You might also like
- CementationDocument40 pagesCementationKumarNo ratings yet
- CementsDocument113 pagesCementsMahBebeNo ratings yet
- Luting Cements and CementationDocument59 pagesLuting Cements and CementationDRPRIYA007No ratings yet
- Material Merged MergedDocument204 pagesMaterial Merged MergedBasma BasemNo ratings yet
- Dental Cements SectionDocument56 pagesDental Cements Sectionnehalabosamra91No ratings yet
- Cement Bases LinersDocument50 pagesCement Bases LinersNoura RihanNo ratings yet
- Luting Agents and Cementation Techniques: April 2021Document11 pagesLuting Agents and Cementation Techniques: April 2021Anh Tuan DangNo ratings yet
- Dental Cements SectionDocument56 pagesDental Cements Sectionnehalabosamra91No ratings yet
- Glass ionomer cement properties and usesDocument67 pagesGlass ionomer cement properties and usesANUBHA75% (4)
- Zinc Oxide Eugenol CementDocument32 pagesZinc Oxide Eugenol CementSahil SethiNo ratings yet
- Provisional Restoration in FPDDocument45 pagesProvisional Restoration in FPDrejipg100% (1)
- 04 - 003 Dental Luting CementsDocument2 pages04 - 003 Dental Luting CementsZazilatul KhikmiahNo ratings yet
- Dental Cements Guide: Classification, Properties & UsesDocument11 pagesDental Cements Guide: Classification, Properties & Usessakib samiNo ratings yet
- Dental Luting Cement Types & Selection CriteriaDocument23 pagesDental Luting Cement Types & Selection CriteriaNabil Al KingNo ratings yet
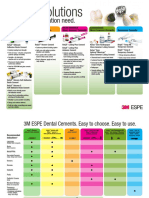
- Technical Product Profile: RelyxDocument28 pagesTechnical Product Profile: RelyxTriawan NuswantoroNo ratings yet
- Dental Cements: Dr. Hamida KhatunDocument39 pagesDental Cements: Dr. Hamida Khatunsakib samiNo ratings yet
- Dental CementDocument8 pagesDental CementDuha SalwanNo ratings yet
- Tooth Colored RestorationDocument98 pagesTooth Colored Restorationjamaica faith ramonNo ratings yet
- 04 - 003 Dental Luting CementsDocument2 pages04 - 003 Dental Luting CementskaniaNo ratings yet
- 7 - DrAbeer's Lecture (Dental Cements & Cementation Procedures) PDFDocument51 pages7 - DrAbeer's Lecture (Dental Cements & Cementation Procedures) PDFTasneem ShamaliNo ratings yet
- Dental CementsDocument47 pagesDental CementsDrShweta SainiNo ratings yet
- Pulp Protection Methods and MaterialsDocument13 pagesPulp Protection Methods and MaterialsmirfanulhaqNo ratings yet
- Pulp Protection Methods and MaterialsDocument13 pagesPulp Protection Methods and MaterialsmirfanulhaqNo ratings yet
- Glass Ionomer Cement: Made By: Dr. Shweta Rahi Roll No.-185 2K15 BatchDocument26 pagesGlass Ionomer Cement: Made By: Dr. Shweta Rahi Roll No.-185 2K15 BatchlucasNo ratings yet
- Lecture 9 & 10 - Cements (Slides)Document52 pagesLecture 9 & 10 - Cements (Slides)JustDen09No ratings yet
- All DMS Essay Questions 06-14Document17 pagesAll DMS Essay Questions 06-14mepegajNo ratings yet
- DR Sonu (Cements)Document123 pagesDR Sonu (Cements)SonuNo ratings yet
- Dental Cement 1Document5 pagesDental Cement 1eslamezzat21061990No ratings yet
- Non-adhesive cement cannot bond to tooth structure or restoration. Resin cement bonds micromechanically to etched surfacesDocument89 pagesNon-adhesive cement cannot bond to tooth structure or restoration. Resin cement bonds micromechanically to etched surfacesNikita Aggarwal71% (7)
- Dental Cements: BY Pranalika Kanojiya Mds 1 YearDocument128 pagesDental Cements: BY Pranalika Kanojiya Mds 1 Yearpranalika .................No ratings yet
- Introduction To Composites: Dr. MehreenDocument24 pagesIntroduction To Composites: Dr. MehreenAnfal TariqNo ratings yet
- Dental Materials: Types of The CementsDocument40 pagesDental Materials: Types of The CementsFoysal SirazeeNo ratings yet
- Dental Cements Used in Fixed Dental ProsthrsisDocument83 pagesDental Cements Used in Fixed Dental ProsthrsissonalitalkeNo ratings yet
- Dental CementDocument74 pagesDental CementAisha samreenNo ratings yet
- Relyx Product ChartDocument2 pagesRelyx Product ChartRicardo Cenicante0% (1)
- Anyagtan Dental Cemetns AngolDocument36 pagesAnyagtan Dental Cemetns Angolia_moheetNo ratings yet
- Operative Dentistry 2004Document269 pagesOperative Dentistry 2004dishakamath100% (5)
- Ceramic Inlays and Onlays: Presented By, Dr. G. V. Krishna Mohan, Reader in Department of Prosthodontics, SscdsDocument35 pagesCeramic Inlays and Onlays: Presented By, Dr. G. V. Krishna Mohan, Reader in Department of Prosthodontics, SscdsAya Ibrahim YassinNo ratings yet
- Resin Composite Fall 12Document25 pagesResin Composite Fall 12Naji Z. ArandiNo ratings yet
- Glass Ionomer in Contemp Orary Restorative Dentistr Y: by Rooj Rojasawasthien. DDS, Msc. 16 August 2010Document42 pagesGlass Ionomer in Contemp Orary Restorative Dentistr Y: by Rooj Rojasawasthien. DDS, Msc. 16 August 2010Dent YomarajNo ratings yet
- Luting CementsDocument22 pagesLuting CementsAfaf MagedNo ratings yet
- Recent Advances in Luting CementsDocument82 pagesRecent Advances in Luting CementsChaitrali Desai83% (6)
- Varnishes Liners BasesDocument35 pagesVarnishes Liners BasesAbdul ShameemNo ratings yet
- Provisional Restorations: Wael Al-Omari. BDS, Mdentsci, PHDDocument27 pagesProvisional Restorations: Wael Al-Omari. BDS, Mdentsci, PHDSuvasish SuvasishNo ratings yet
- Luting Cement Types and PropertiesDocument70 pagesLuting Cement Types and PropertiesGoutham SunilNo ratings yet
- Cement Ebook Layout 3.8.19 PDFDocument27 pagesCement Ebook Layout 3.8.19 PDFIndira Mota100% (1)
- Screenshot 2022-09-30 at 12.40.41 AMDocument59 pagesScreenshot 2022-09-30 at 12.40.41 AMgulrukh.bNo ratings yet
- Dental CementsDocument159 pagesDental Cementsdrbaraa93100% (6)
- Classification of Glass Ionomer CementsDocument6 pagesClassification of Glass Ionomer Cementssuchi7sahaNo ratings yet
- Dental Materials IVDocument11 pagesDental Materials IVkevin1678100% (1)
- Dental Cements Chapter 13Document60 pagesDental Cements Chapter 13Maria Mercedes LeivaNo ratings yet
- Dental Luting Cements Objectives:: Course Date: 10/10 Expiration Date: 10/13Document14 pagesDental Luting Cements Objectives:: Course Date: 10/10 Expiration Date: 10/13Dampee ReturnNo ratings yet
- Biomaterials Lecture 2Document3 pagesBiomaterials Lecture 2alinehh5No ratings yet
- Denture Base Resins 03Document49 pagesDenture Base Resins 03AyaNo ratings yet
- Concrete in Highway Engineering: International Series of Monographs in Civil EngineeringFrom EverandConcrete in Highway Engineering: International Series of Monographs in Civil EngineeringRating: 4 out of 5 stars4/5 (5)
- Endodontic MISHAPSDocument14 pagesEndodontic MISHAPSahmed muhammadNo ratings yet
- Obturation TechniquesDocument111 pagesObturation Techniquesahmed muhammadNo ratings yet
- vital pulp therapy الشرقاويDocument3 pagesvital pulp therapy الشرقاويahmed muhammadNo ratings yet
- EndodonticsDocument206 pagesEndodonticssomebody_ma90% (10)
- Diet and Nutrition in Pediatric Dentistry PDFDocument25 pagesDiet and Nutrition in Pediatric Dentistry PDFpreet sandhuNo ratings yet
- Introduction To Dental Materials - Richard Van NoortDocument299 pagesIntroduction To Dental Materials - Richard Van Noortahmed muhammad100% (1)
- Diagnosdiagnosis 2019Document40 pagesDiagnosdiagnosis 2019ahmed muhammadNo ratings yet
- Art and Science of Operative DentistryDocument699 pagesArt and Science of Operative DentistryPatricia Popescu100% (3)
- العربية بين يديك كتاب الطالب 1 3Document402 pagesالعربية بين يديك كتاب الطالب 1 3ahmed muhammad100% (1)
- 13-SAMSS-003 2017 General Purpose Gear UnitsDocument7 pages13-SAMSS-003 2017 General Purpose Gear UnitsWHWENNo ratings yet
- Dr. P S Adhya 7186Document1 pageDr. P S Adhya 7186Partha AdhyaNo ratings yet
- BergHOFF - серия посуды EssentialsDocument160 pagesBergHOFF - серия посуды EssentialsAntonNo ratings yet
- SAFETY DATA SHEET TECSEL ADHESIVE - Rev 01Document7 pagesSAFETY DATA SHEET TECSEL ADHESIVE - Rev 01Dairo GomezNo ratings yet
- Lwtech HR Management FlyerDocument2 pagesLwtech HR Management FlyerAshlee RouseyNo ratings yet
- Sonotron NDTDocument3 pagesSonotron NDTNour MasmoudiNo ratings yet
- Long Test MILDocument3 pagesLong Test MILBern PabNo ratings yet
- EER WorksheetDocument3 pagesEER WorksheetMichael PoddubnyNo ratings yet
- 3 Novec™ 1230 Fire Protection Fluid Data SheetDocument4 pages3 Novec™ 1230 Fire Protection Fluid Data SheetL ONo ratings yet
- Hygro-Thermometer Pen: User's GuideDocument4 pagesHygro-Thermometer Pen: User's GuideTedosNo ratings yet
- St. Patrick's DayDocument3 pagesSt. Patrick's DayRobin LamNo ratings yet
- Advanced Vehicle Security System: Key To The Programmable WorldDocument40 pagesAdvanced Vehicle Security System: Key To The Programmable WorldTajinder SinghNo ratings yet
- 20 Rules of Parenting (Specific To Mothers)Document2 pages20 Rules of Parenting (Specific To Mothers)Karen KitchellNo ratings yet
- Parte 2 Segundo ParcialDocument23 pagesParte 2 Segundo ParcialJose Luis Rasilla GonzalezNo ratings yet
- Hydraulic Fluids in Mobile Application Re98128 - 2015-06 - Online PDFDocument13 pagesHydraulic Fluids in Mobile Application Re98128 - 2015-06 - Online PDFDennis Huanuco CcamaNo ratings yet
- Technical Manual: Weighing TerminalDocument122 pagesTechnical Manual: Weighing Terminalalfredo morenoNo ratings yet
- Prof Ed6 Intro To MetacognitionDocument83 pagesProf Ed6 Intro To MetacognitionRishane Lolo ListanaNo ratings yet
- 15419Document29 pages15419Sadashiva SahooNo ratings yet
- Reviewer Ansc 111Document6 pagesReviewer Ansc 111Jeric MadroñoNo ratings yet
- Theories of AgingDocument6 pagesTheories of AgingBamba FloresNo ratings yet
- Rundingan Perdagangan Antara Malaysia Dan Indonesia Di Wisma Putra, Kuala Lumpur 1967Document15 pagesRundingan Perdagangan Antara Malaysia Dan Indonesia Di Wisma Putra, Kuala Lumpur 1967nixyingboNo ratings yet
- Chemistry Ssc-I: Answer Sheet No.Document7 pagesChemistry Ssc-I: Answer Sheet No.Mohsin SyedNo ratings yet
- Doctor and Clinical AssistantsDocument2 pagesDoctor and Clinical AssistantsIvan DwiputraNo ratings yet
- GOVT - Departments - Contact - Details - MF-14-06-2021 UpdatedDocument32 pagesGOVT - Departments - Contact - Details - MF-14-06-2021 Updatedadf_raghuNo ratings yet
- Amalgams Qs & AsDocument27 pagesAmalgams Qs & Askaran89No ratings yet
- b2 Open Cloze - EpidemicsDocument3 pagesb2 Open Cloze - EpidemicsJose Manuel Morín BarriosNo ratings yet
- Network Marketing BusinessesDocument1 pageNetwork Marketing BusinessessukhberNo ratings yet
- FLCCC Alliance's I RECOVER Management Protocol For Long Haul COVID 19 SyndromeDocument3 pagesFLCCC Alliance's I RECOVER Management Protocol For Long Haul COVID 19 SyndromeAlan N100% (1)
- Foreign Bodies of Air Passages and Food PassageDocument20 pagesForeign Bodies of Air Passages and Food PassageRamli HassanNo ratings yet
- Basic Counseling SkillsDocument58 pagesBasic Counseling SkillsAnonymous QThGsU93gNo ratings yet