You might also like
- Public Mental Health: The Time Is Ripe For Translation of Evidence Into PracticeDocument7 pagesPublic Mental Health: The Time Is Ripe For Translation of Evidence Into PracticeLibiaNo ratings yet
- Saraceno B Freeman M Funk M. PUBLIC MENTAL HEALTHDocument20 pagesSaraceno B Freeman M Funk M. PUBLIC MENTAL HEALTHenviosmentalmedNo ratings yet
- Health Impact Pyramid Framework Research Paper On Global Health: Mental HealthDocument9 pagesHealth Impact Pyramid Framework Research Paper On Global Health: Mental Healthapi-534714258No ratings yet
- Kirkbridge Et Al - 2024 - The Social Determinants of Health and DisorderDocument33 pagesKirkbridge Et Al - 2024 - The Social Determinants of Health and DisorderVictor Hugo Loaiza SeguraNo ratings yet
- The Outbreak of Coronavirus Disease 2019: a psychological perspectiveFrom EverandThe Outbreak of Coronavirus Disease 2019: a psychological perspectiveNo ratings yet
- Global, National, and Local Approaches To Mental Health: Examples From IndiaDocument20 pagesGlobal, National, and Local Approaches To Mental Health: Examples From Indiaujangketul62No ratings yet
- Cohesive, Collaborative, Collective: Advancing Mental Health Promotion in CanadaDocument60 pagesCohesive, Collaborative, Collective: Advancing Mental Health Promotion in CanadaPeterborough Examiner100% (2)
- Mental Health, Intellectual and Developmental Disabilities and the Ageing ProcessFrom EverandMental Health, Intellectual and Developmental Disabilities and the Ageing ProcessNo ratings yet
- Mental Health Promotion: A Framework For ActionDocument6 pagesMental Health Promotion: A Framework For ActionHasrat ButtarNo ratings yet
- 10 Lund. 2018. Determinantes Sociales de La Salud Mental y ODS PDFDocument4 pages10 Lund. 2018. Determinantes Sociales de La Salud Mental y ODS PDFRobertDRockNo ratings yet
- Global mental challengesDocument1 pageGlobal mental challengesSidNo ratings yet
- Guideline MinimunDocument14 pagesGuideline MinimunsofinoyaNo ratings yet
- Mental HealthDocument4 pagesMental Healthrobin.rjmNo ratings yet
- CanteringDocument4 pagesCanteringkuspabostaNo ratings yet
- Poverty and Mental HealthDocument110 pagesPoverty and Mental HealthvikiNo ratings yet
- Mental Health and Addiction Sector ApproachDocument5 pagesMental Health and Addiction Sector ApproachNilanjana ChakrabortyNo ratings yet
- Unit 2. CPHDocument109 pagesUnit 2. CPHAesthetics MinNo ratings yet
- Community & Public Health: Course TittleDocument11 pagesCommunity & Public Health: Course TittleAesthetics MinNo ratings yet
- Healthy Public Policy AdvocacyDocument3 pagesHealthy Public Policy AdvocacyLuo MiyandaNo ratings yet
- MENTAL-HEALTHDocument2 pagesMENTAL-HEALTHzyrl1235No ratings yet
- Empowering People For Mental Health - A Literature ReviewDocument3 pagesEmpowering People For Mental Health - A Literature ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Qualities of A Healthy Community IncludeDocument3 pagesQualities of A Healthy Community Includeim_mikezNo ratings yet
- The Need for a Balanced Approach to Mental Health Promotion, Prevention and TreatmentDocument7 pagesThe Need for a Balanced Approach to Mental Health Promotion, Prevention and Treatmentshah khalidNo ratings yet
- Mental Health: Strengthening Our Response: Key FactsDocument6 pagesMental Health: Strengthening Our Response: Key FactsMarcel MaulanaNo ratings yet
- Global Mental Health Action Plan OverviewDocument22 pagesGlobal Mental Health Action Plan OverviewJenezon CardenioNo ratings yet
- Universal Health Coverage in Latin America 3: SeriesDocument9 pagesUniversal Health Coverage in Latin America 3: SeriesEgi NabilaNo ratings yet
- Mental Healthin Covid19 InfectionDocument20 pagesMental Healthin Covid19 Infectionसारथी समयNo ratings yet
- Running Head: Global Health Policy 1Document13 pagesRunning Head: Global Health Policy 1Amit KumarNo ratings yet
- Kinds of StressorDocument28 pagesKinds of StressorMay Ann VelosoNo ratings yet
- Group 10 Global HealthDocument12 pagesGroup 10 Global HealthPearl Alex CandoNo ratings yet
- Makalah EnglishDocument14 pagesMakalah EnglishMike PutriNo ratings yet
- Agenda - Addressing Mental Health - World Health Organization (WHO)Document17 pagesAgenda - Addressing Mental Health - World Health Organization (WHO)jenniferNo ratings yet
- CWTS 2 Module 2 Mental Health and Self AwarenessDocument44 pagesCWTS 2 Module 2 Mental Health and Self Awarenesstfdi support groupNo ratings yet
- Innovative Models Close Mental Health Treatment Gap with Task SharingDocument13 pagesInnovative Models Close Mental Health Treatment Gap with Task SharingCESFAM Santa AnitaNo ratings yet
- Mental HealthDocument4 pagesMental Healthvhen adrian villanuevaNo ratings yet
- Mental illness overview and plansDocument15 pagesMental illness overview and plansbeibhydNo ratings yet
- Wpa 020014Document6 pagesWpa 020014juniartiyudhaNo ratings yet
- Primary Care Mental Health in Older People: A Global PerspectiveFrom EverandPrimary Care Mental Health in Older People: A Global PerspectiveCarlos Augusto de Mendonça LimaNo ratings yet
- Jurnal Terindeks ScopusDocument8 pagesJurnal Terindeks ScopusAyu Sisca PrastiwiNo ratings yet
- Research Paper On Mental HealthDocument41 pagesResearch Paper On Mental HealthExample100% (1)
- Nimhd Strategic Plan 2021 2025Document38 pagesNimhd Strategic Plan 2021 2025jeanbourgeatNo ratings yet
- Global Burden of Mental Disorders and The Need For A Comprehensive, Coordinated Response From Health and Social Sectors at The Country LevelDocument6 pagesGlobal Burden of Mental Disorders and The Need For A Comprehensive, Coordinated Response From Health and Social Sectors at The Country Levelmohsen ghaffariNo ratings yet
- Integration of Mental Health Into Primary Health CareDocument15 pagesIntegration of Mental Health Into Primary Health CareBenson Nyirenda Jnr100% (1)
- Satcher 2000 - Executive Summary - A Report of The SG On Mental HealthDocument13 pagesSatcher 2000 - Executive Summary - A Report of The SG On Mental HealthSivaprakash BalasundaramNo ratings yet
- Un Platform FinalDocument18 pagesUn Platform FinalAginaya ReinNo ratings yet
- Week 2Document8 pagesWeek 2Cynthia ChenNo ratings yet
- Mental Health/Mental Hygiene: Awareness, Improving Population and Public HealthDocument9 pagesMental Health/Mental Hygiene: Awareness, Improving Population and Public HealthArjiel San MansuganNo ratings yet
- Promoting Mental Health: Concepts Emerging Evidence PracticeDocument70 pagesPromoting Mental Health: Concepts Emerging Evidence PracticeelvineNo ratings yet
- World Mental Health Day - 2022Document17 pagesWorld Mental Health Day - 2022TesitaNo ratings yet
- Deluao - Global Context Course ActivityDocument5 pagesDeluao - Global Context Course Activityangelica javierNo ratings yet
- Mental Health HealthDocument6 pagesMental Health Healthsarahjehad12345No ratings yet
- National Mental Health ProgrammeDocument36 pagesNational Mental Health ProgrammeSusmita Halder100% (1)
- National Mental Health Program (DOH)Document10 pagesNational Mental Health Program (DOH)Nicole Marin-ChingNo ratings yet
- 1.introduction To Public HealthDocument32 pages1.introduction To Public Healthwrite.medsyedsaadNo ratings yet
- NHPDocument13 pagesNHPCJ AngelesNo ratings yet
- The World Health Report 2005: Make Every Mother and Child Count (WHO, 2005) Recognizes The ImportanceDocument10 pagesThe World Health Report 2005: Make Every Mother and Child Count (WHO, 2005) Recognizes The ImportanceMaryni MangaNo ratings yet
- 1020 3397 2020 2610 1148 1150 EngDocument3 pages1020 3397 2020 2610 1148 1150 EngRosales RonaldNo ratings yet
- Unless Otherwise Noted, The Content of This Course Material Is Licensed Under A Creative Commons 3.0 LicenseDocument48 pagesUnless Otherwise Noted, The Content of This Course Material Is Licensed Under A Creative Commons 3.0 LicenseAmra ahmedNo ratings yet
- DesigningDocument26 pagesDesigningFIRDA NURSANTINo ratings yet
- Leading Dalam Perspektif PerencanaanDocument15 pagesLeading Dalam Perspektif PerencanaanFIRDA NURSANTINo ratings yet
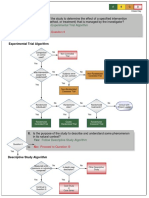
- Research Design AlgorithmDocument11 pagesResearch Design AlgorithmFIRDA NURSANTINo ratings yet
- Seaweed Biorefinery PDFDocument54 pagesSeaweed Biorefinery PDFJavier Andres Davila RinconNo ratings yet
- Reabilitare Dupa AvcDocument91 pagesReabilitare Dupa AvcDiana StancaNo ratings yet
- Method of Statement For Survey & Setting Out MakkahDocument17 pagesMethod of Statement For Survey & Setting Out MakkahToufeeq.HSE AbrarNo ratings yet
- Sensory Integration Therapy and Auditory Integration TrainingDocument10 pagesSensory Integration Therapy and Auditory Integration TrainingMuskaan KhannaNo ratings yet
- Stress Management and Well-BeingDocument4 pagesStress Management and Well-BeingAngelene FranciscoNo ratings yet
- Optometry and Vision Science Handbook - Department of Optometry (PDFDrive)Document48 pagesOptometry and Vision Science Handbook - Department of Optometry (PDFDrive)هدهد رحاب100% (1)
- F2 Chapter 4 Human HealthDocument6 pagesF2 Chapter 4 Human HealthJue Hazea GoldshopNo ratings yet
- FOMODocument13 pagesFOMONguyen Gia LinhNo ratings yet
- Dialog Patient AdmissionDocument3 pagesDialog Patient AdmissionYunita TriscaNo ratings yet
- Saudi Aramco Scaffold Safety RequirementsDocument21 pagesSaudi Aramco Scaffold Safety RequirementsKashmir Ka Bata Abdul GHAFFAR LAL DIN CHNo ratings yet
- JFamCommunityMed262113-1349692 034456Document5 pagesJFamCommunityMed262113-1349692 034456Putri Zatalini SabilaNo ratings yet
- Leadership That Get Results PPT (FINAL)Document11 pagesLeadership That Get Results PPT (FINAL)vicky gaikwadNo ratings yet
- Project BHDocument41 pagesProject BHBinsha ShyjanNo ratings yet
- Diabetics PrescriptionDocument1 pageDiabetics PrescriptionSunil HNo ratings yet
- How Do Organisms Reproduce Class 10 Notes Science Chapter 8 - Learn CBSEDocument20 pagesHow Do Organisms Reproduce Class 10 Notes Science Chapter 8 - Learn CBSEPranav MurkumbiNo ratings yet
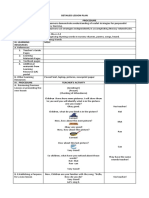
- Detailed Lesson Plan I. Objectives ProcedureDocument5 pagesDetailed Lesson Plan I. Objectives ProcedureAngelaNo ratings yet
- Tataamalan HIRARC 2020Document42 pagesTataamalan HIRARC 2020Khaty JahNo ratings yet
- Attitudes and Behaviour of School Students Towards Global Warming - A Cross Sectional Observational StudyDocument5 pagesAttitudes and Behaviour of School Students Towards Global Warming - A Cross Sectional Observational StudyIOSRjournalNo ratings yet
- Indonesian Traditional Complementary and Alternative MedicineDocument16 pagesIndonesian Traditional Complementary and Alternative MedicineIrene RaphaNo ratings yet
- Turtura ResumeDocument1 pageTurtura ResumeaturturaNo ratings yet
- Craniofacial Surgery Brochure - PRINTDocument2 pagesCraniofacial Surgery Brochure - PRINTLaily AkbarNo ratings yet
- Neurologia Croatica CROCAD 2020Document96 pagesNeurologia Croatica CROCAD 2020Goran SimicNo ratings yet
- Walmart Drug ListDocument6 pagesWalmart Drug ListShirley Pigott MDNo ratings yet
- Strategies For Ethical Decision Making: Nine Step Model: Gerald P. Koocher & Patricia Keith-SpiegelDocument9 pagesStrategies For Ethical Decision Making: Nine Step Model: Gerald P. Koocher & Patricia Keith-Spiegelpai_jyotiNo ratings yet
- Hazards and Risks of Catalyst Replacement at Butane TreaterDocument32 pagesHazards and Risks of Catalyst Replacement at Butane TreaterIhdaNo ratings yet
- 1 - The Leader's Light or ShadowDocument29 pages1 - The Leader's Light or ShadowLeslie Ann Elazegui UntalanNo ratings yet
- Heart Disease Prediction Model: DissertationDocument4 pagesHeart Disease Prediction Model: DissertationGaurav MehraNo ratings yet
- HSE L151 - 2014 - Explosives Regulations 2014 Guidance On Regulations - Security ProvisionsDocument68 pagesHSE L151 - 2014 - Explosives Regulations 2014 Guidance On Regulations - Security ProvisionsKris WilochNo ratings yet
- Safety Data Sheet (SDS) Anysol-D100Document11 pagesSafety Data Sheet (SDS) Anysol-D100U.s. Ezhil ArivudainambiNo ratings yet
- Nitthiyan AnneeeDocument27 pagesNitthiyan AnneeeVisali0311No ratings yet