You might also like
- AKI Vs CKD Lecture Latest 3rd Dec 2018Document51 pagesAKI Vs CKD Lecture Latest 3rd Dec 2018mugilessNo ratings yet
- Gyne - Benign LesionsDocument4 pagesGyne - Benign LesionsIsabel CastilloNo ratings yet
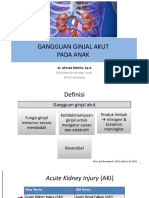
- 2.2gangguan Ginjal Akut Pada AnakDocument34 pages2.2gangguan Ginjal Akut Pada AnakMUNIFRIZALNo ratings yet
- Acute Kidney Injury in HospitaDocument7 pagesAcute Kidney Injury in HospitaRobertNo ratings yet
- AKI Diagnosis and ClassificationDocument12 pagesAKI Diagnosis and ClassificationIndah Nur LathifahNo ratings yet
- Leziunea Acuta de Rinichi (LAR) : Acute Kidney Injury (AKI) Insuficienta Renala Acuta (IRA)Document49 pagesLeziunea Acuta de Rinichi (LAR) : Acute Kidney Injury (AKI) Insuficienta Renala Acuta (IRA)mihai mayorNo ratings yet
- Chapter 28-1 - Approach To The Patient With Acute Kidney Injury - Case 1Document9 pagesChapter 28-1 - Approach To The Patient With Acute Kidney Injury - Case 1fabyuiNo ratings yet
- Acute Kidney Injury: Acute Kidney Injury (AKI) Is A Clinical Syndrome Generally Defined by AnDocument13 pagesAcute Kidney Injury: Acute Kidney Injury (AKI) Is A Clinical Syndrome Generally Defined by AnARMANo ratings yet
- AKI LectureDocument95 pagesAKI LectureDaryl Gay NanoNo ratings yet
- Variation in 1 3S and 2 2S RejectionsDocument6 pagesVariation in 1 3S and 2 2S Rejectionsisaungureanu88.iuNo ratings yet
- 3rd Session - Management of Hyperglycemic Crisis - DR Lukman Hatta SPPDDocument24 pages3rd Session - Management of Hyperglycemic Crisis - DR Lukman Hatta SPPDAndhika WicaksanaNo ratings yet
- CKD Research Menuscript Final AmiyanshuDocument11 pagesCKD Research Menuscript Final AmiyanshuAmiyanshu BeheraNo ratings yet
- 2 - Diagnostic AKI in ICU From KDIGO To BlomakerDocument80 pages2 - Diagnostic AKI in ICU From KDIGO To Blomakerhartanto_budi6222No ratings yet
- 15-Acute Kidney InjuryDocument18 pages15-Acute Kidney Injuryمصطفى محمد جواد كاظمNo ratings yet
- Perioperativeacute Kidneyinjury: Risk Factors and Predictive StrategiesDocument18 pagesPerioperativeacute Kidneyinjury: Risk Factors and Predictive StrategiesBillyNicolasNo ratings yet
- N Engl J Med 2022 386 964 - AppendixDocument5 pagesN Engl J Med 2022 386 964 - AppendixEvelynNo ratings yet
- HA 1 SolvedDocument8 pagesHA 1 Solvednoorkomal47No ratings yet
- Pediatric Oncology Calculations & Monitoring Clinical PearlsDocument11 pagesPediatric Oncology Calculations & Monitoring Clinical PearlsTaufik HidayahNo ratings yet
- National Competition Case: ASHP Clinical Skills CompetitionDocument16 pagesNational Competition Case: ASHP Clinical Skills CompetitionHelmiNo ratings yet
- Sulphur ChemicalDocument5 pagesSulphur ChemicalRASHMIN GADHIYANo ratings yet
- Pitfalls in Dengue and Management: Prof MD Robed Amin Prof of Medicine Line Director NCDC DghsDocument17 pagesPitfalls in Dengue and Management: Prof MD Robed Amin Prof of Medicine Line Director NCDC DghsMr xNo ratings yet
- CPrecision July 23 PDFDocument6 pagesCPrecision July 23 PDFGeorjalyn Joy Quiachon (Jaja)No ratings yet
- Handbook - Diagnosis and Staging of AKI Based On KDIGODocument33 pagesHandbook - Diagnosis and Staging of AKI Based On KDIGOMadyline KatipanaNo ratings yet
- Adobe Scan Nov 08, 2022Document11 pagesAdobe Scan Nov 08, 2022artemis 0516No ratings yet
- Table 30-1Document1 pageTable 30-1Dragutin PetrićNo ratings yet
- Formulation and Evaluation of Mucoadhesive Glipizide MicrospheresDocument18 pagesFormulation and Evaluation of Mucoadhesive Glipizide MicrospheresVinay SainiNo ratings yet
- AKI MBCHB VDocument64 pagesAKI MBCHB VSsenyonga DominicNo ratings yet
- Department of Clinical Biochemistry: Lipid ProfileDocument3 pagesDepartment of Clinical Biochemistry: Lipid ProfilegeorgeNo ratings yet
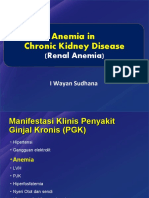
- Anemia in Chronic Kidney DiseaseDocument38 pagesAnemia in Chronic Kidney DiseaseHemodialisa LindimaraNo ratings yet
- Critical ResultDocument2 pagesCritical ResultSUSANTONo ratings yet
- Background: CKD of Uncertain Etiology Sri Lanka A Population Study at Girandurukotte, Uva Province, Preliminary ReportDocument6 pagesBackground: CKD of Uncertain Etiology Sri Lanka A Population Study at Girandurukotte, Uva Province, Preliminary Reportsumanenthiran123No ratings yet
- Seminar HD-RSUD Sleman 2019Document36 pagesSeminar HD-RSUD Sleman 2019herkamaya100% (1)
- Nutrients: Nutritional Status of Bariatric Surgery CandidatesDocument11 pagesNutrients: Nutritional Status of Bariatric Surgery CandidatesDana MuresanNo ratings yet
- Pemeriksaan KlinisDocument1 pagePemeriksaan Klinis30. Nur Alia BalqisNo ratings yet
- R E W IN D: Esearching CV Vents With A Eekly Cretin in IabetesDocument69 pagesR E W IN D: Esearching CV Vents With A Eekly Cretin in IabetesChristian Acosta VillegasNo ratings yet
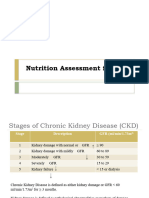
- CKD Final 2Document4 pagesCKD Final 2Amiyanshu BeheraNo ratings yet
- Adekuasi HD (Pelatihan HD, 10 Maret 2016)Document42 pagesAdekuasi HD (Pelatihan HD, 10 Maret 2016)MeryNo ratings yet
- Wednesday SomersDocument57 pagesWednesday SomersNational Press FoundationNo ratings yet
- AkiDocument20 pagesAkiEnvhy AmaliaNo ratings yet
- Git Case 3 Kunwor, BishalDocument15 pagesGit Case 3 Kunwor, BishalBishal JB KunworNo ratings yet
- Disease: Colchicine in Patients With Chronic CoronaryDocument8 pagesDisease: Colchicine in Patients With Chronic CoronaryNiki MawraNo ratings yet
- Name Lab No. A/c Status Sahil MKPDP1035 P Age: 23 Years Gender: Ref By: DR - Veena Bora Collected Received Reported Report StatusDocument2 pagesName Lab No. A/c Status Sahil MKPDP1035 P Age: 23 Years Gender: Ref By: DR - Veena Bora Collected Received Reported Report StatusBathroom SingersNo ratings yet
- Pathogenesis and Management Sepsis - Aki: Fajar Yuwanto Rsud Abdul Moeloek Bandar LampungDocument21 pagesPathogenesis and Management Sepsis - Aki: Fajar Yuwanto Rsud Abdul Moeloek Bandar LampungNodi Rahma DiniNo ratings yet
- Kidney Transplantation Without Prior Dialysis in Children: The Eurotransplant ExperienceDocument16 pagesKidney Transplantation Without Prior Dialysis in Children: The Eurotransplant ExperienceElisabethJaniceRusliNo ratings yet
- 2017-Issues of Acute Kidney Injury Staging and Management in Sepsis and Critical Illness A Narrative Review PDFDocument25 pages2017-Issues of Acute Kidney Injury Staging and Management in Sepsis and Critical Illness A Narrative Review PDFClaudioLagosNo ratings yet
- The Miracle of Vegan (Dr. Susianto Tseng) - Susianto TsengDocument43 pagesThe Miracle of Vegan (Dr. Susianto Tseng) - Susianto Tsengharrykusuma199No ratings yet
- Anemia in Chronic Kidney DiseaseDocument37 pagesAnemia in Chronic Kidney DiseaseRendyNo ratings yet
- Uk007 2223 006609Document3 pagesUk007 2223 006609Arpit KumarNo ratings yet
- Jurnal Daun Kersen Untuk DiabetesDocument11 pagesJurnal Daun Kersen Untuk DiabetesMuhammad FahrisNo ratings yet
- Sush PMBDocument38 pagesSush PMBAnindaNo ratings yet
- Analisis 2Document6 pagesAnalisis 2josé armando ramirezNo ratings yet
- CASE STUDY FORMAT (Kidney Transplantation)Document12 pagesCASE STUDY FORMAT (Kidney Transplantation)ashnaNo ratings yet
- Anemia Renal - BDF 2018-2Document38 pagesAnemia Renal - BDF 2018-2Buku Tama WaingapuNo ratings yet
- 4 Assesmment + Case - FinalDocument20 pages4 Assesmment + Case - FinalSophie RoseNo ratings yet
- Result and ConclusionDocument30 pagesResult and ConclusionjirapichaNo ratings yet
- Chemistry Unit: 6.3 Glycated Haemoglobin (Hba1C)Document2 pagesChemistry Unit: 6.3 Glycated Haemoglobin (Hba1C)SwissFm Cleaning CaptainsNo ratings yet
- 1030-1200 G JonesDocument50 pages1030-1200 G Jonesrezki_WSNo ratings yet
- N NJ Grand RoundDocument39 pagesN NJ Grand RoundIshfaq AhmadNo ratings yet
- Nutritional Genomics: Discovering the Path to Personalized NutritionFrom EverandNutritional Genomics: Discovering the Path to Personalized NutritionJim KaputNo ratings yet
- Worksheet I For Land Administration and Surveying ProgramDocument3 pagesWorksheet I For Land Administration and Surveying ProgramZewudu MossieNo ratings yet
- Ian Watson Homeopathic Remedies For Current Outbreak - March 2020 Version 1Document1 pageIan Watson Homeopathic Remedies For Current Outbreak - March 2020 Version 1sneemNo ratings yet
- MPT Question BankDocument26 pagesMPT Question BankAbilash Prabhuraj M KNo ratings yet
- NAGPUR QUARANTINE LIST Police STN WiseDocument37 pagesNAGPUR QUARANTINE LIST Police STN Wiseabhijeet singh amarnathNo ratings yet
- Treatment Priciples in The Management of Open FractureDocument23 pagesTreatment Priciples in The Management of Open FractureNunks FiryaniNo ratings yet
- Autoimun Cook2023Document36 pagesAutoimun Cook2023Salsabila RatuNo ratings yet
- Charleston County Clinical Operating Guidelines: Adult & PediatricDocument207 pagesCharleston County Clinical Operating Guidelines: Adult & PediatricJohn DodsonNo ratings yet
- Environmental TheoryDocument3 pagesEnvironmental Theorydp dlsntsNo ratings yet
- Managing Side Effects of COVID VaccineDocument2 pagesManaging Side Effects of COVID VaccineMugluuNo ratings yet
- The Social Impact of Covid-19Document1 pageThe Social Impact of Covid-19Trisha MaguikayNo ratings yet
- Guide To CPET Versie FinaalDocument21 pagesGuide To CPET Versie Finaaljimurga100% (1)
- Relation of Alcohol Consumption and Benign Breast DiseasesDocument8 pagesRelation of Alcohol Consumption and Benign Breast DiseasesmohamedhazemelfollNo ratings yet
- DHMS Chronic - Illness - Benefit PDFDocument9 pagesDHMS Chronic - Illness - Benefit PDFNontobeko MkhizeNo ratings yet
- Information 13 00330 v2 PDFDocument28 pagesInformation 13 00330 v2 PDFYasmine A. SabryNo ratings yet
- Rehab (Soap)Document14 pagesRehab (Soap)Norhuzmaira Mohd RofaeiNo ratings yet
- RMTH Chapter OneDocument42 pagesRMTH Chapter Onesosina eseyewNo ratings yet
- Pre Diabetes Risk Factor Management Nov16Document7 pagesPre Diabetes Risk Factor Management Nov16CharlieNo ratings yet
- Capacity of Hospita101 2Document45 pagesCapacity of Hospita101 2kneou dojolesNo ratings yet
- Synovial ChondromatosisDocument4 pagesSynovial ChondromatosisNadia Bordaş100% (1)
- Childrens Uniform Mental Health Assessment CUMHA 1Document14 pagesChildrens Uniform Mental Health Assessment CUMHA 1Hira WarsiNo ratings yet
- The Real Risks of MarijuanaDocument5 pagesThe Real Risks of MarijuanaIvy Maril De GuzmanNo ratings yet
- SYPHILIS (103 To 108) PPT - PPTX - 20230906 - 161225 - 0000Document15 pagesSYPHILIS (103 To 108) PPT - PPTX - 20230906 - 161225 - 0000Aaditya GadhviNo ratings yet
- HP4. Endocrine System - 100 - Ethan HelmDocument17 pagesHP4. Endocrine System - 100 - Ethan HelmNorPhea - នភាNo ratings yet
- Injury Report Form: Circle and NameDocument1 pageInjury Report Form: Circle and NameNinNo ratings yet
- Heart Disease Prediction Using Machine Learning Techniques: Devansh Shah Samir Patel Santosh Kumar BhartiDocument6 pagesHeart Disease Prediction Using Machine Learning Techniques: Devansh Shah Samir Patel Santosh Kumar Bhartifuck MeNo ratings yet
- 3rd Quarter Test Item Bank School Year 2019-2020 Subject: MAPEH 10 Code Learning CompetenciesDocument4 pages3rd Quarter Test Item Bank School Year 2019-2020 Subject: MAPEH 10 Code Learning Competenciesmilafer dabanNo ratings yet
- Saponins and Their Potential Role in Diabetes MellitusDocument12 pagesSaponins and Their Potential Role in Diabetes MellitusArmenia Eka PutrianaNo ratings yet
- FDA NiacinDocument22 pagesFDA NiacinSALSABILA KURNIASIHNo ratings yet
- Warsaw Ghetto Thesis StatementDocument6 pagesWarsaw Ghetto Thesis Statementfd0kyjpa100% (2)