagesToF ScriptCaity YoungNo ratings yet
- Genetic Basis For Congenital Heart Disease: Revisited: CirculationDocument59 pagesGenetic Basis For Congenital Heart Disease: Revisited: CirculationCaity YoungNo ratings yet
- Part 2: Male Reproductive System: Normal Physiology and StructureDocument30 pagesPart 2: Male Reproductive System: Normal Physiology and StructureCaity YoungNo ratings yet
- Dink in 2014Document24 pagesDink in 2014Okta Kurniawan SaputraNo ratings yet
- IsbelDocument7 pagesIsbelCaity YoungNo ratings yet
- 4-5 GlomerularDiseasesDocument21 pages4-5 GlomerularDiseasesCaity YoungNo ratings yet
- Sore Throat: Navigating The Differential DiagnosisDocument7 pagesSore Throat: Navigating The Differential DiagnosisCaity YoungNo ratings yet
- Dover Vendor Training ManualDocument40 pagesDover Vendor Training ManualAngelo ScharfNo ratings yet
- CSIRO Diet PlansDocument7 pagesCSIRO Diet PlansJulian van Raalte67% (3)
- PPCM BromocriptineDocument39 pagesPPCM BromocriptineChristian SunurNo ratings yet
- Ring Dip Progression Template For CR PDFDocument18 pagesRing Dip Progression Template For CR PDFAnaLiza PinlacNo ratings yet
- Medical Product Guide April 2019 PDFDocument36 pagesMedical Product Guide April 2019 PDFSabina IoanaNo ratings yet
- Intermittent Fasting 101 - The Ultimate Beginner's GuideDocument16 pagesIntermittent Fasting 101 - The Ultimate Beginner's Guideradhika1992No ratings yet
- Unit 06 Work Book AkDocument1 pageUnit 06 Work Book AkkillgoliatNo ratings yet
- Ch. 14 Vander's Human Physiology Book NotesDocument6 pagesCh. 14 Vander's Human Physiology Book Noteskts50% (2)
- Lsu WoDocument17 pagesLsu Wocoachmilk80% (5)
- Imdur for Angina Relief in 60 SecondsDocument23 pagesImdur for Angina Relief in 60 SecondsJoyce Anne SupnetNo ratings yet
- Global Ingredient and Out of Home Dining Trends Aug 2016Document31 pagesGlobal Ingredient and Out of Home Dining Trends Aug 2016cufi007No ratings yet
- Occlusionpaper PDFDocument10 pagesOcclusionpaper PDFNigel Allas100% (1)
- Session 1 Mbfhi A Global StrategyDocument37 pagesSession 1 Mbfhi A Global StrategyLopezDistrict FarmersHospitalNo ratings yet
- ABG Algorithm PDFDocument2 pagesABG Algorithm PDFamin2014No ratings yet
- Men's Health Bellyoff Complete W-ChaptersDocument43 pagesMen's Health Bellyoff Complete W-Chaptersbeatchica100% (12)
- Lunch Bunch - Kids Healthy Options ProgrammeDocument7 pagesLunch Bunch - Kids Healthy Options ProgrammeAlison Hourihan - Nutrition Division100% (2)
- Gluten-Free Flour in Biscuit Production Laila Ozola, Evita Straumite, Tatjana RakcejevaDocument4 pagesGluten-Free Flour in Biscuit Production Laila Ozola, Evita Straumite, Tatjana RakcejevaAle Díaz TorresNo ratings yet
- Mcardle Energy Value Food Ch4 ConnectionDocument7 pagesMcardle Energy Value Food Ch4 ConnectionsaravkiruNo ratings yet
- Journal DM Type 2Document8 pagesJournal DM Type 2LuthfiNo ratings yet
- Strength and Conditioning For Rugby League and Rugby Union Part 1Document10 pagesStrength and Conditioning For Rugby League and Rugby Union Part 1kurupirockeroNo ratings yet
- Protocol For The Conconi Test and Determination of The Heart Rate Deflection PointDocument3 pagesProtocol For The Conconi Test and Determination of The Heart Rate Deflection PointLGGNo ratings yet
- Kinetik Technologies Slim 'N' GlowDocument2 pagesKinetik Technologies Slim 'N' GlowgowestcreativeNo ratings yet
- 15 CH110 Lipids TimberlakeDocument96 pages15 CH110 Lipids TimberlakeSumit TatedNo ratings yet
- Mens FitnessDocument164 pagesMens Fitnessbushmanos100% (1)
- NHM Letter World Diabetes DayDocument9 pagesNHM Letter World Diabetes DayAnonymous RCDcVGlFpzNo ratings yet
- Kai Greene Leg Workout PDFDocument2 pagesKai Greene Leg Workout PDFHarith SimonNo ratings yet
- Trial Penang 2014 SPM Sains K1 K2 Skema (SCAN)Document18 pagesTrial Penang 2014 SPM Sains K1 K2 Skema (SCAN)Cikgu Faizal100% (3)
- CPH PPT With PicDocument31 pagesCPH PPT With PicViena Mae MaglupayNo ratings yet
- PENYALAHGUNAAN BAHAN SUKANDocument15 pagesPENYALAHGUNAAN BAHAN SUKANarehlaaNo ratings yet
- Planning and Monitoring Training Loads During The Competition Phase in Team SportsDocument7 pagesPlanning and Monitoring Training Loads During The Competition Phase in Team SportsMateus Rotermund BarattoNo ratings yet