You might also like
- 2022 Annual ReportDocument76 pages2022 Annual ReportLive 5 NewsNo ratings yet
- Health: Quarter 3 - Module 4Document25 pagesHealth: Quarter 3 - Module 4Jervis Roy MendezNo ratings yet
- Can We Induce Lucid Dreams? A Pharmacological Point of ViewDocument14 pagesCan We Induce Lucid Dreams? A Pharmacological Point of ViewAlex NNo ratings yet
- ATEXDocument1 pageATEXmigelNo ratings yet
- REM Lucid Dreaming and Executed Actions LikesDocument8 pagesREM Lucid Dreaming and Executed Actions LikesAdrian ManeaNo ratings yet
- Lucid DreamingDocument11 pagesLucid DreamingMarina AlexopoulouNo ratings yet
- Process RecordingDocument8 pagesProcess RecordingjoanneNo ratings yet
- Theories of Dreaming and Lucid Dreaming: An Integrative Review Towards Sleep, Dreaming and ConsciousnessDocument19 pagesTheories of Dreaming and Lucid Dreaming: An Integrative Review Towards Sleep, Dreaming and ConsciousnessraskoskiNo ratings yet
- Microdream Neurophenomenology: Tore NielsenDocument17 pagesMicrodream Neurophenomenology: Tore NielsenAggelou MayaNo ratings yet
- Paul Schdlich Erlacher 2014 Visual TactileDocument7 pagesPaul Schdlich Erlacher 2014 Visual Tactilehappy crackNo ratings yet
- The Effect of External Stimuli On Dreams, As Assessed Using Q-MethodologyDocument9 pagesThe Effect of External Stimuli On Dreams, As Assessed Using Q-MethodologySuci PrastyaNo ratings yet
- Microdream NeurophenomenologyDocument17 pagesMicrodream NeurophenomenologyPatrik KelemenNo ratings yet
- Aspy Delfabbro Proeveand Mohr 2017Document27 pagesAspy Delfabbro Proeveand Mohr 2017VanNo ratings yet
- 10 1016@j Paid 2004 02 003 PDFDocument11 pages10 1016@j Paid 2004 02 003 PDFMarina AlexopoulouNo ratings yet
- Lucid Dream Research at The Sleep and Dream Laboratory, University of Virginia, Medical CenterDocument3 pagesLucid Dream Research at The Sleep and Dream Laboratory, University of Virginia, Medical CenterАлександр ПожидаевNo ratings yet
- Reasons As To Why People DreamDocument3 pagesReasons As To Why People DreamАзиз ЮлдашевNo ratings yet
- Lecturas. Good Morning Creativity Task Reactivation During Sleepenhances Beneficial Effect of Sleep On Creative PerformanceDocument5 pagesLecturas. Good Morning Creativity Task Reactivation During Sleepenhances Beneficial Effect of Sleep On Creative PerformanceAmets MendiolaNo ratings yet
- Elliott 2014Document5 pagesElliott 2014irnyirnyNo ratings yet
- Induction of Lucid Dreams: A Systematic Review of Evidence: Author NoteDocument57 pagesInduction of Lucid Dreams: A Systematic Review of Evidence: Author NoteIsabel ValdésNo ratings yet
- Information Processing During Sleep: The Effect of Olfactory Stimuli On Dream Content and Dream EmotionsDocument6 pagesInformation Processing During Sleep: The Effect of Olfactory Stimuli On Dream Content and Dream EmotionsMariaNo ratings yet
- The Cognitive Neuroscience of Lucid Dreaming: Try Out and Tell Us What You Think.Document61 pagesThe Cognitive Neuroscience of Lucid Dreaming: Try Out and Tell Us What You Think.Helena QuintNo ratings yet
- Sleep Deprivation Increases Formation of False MemoryDocument10 pagesSleep Deprivation Increases Formation of False MemoryMatheus VilarinhoNo ratings yet
- Running Head: Sleeps Effect On Cognitive Ability 1Document15 pagesRunning Head: Sleeps Effect On Cognitive Ability 1api-302115018No ratings yet
- Sleep Duration Is Associated With White Matter Microstructure and Cognitive Performance in Healthy AdultsDocument9 pagesSleep Duration Is Associated With White Matter Microstructure and Cognitive Performance in Healthy AdultsReynaldy Anggara SaputraNo ratings yet
- Articol PT EvaluareDocument7 pagesArticol PT EvaluareGeorgeta TufisNo ratings yet
- From Pulses To Sleep Stages: Towards Optimized Sleep Classification Using Heart-Rate VariabilityDocument17 pagesFrom Pulses To Sleep Stages: Towards Optimized Sleep Classification Using Heart-Rate Variability葛子骏No ratings yet
- Sleep Medicine Reviews: Michael SchredlDocument7 pagesSleep Medicine Reviews: Michael SchredlAdrienn MatheNo ratings yet
- Schdlich Erlacher 2012 Applications of Lucid Dreams PDFDocument6 pagesSchdlich Erlacher 2012 Applications of Lucid Dreams PDFdetschelNo ratings yet
- Dresler 2012Document4 pagesDresler 2012Andres MardonesNo ratings yet
- Non-Dreamers: J.F. PagelDocument7 pagesNon-Dreamers: J.F. PagelDervilia Compañ CalzadaNo ratings yet
- Jurnal 1Document5 pagesJurnal 1Nia SamahNo ratings yet
- Consciousness and Cognition: Josie E. MalinowskiDocument7 pagesConsciousness and Cognition: Josie E. MalinowskiAdrienn MatheNo ratings yet
- Tetris EffectDocument12 pagesTetris EffectNarendra SiddanNo ratings yet
- Abstracts / Sleep Medicine 40 (2017) E3 Ee185 E174Document1 pageAbstracts / Sleep Medicine 40 (2017) E3 Ee185 E174MariaNo ratings yet
- Beauty Sleep Experimental Study On The Perceived Health and Attractiveness of Sleep Deprived People - The BMJDocument13 pagesBeauty Sleep Experimental Study On The Perceived Health and Attractiveness of Sleep Deprived People - The BMJAdelle Bert DiazNo ratings yet
- Biological ApproachDocument7 pagesBiological ApproachridaNo ratings yet
- 3389 PDFDocument6 pages3389 PDFvarun sahaniNo ratings yet
- DementDocument2 pagesDementHamnah Malick 2253294No ratings yet
- Pengukuran Kualitas TidurDocument8 pagesPengukuran Kualitas TidurmllnaekaaNo ratings yet
- (Re-) Mapping The Concept of DreamingDocument5 pages(Re-) Mapping The Concept of DreamingEduardo VLNo ratings yet
- The Lucid Dreaming Playbook - How To Take Charge of Your Dreams - Aeon IdeasDocument3 pagesThe Lucid Dreaming Playbook - How To Take Charge of Your Dreams - Aeon IdeasBlazing BooksNo ratings yet
- Pupil Dilation During Visual Target DetectionDocument14 pagesPupil Dilation During Visual Target DetectionShane G MoonNo ratings yet
- Effects of Red Light On Sleep InertiaDocument13 pagesEffects of Red Light On Sleep InertiaMonica SaavedraNo ratings yet
- Lab 601 Group 1Document13 pagesLab 601 Group 1Clemente Abines IIINo ratings yet
- Pairing Journal Review SHMY1013Document15 pagesPairing Journal Review SHMY1013sp-hazaranaz.mohdaslamNo ratings yet
- 2019 - AJA-19-0026 FaltaDocument10 pages2019 - AJA-19-0026 FaltaLuis Fernando GarciaNo ratings yet
- Lucid Dreaming in NarcolepsyDocument11 pagesLucid Dreaming in NarcolepsyPAOLA MU�OZ PEREIRANo ratings yet
- Dreaming Memory Consolidation Wamsley 2014Document7 pagesDreaming Memory Consolidation Wamsley 2014jenniferNo ratings yet
- Beauty Sleep - A ResearchDocument10 pagesBeauty Sleep - A ResearchKyleigh SaculingganNo ratings yet
- Baird MotaRolim Dresler - Lucid DreamingDocument69 pagesBaird MotaRolim Dresler - Lucid DreamingAnonymous IZJqiRv0oKNo ratings yet
- Palinkas - 2017 - Nocturnal Sleep Architecture Is Altered by Sleep BruxismDocument5 pagesPalinkas - 2017 - Nocturnal Sleep Architecture Is Altered by Sleep Bruxismcarolina marpaungNo ratings yet
- Nihms-1525230 Lucid DreamingDocument48 pagesNihms-1525230 Lucid DreamingJosé Francisco Muñoz SilvaNo ratings yet
- Dream Recall Frequency and Content in Patients With Temporal Lobe EpilepsyDocument6 pagesDream Recall Frequency and Content in Patients With Temporal Lobe EpilepsyAnonymous zxTFUoqzklNo ratings yet
- Abstracts / Sleep Medicine 64 (2019) S1 Es359 S237Document1 pageAbstracts / Sleep Medicine 64 (2019) S1 Es359 S237Pedro AmorimNo ratings yet
- Psychology All Case Studies PDFDocument54 pagesPsychology All Case Studies PDFArmeen AmirNo ratings yet
- A Laboratory Approach To The Nocturnal 1969 PDFDocument15 pagesA Laboratory Approach To The Nocturnal 1969 PDFVitor Moura VisoniNo ratings yet
- Askay-Virtual Reality HypnosisDocument8 pagesAskay-Virtual Reality HypnosisClaudio Alonso MoyNo ratings yet
- Mallett Et Al 2022 PDFDocument14 pagesMallett Et Al 2022 PDFJarrod GottNo ratings yet
- Dreaming During Non-Rapid Eye Movement Sleep in The Absence of Prior Rapid Eye Movement SleepDocument5 pagesDreaming During Non-Rapid Eye Movement Sleep in The Absence of Prior Rapid Eye Movement SleepRizmu HandijayaNo ratings yet
- Short Sleep - Poor Sleep? A Polysomnographic Study in A Large Population Based Sample of WomenDocument7 pagesShort Sleep - Poor Sleep? A Polysomnographic Study in A Large Population Based Sample of Womenmahfuz emonNo ratings yet
- Sleepless in America: Inadequate Sleep and Relationships To Health and Well-Being of Our Nation's ChildrenDocument18 pagesSleepless in America: Inadequate Sleep and Relationships To Health and Well-Being of Our Nation's ChildrenDavid SzNo ratings yet
- A Comparative Review On Sleep Stage Classification MethodsDocument19 pagesA Comparative Review On Sleep Stage Classification MethodsVy Tô Nguyễn TườngNo ratings yet
- Multisensorial StrokeDocument11 pagesMultisensorial StrokeAlbaNo ratings yet
- Congenital CataractDocument20 pagesCongenital CataractYouhengNo ratings yet
- National Rehabilitation Strategic Plan (2020-2024) - English (REVISED)Document44 pagesNational Rehabilitation Strategic Plan (2020-2024) - English (REVISED)Sergio CurteanNo ratings yet
- Nurse Manager CompetenciesDocument8 pagesNurse Manager Competenciessd pilar bangsaNo ratings yet
- General Nursing and MidwiferyDocument4 pagesGeneral Nursing and MidwiferyBALAJI INSTITUTENo ratings yet
- People v. Opuran, G.R. Nos. 147674-75, 17 March 2004Document6 pagesPeople v. Opuran, G.R. Nos. 147674-75, 17 March 2004Anna BarbadilloNo ratings yet
- Bs 120 PDFDocument3 pagesBs 120 PDFPaa Kwesi XCelNo ratings yet
- Dissertation Ideas DrugsDocument6 pagesDissertation Ideas DrugsBuyPapersOnlineForCollegeUK100% (1)
- Group 4 Gastro Intestinal Complications of The NewbornDocument20 pagesGroup 4 Gastro Intestinal Complications of The NewbornCHARLOTTE DU PREEZNo ratings yet
- Rama College of Nursing: Health Education OnDocument24 pagesRama College of Nursing: Health Education OnBrijesh Yadav100% (1)
- Perspective: New England Journal MedicineDocument3 pagesPerspective: New England Journal MedicinePatrick CommettantNo ratings yet
- Detail Studies of Mango Qualitative Production, Its Marketing and Mango Processing Industry in Uttar PradeshDocument156 pagesDetail Studies of Mango Qualitative Production, Its Marketing and Mango Processing Industry in Uttar PradeshPriety Verma91% (11)
- COVID-19 Source Book: Third EditionDocument64 pagesCOVID-19 Source Book: Third EditionNikolaos GonosNo ratings yet
- Adoc - Pub - Arikunto S 2010 Prosedur Penelitian Rev Ed JakartaDocument5 pagesAdoc - Pub - Arikunto S 2010 Prosedur Penelitian Rev Ed JakartaResa Eni Santi WulandariNo ratings yet
- Vaporesso XROS 3 User Manual A1 20221102Document33 pagesVaporesso XROS 3 User Manual A1 20221102EnricoNo ratings yet
- Mental HealthDocument58 pagesMental HealthKshitij MauryaNo ratings yet
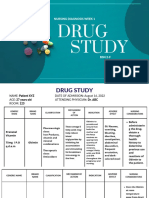
- Study: Nursing Diagnosis Week 1Document9 pagesStudy: Nursing Diagnosis Week 122 - Fernandez, Lyza Mae D.No ratings yet
- Memorandum of AgreementDocument2 pagesMemorandum of Agreementbhagzc khuya100% (1)
- Dental Anxiety Prediction Using Venham Picture Test A Preliminary Cross-Sectional StudyDocument5 pagesDental Anxiety Prediction Using Venham Picture Test A Preliminary Cross-Sectional StudyDeska PertiwiNo ratings yet
- Test Bank For Biology of Aging 1st by McdonaldDocument6 pagesTest Bank For Biology of Aging 1st by McdonaldThomas Bila100% (25)
- Agro Power Energy MSDS 1Document3 pagesAgro Power Energy MSDS 1Om RanjanNo ratings yet
- Royal Government of Bhutan Jigme Dorji Wangchuk National Referral Hospital Patient Discharge FormDocument1 pageRoyal Government of Bhutan Jigme Dorji Wangchuk National Referral Hospital Patient Discharge FormSuman Pradhan 2803No ratings yet
- Kecanduan Internet Gaming Dan Status Body Mass Index (BMI) Pada Remaja Tingkat Sekolah Menengah Pertama Tahun 2018Document8 pagesKecanduan Internet Gaming Dan Status Body Mass Index (BMI) Pada Remaja Tingkat Sekolah Menengah Pertama Tahun 2018Hanum PramestiNo ratings yet
- World Journal of Surgical OncologyDocument4 pagesWorld Journal of Surgical OncologyWa Ode Nur AsrawatiNo ratings yet
- Managerial Skill Development Unit-3Document44 pagesManagerial Skill Development Unit-3Arif QuadriNo ratings yet
- Journal of Arts Science and Technology - JAST - Vol. 14 - No. 1 March 2022Document178 pagesJournal of Arts Science and Technology - JAST - Vol. 14 - No. 1 March 2022Akinlabi HendricksNo ratings yet
- Neurology 1.03 Approach To Cerebral Function - Dr. MartinezDocument7 pagesNeurology 1.03 Approach To Cerebral Function - Dr. MartinezDeomicah SolanoNo ratings yet