You might also like
- Medical Terminology - Prefixes, Suffixes, Root WordsDocument9 pagesMedical Terminology - Prefixes, Suffixes, Root Wordssooperstarx2171% (7)
- Lab - 18 (Gizmo) Senses SEDocument8 pagesLab - 18 (Gizmo) Senses SEJack50% (4)
- Gastrointestinal Physiology, JohnsonDocument310 pagesGastrointestinal Physiology, JohnsonSubhajit Chakraborty80% (5)
- MBBS renal physiology lecture notesDocument129 pagesMBBS renal physiology lecture notesNayyer Khan83% (6)
- Functions of KidneyDocument24 pagesFunctions of KidneyJohnson100% (1)
- Anatomy, Lecture 12, Blood Supply of The Gastrointestinal Tract (Slides)Document27 pagesAnatomy, Lecture 12, Blood Supply of The Gastrointestinal Tract (Slides)Ali Al-QudsiNo ratings yet
- HAPP Supplementary Notes - Urinary SystemDocument15 pagesHAPP Supplementary Notes - Urinary SystemZuhri PorzaNo ratings yet
- Final UrinarysystemDocument15 pagesFinal UrinarysystemPrabhjot KaurNo ratings yet
- Physiology Handouts (Topics 89-103)Document19 pagesPhysiology Handouts (Topics 89-103)bc200411046No ratings yet
- Renal Anatomy and PhysiologyDocument15 pagesRenal Anatomy and PhysiologySapna JainNo ratings yet
- Introduction to the Renal System and Kidney Anatomy (39Document10 pagesIntroduction to the Renal System and Kidney Anatomy (39Jeeson MichaelNo ratings yet
- Radi 583 Paper Final Draft - HicksDocument26 pagesRadi 583 Paper Final Draft - Hicksapi-356393960No ratings yet
- Anatomy and Physiology of KidneyDocument5 pagesAnatomy and Physiology of KidneyMaLik ZaKwan IwAnNo ratings yet
- Urinary System - Students ReadingDocument16 pagesUrinary System - Students ReadingQashqar & GB FolksNo ratings yet
- Location and External Anatomy of The KidneysDocument15 pagesLocation and External Anatomy of The KidneysKyla Malapit GarvidaNo ratings yet
- The Kidneys Are A Pair of Purplish-Brown Organs Is Located Below The Ribs Toward The Middle ofDocument6 pagesThe Kidneys Are A Pair of Purplish-Brown Organs Is Located Below The Ribs Toward The Middle ofJoana Bless PereyNo ratings yet
- UrinaryDocument15 pagesUrinaryJovelou MihangosNo ratings yet
- HISTOLOGY OF THE KIDNEYDocument4 pagesHISTOLOGY OF THE KIDNEYIzzi FekratNo ratings yet
- Urinary SystemDocument28 pagesUrinary Systemgabanule brandonNo ratings yet
- Urinary System AssessmentDocument43 pagesUrinary System AssessmentGiri Siva100% (2)
- The Structure of A Kidney NephronDocument4 pagesThe Structure of A Kidney NephronMarie St. Louis100% (1)
- Anatomy and Physiology-KIDNEYSDocument5 pagesAnatomy and Physiology-KIDNEYSnessie dianne c. cuevasNo ratings yet
- Urinary SystemDocument64 pagesUrinary SystemAlishba AslamNo ratings yet
- Review of AnaphysioDocument8 pagesReview of AnaphysioDizerine Mirafuentes RolidaNo ratings yet
- The Urinary System: Structure and Functions in 40 CharactersDocument30 pagesThe Urinary System: Structure and Functions in 40 CharactersRadia RaicyNo ratings yet
- The Human Renal SystemDocument6 pagesThe Human Renal Systemhoneydine_03No ratings yet
- The Human Renal SystemDocument15 pagesThe Human Renal SystemChuche SustentoNo ratings yet
- RenalphysiologyDocument178 pagesRenalphysiologyanisreeNo ratings yet
- Study Guide 24 - Urinary SystemDocument19 pagesStudy Guide 24 - Urinary SystemcharlesNo ratings yet
- Anatomy and PhysiologyDocument17 pagesAnatomy and PhysiologychardiginNo ratings yet
- Human Anatomy Handout 2Document23 pagesHuman Anatomy Handout 2Daniel LemmaNo ratings yet
- Hafeezullah: Subject:Anatomy Topic: Anatomy of Excretory System Roll No: 15 Semester: 1 RepeaterDocument10 pagesHafeezullah: Subject:Anatomy Topic: Anatomy of Excretory System Roll No: 15 Semester: 1 RepeaterMuhammad ShahzaibNo ratings yet
- UNIT 10 (Urinary System)Document6 pagesUNIT 10 (Urinary System)Workinesh Kaynabo KambaloNo ratings yet
- Urinary System FunctionsDocument9 pagesUrinary System FunctionsPande YogamNo ratings yet
- Kidney Anatomy and PhysiologyDocument5 pagesKidney Anatomy and PhysiologyDianne MacaraigNo ratings yet
- Urinary System Part 1Document8 pagesUrinary System Part 1عبدالرحمن عدي عبدالفتاح100% (1)
- Anatomy Ginjal 2Document16 pagesAnatomy Ginjal 2agung neutronNo ratings yet
- Diffusion and Osmosis in The Human BodyDocument13 pagesDiffusion and Osmosis in The Human BodyCody EllisNo ratings yet
- SJFJFDocument9 pagesSJFJFcharizze alpechiNo ratings yet
- Understanding the Urinary SystemDocument7 pagesUnderstanding the Urinary SystemGanah PeterNo ratings yet
- The Human Renal SystemDocument8 pagesThe Human Renal SystemRobert CaseyNo ratings yet
- Anatomy of the Urinary System: Kidneys and NephronsDocument6 pagesAnatomy of the Urinary System: Kidneys and NephronsHunter Japon TorquiNo ratings yet
- The Kidneys The Functions of The KidneyDocument5 pagesThe Kidneys The Functions of The KidneylaraNo ratings yet
- Prepared by ShakirullahDocument99 pagesPrepared by ShakirullahKhan AbubakarNo ratings yet
- MIRADOR, Kiana AnaphyAct16Document4 pagesMIRADOR, Kiana AnaphyAct16Kiana MiradorNo ratings yet
- Anatomy and physiology of the cardiovascular systemDocument11 pagesAnatomy and physiology of the cardiovascular systemKier_John_Kora_9076No ratings yet
- Anatomy 2nd-U-5 Urinary SystemDocument115 pagesAnatomy 2nd-U-5 Urinary Systemsinte beyuNo ratings yet
- Kidneys filter blood and produce urine through nephronsDocument4 pagesKidneys filter blood and produce urine through nephronsArif NabeelNo ratings yet
- Chapter-19 Excretory Products and Their Elimnation: Forms of Nitrogen ExcretionsDocument8 pagesChapter-19 Excretory Products and Their Elimnation: Forms of Nitrogen Excretionsmaryak3050No ratings yet
- Urinary SystemDocument24 pagesUrinary SystemTalal TariqNo ratings yet
- The Excretory System: Vital for Waste RemovalDocument13 pagesThe Excretory System: Vital for Waste RemovalbnksukantaNo ratings yet
- Histology of The The Urinary SystemDocument63 pagesHistology of The The Urinary SystemKankomba MuleyaNo ratings yet
- Anatomic and Physiologic OverviewDocument5 pagesAnatomic and Physiologic OverviewShannen Alija M. LaoNo ratings yet
- Xcretory System: BY: Pramod KumarDocument50 pagesXcretory System: BY: Pramod KumarCay C. CordovaNo ratings yet
- Urinary System 1. List The Functions of The KidneysDocument6 pagesUrinary System 1. List The Functions of The KidneysheerNo ratings yet
- The Urinary System: Kidneys, Nephrons and Urine FormationDocument45 pagesThe Urinary System: Kidneys, Nephrons and Urine FormationRyann SmithNo ratings yet
- Urinary SystemDocument14 pagesUrinary SystemSaadNo ratings yet
- Urinary SystemDocument2 pagesUrinary SystemCharlayne AnneNo ratings yet
- HomeostasisDocument10 pagesHomeostasisSiddhesh YadavNo ratings yet
- Anatomy and Physiology of Urinary SystemDocument5 pagesAnatomy and Physiology of Urinary SystemIan CruzNo ratings yet
- Nteractive 3d-Model Scheme of The Circulation:: Pomacea Canaliculata SnailDocument3 pagesNteractive 3d-Model Scheme of The Circulation:: Pomacea Canaliculata SnailAnonymous odVgws2No ratings yet
- External AnatomyDocument6 pagesExternal AnatomyRosevick BadocoNo ratings yet
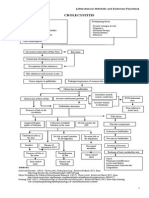
- Cholecystitis: (Alterations in Metabolic and Endocrine Functions)Document4 pagesCholecystitis: (Alterations in Metabolic and Endocrine Functions)Jorie RocoNo ratings yet
- How Animals SurviveDocument69 pagesHow Animals SurviveMichael Daryl GalsimNo ratings yet
- Pavlov by KonorskiDocument4 pagesPavlov by KonorskiG1993NCKNo ratings yet
- Treatment of Nipple Hypertrophy by A Simplified Reduction TechniqueDocument7 pagesTreatment of Nipple Hypertrophy by A Simplified Reduction TechniqueАндрей ПетровNo ratings yet
- Cranial Nerves SummaryDocument3 pagesCranial Nerves SummaryJoash F. Pacquing75% (4)
- Animaltissues 180604115637Document40 pagesAnimaltissues 180604115637proud.student2023No ratings yet
- Liver Cirrhosis PowerPointDocument12 pagesLiver Cirrhosis PowerPointFrancis Adrian100% (2)
- First Quarterly Test: General Biology 2Document10 pagesFirst Quarterly Test: General Biology 2glaiza abucayNo ratings yet
- Renal ScintigraphyDocument20 pagesRenal ScintigraphyHengNo ratings yet
- Liver HistologyDocument7 pagesLiver HistologyAhmad Khan GhoriNo ratings yet
- Pacemaker Learning Package: Paula Nekic CNE Liverpool Hospital ICU January 2016Document46 pagesPacemaker Learning Package: Paula Nekic CNE Liverpool Hospital ICU January 2016Zahangir Kabir AshikNo ratings yet
- Diabetes Related CKD 2Document1 pageDiabetes Related CKD 2Jia-PeiWuNo ratings yet
- ANPH 4114 PHAP 4114: Graduate School of MedicineDocument8 pagesANPH 4114 PHAP 4114: Graduate School of MedicinelovelysyafiqahNo ratings yet
- Acute CholangitisDocument12 pagesAcute CholangitisWira LinNo ratings yet
- Module 9 Lesson 4Document11 pagesModule 9 Lesson 4Faatoots FatsNo ratings yet
- Addison DiseaseDocument23 pagesAddison DiseaseKompari EvansNo ratings yet
- CMDA STUDENTS EXAMDocument9 pagesCMDA STUDENTS EXAMEwaoluwa AribaNo ratings yet
- KIDNEYDocument3 pagesKIDNEYBaJo GarnaceNo ratings yet
- Food Classes: FAT Water Vitamins, Minerals, & Roughage ProteinDocument25 pagesFood Classes: FAT Water Vitamins, Minerals, & Roughage Proteinuminoriah80% (5)
- Dialog Konseling-1Document8 pagesDialog Konseling-1ni kadek purwatiNo ratings yet
- TCD Thyroid-6-1Document72 pagesTCD Thyroid-6-1amrsameerNo ratings yet
- Anatomy and Physiology - Kidney - ForDocument3 pagesAnatomy and Physiology - Kidney - ForKristelle ModalesNo ratings yet
- Animal Nervous System (Earthworm & Fish)Document18 pagesAnimal Nervous System (Earthworm & Fish)Keth LaurelNo ratings yet
- Anatomy and Physiology GMCDocument15 pagesAnatomy and Physiology GMCsamantha tanoNo ratings yet
- 3.2 The Kidneys and HomeostasisDocument2 pages3.2 The Kidneys and HomeostasisNirmala Josephine0% (3)
- Congenital HypothyroidismDocument50 pagesCongenital HypothyroidismG VenkateshNo ratings yet