0% found this document useful (0 votes)
1K views4 pagesCSI Nomination Form
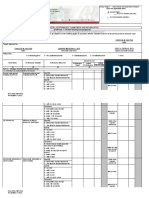
This document contains a nomination form for government officials and employees to attend training programs conducted by the Center for Strategic Initiatives (CSI). The form requests information such as the nominee's name, position, contact number, and email address. It also lists the registration terms and conditions, which state that nominees must be nominated by their agency head and will only receive a certificate of completion if they attend the entire training and comply with all requirements. The form must be signed by the authorized agency representative to agree to the terms before submitting the nominations.
Uploaded by
JAHARA PANDAPATANCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as DOCX, PDF, TXT or read online on Scribd
0% found this document useful (0 votes)
1K views4 pagesCSI Nomination Form
This document contains a nomination form for government officials and employees to attend training programs conducted by the Center for Strategic Initiatives (CSI). The form requests information such as the nominee's name, position, contact number, and email address. It also lists the registration terms and conditions, which state that nominees must be nominated by their agency head and will only receive a certificate of completion if they attend the entire training and comply with all requirements. The form must be signed by the authorized agency representative to agree to the terms before submitting the nominations.
Uploaded by
JAHARA PANDAPATANCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as DOCX, PDF, TXT or read online on Scribd